Successful Endoscopic Ultrasound-Guided Treatment of a Spontaneous Rupture of a Hemorrhagic Pancreatic Pseudocyst
- Affiliations
-
- 1Department of Surgery, Wonkwang University College of Medicine and Hospital, Iksan, Korea
- 2Department of Internal Medicine, Wonkwang University College of Medicine and Hospital, Iksan, Korea
- KMID: 2520562
- DOI: http://doi.org/10.5946/ce.2020.279
Abstract
- Spontaneous rupture of a hemorrhagic pancreatic pseudocyst may be life-threatening. Endoscopic ultrasound (EUS)-guided drainage has been reported to be a valuable treatment option for pancreatic pseudocysts. However, its usefulness in the management of a ruptured pancreatic pseudocyst is limited. We report a rare case of a spontaneous rupture of a hemorrhagic pancreatic pseudocyst in a patient with chronic pancreatitis, which was successfully treated with EUS-guided gastrocystostomy with a fully covered self-expandable metallic stent.
Figure
-

Fig. 1. (A) Axial T2-weighted magnetic resonance imaging showing the main pancreatic duct dilation (open black arrow) with multiple pancreatoliths (black arrowheads) and a pseudocyst (open white arrow), about 9 cm in size, in the pancreatic tail. Abdominal computed tomography scan of a hemorrhagic pancreatic pseudocyst that ruptured spontaneously. (B) Axial and (C) coronal views showing mural discontinuity (black arrows) of the hemorrhagic pancreatic pseudocyst (asterisks), extension of fluid into the perisplenic space (white arrows), and multiple main pancreatic duct stones with pancreatic atrophy.
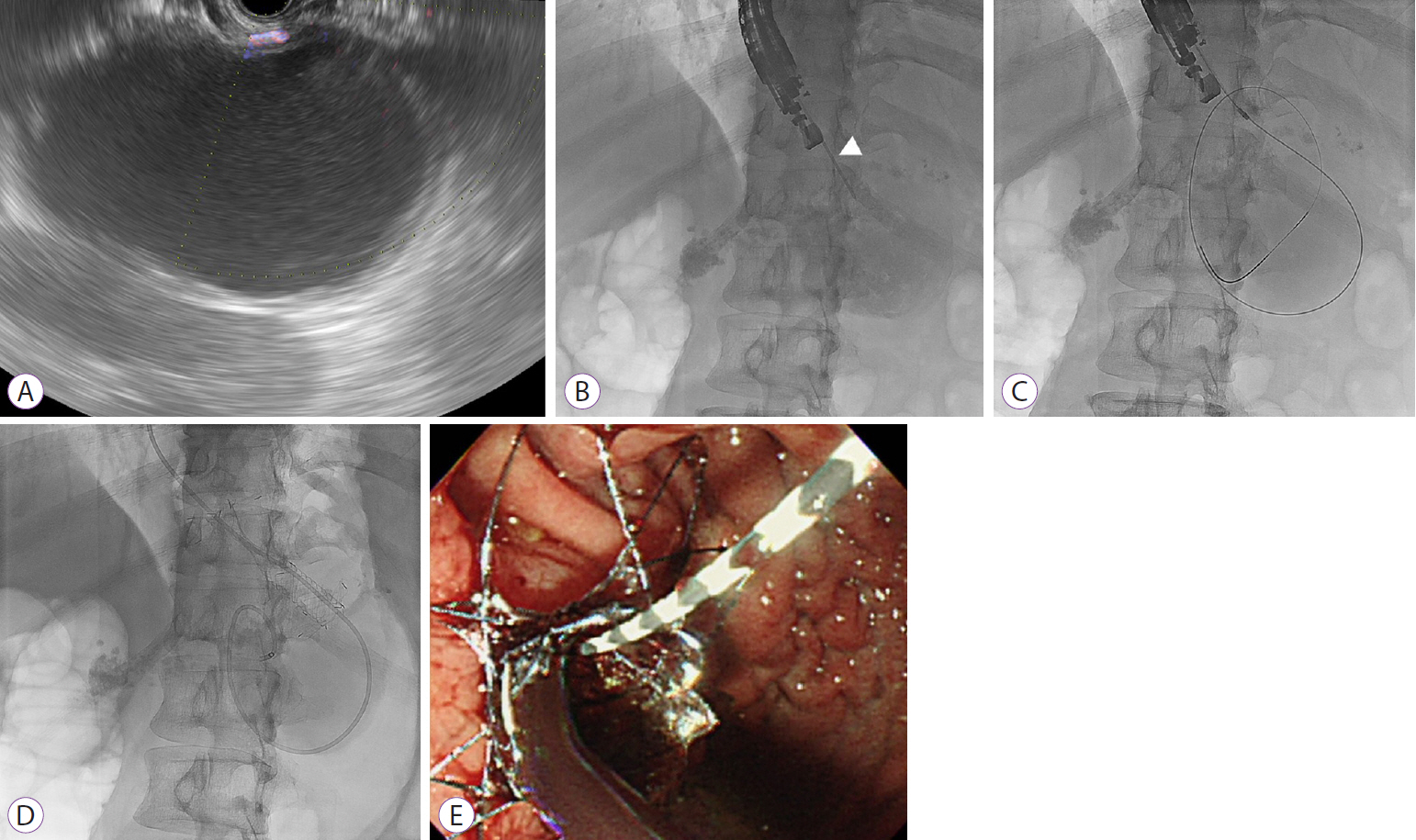
Fig. 2. Endoscopic ultrasound-guided gastrocystostomy. (A) Large anechoic cystic lesion with hyperechoic material on endoscopic ultrasound, (B) The pseudocyst was punctured with a 19-gauge needle for fine-needle aspiration (white arrowhead). (C) Passage of a 0.025-inch guidewire under fluoroscopic guidance, (D) Placement of a metal stent with a nasocystic drainage tube, and (E) Endoscopic view showing gushing thick and turbid bloody fluid gushing out, and the presence of the metal stent.

Fig. 3. Abdominal computed tomography scan showing complete resolution of the ruptured pancreatic pseudocyst with the metal stent (black arrow) on axial (A) and coronal (B) views.
Reference
-
1. Song TJ, Lee SS. Endoscopic drainage of pseudocysts. Clin Endosc. 2014; 47:222–226.
Article2. Habashi S, Draganov PV. Pancreatic pseudocyst. World J Gastroenterol. 2009; 15:38–47.
Article3. Urakami A, Tsunoda T, Kubozoe T, Takeo T, Yamashita K, Imai H. Rupture of a bleeding pancreatic pseudocyst into the stomach. J Hepatobiliary Pancreat Surg. 2002; 9:383–385.
Article4. Hiraishi H, Terano A. Images in clinical medicine. Rupture of a pancreatic pseudocyst into the duodenum. N Engl J Med. 1999; 340:1411.5. Rocha R, Marinho R, Gomes A, et al. Spontaneous rupture of pancreatic pseudocyst: report of two cases. Case Rep Surg. 2016; 2016:7056567.
Article6. Patidar Y, Sureka B, Singh VP, Bansal K, Maiwall R. Spontaneous rupture of intrahepatic pseudocyst into the inferior vena cava. Gastroenterol Rep (Oxf). 2018; 6:225–227.
Article7. Mujer MT, Rai MP, Atti V, Shrotriya S. Spontaneous rupture of a pancreatic pseudocyst. BMJ Case Rep. 2018; 2018:bcr2018226296.
Article8. Alali A, Mosko J, May G, Teshima C. Endoscopic ultrasound-guided management of pancreatic fluid collections: update and review of the literature. Clin Endosc. 2017; 50:117–125.
Article9. Bang JY, Varadarajulu S. Metal versus plastic stent for transmural drainage of pancreatic fluid collections. Clin Endosc. 2013; 46:500–502.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Linear Array Endoscopic Ultrasound-Guided Drainage of a Pancreatic Pseudocyst without Using Fluoroscopy
- Endoscopic Ultrasound-Guided Drainage of Pancreatic Fluid Collections (with Video)
- A Case of Cystoduodenal and Cystocolic Fistula Complicated in Pancreatic Pseudocyst
- Angiographic diagnosis and treatment of a splenic artery pseudoaneurysm following endoscopic cystogastrostomy for a pancreatic pseudocyst
- Endoscopic Ultrasound-Guided Transesophageal Drainage of a Mediastinal Pancreatic Pseudocyst
