Cracking Difficult Biliary Stones
- Affiliations
-
- 1Department of Anatomy, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Bangkok, Thailand
- 2Division of Gastroenterology, Department of Medicine, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Bangkok, Thailand
- 3Center of Excellence for Innovation and Endoscopy in Gastrointestinal Oncology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
- KMID: 2520548
- DOI: http://doi.org/10.5946/ce.2020.256-IDEN
Abstract
- Apart from difficult biliary cannulation, biliary stone removal is considered one of the hurdles in endoscopic retrograde cholangiopancreatography. Generally, simple common bile duct (CBD) stones can be removed either with an extraction balloon or a basket. However, there are difficult stones that cannot be removed using these standard methods. The most difficult stones are large CBD stones and impacted stones in a tapering CBD. A few decades ago, mechanical lithotripsy was usually required to manage these stones. At present, endoscopic papillary large balloon dilation (EPLBD) of the biliary orifice has become the gold standard for large CBD stones up to 1.5 cm. EPLBD can reduce the procedural time by shortening the stone removal process. It can also save the cost of the devices, especially multiple baskets, used in mechanical lithotripsy. Unfortunately, very large CBD stones, stones impacted in a tapering CBD, and some intrahepatic duct stones still require lithotripsy. Peroral cholangioscopy provides direct visualization of the stone, which helps the endoscopist perform a probe-based lithotripsy either with an electrohydraulic probe or a laser probe. This technique can facilitate the management of difficult CBD stones with a high success rate and save procedural time without significant technical complications.
Keyword
Figure
-
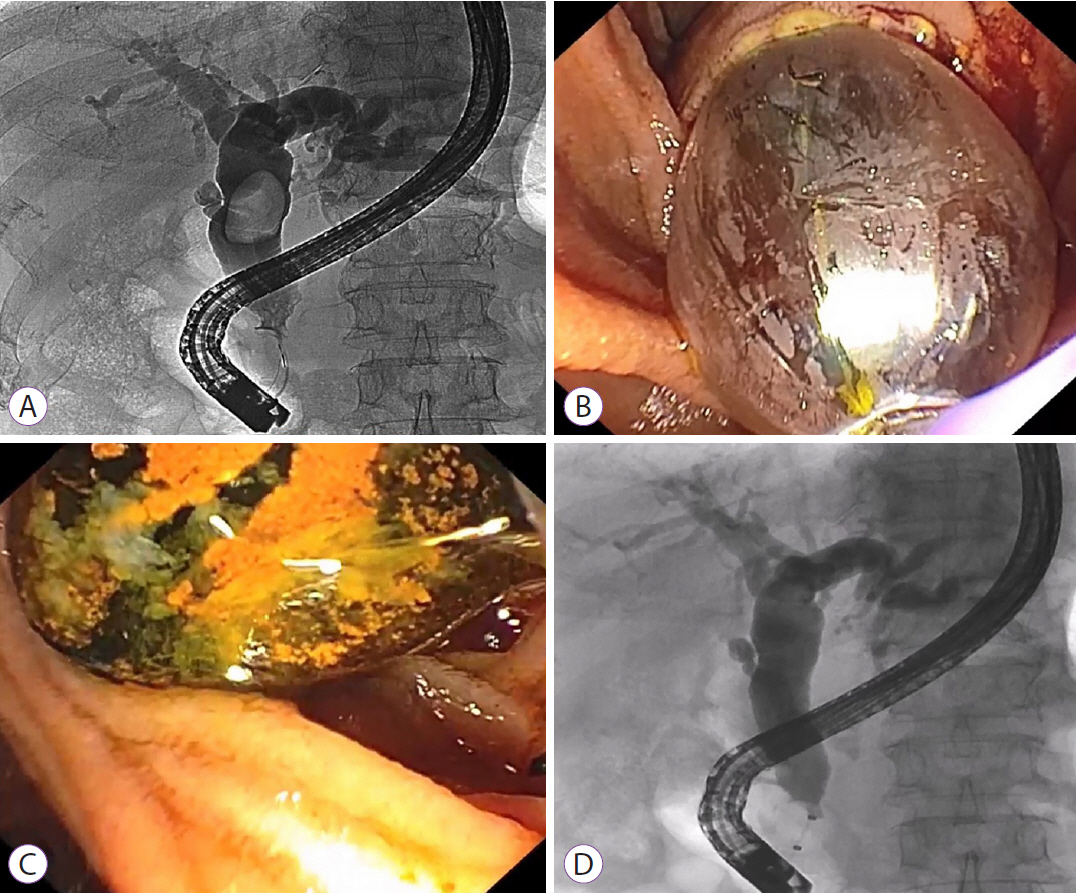
Fig. 1. A large bile duct stone successfully treated with endoscopic papillary large balloon dilation (EPLBD). (A) Cholangiogram showing a large bile duct stone. (B) Endoscopic view of EPLBD after sphincterotomy. (C) A large stone removed with an extraction balloon. (D) Occlusion cholangiogram showing no residual filling defect.
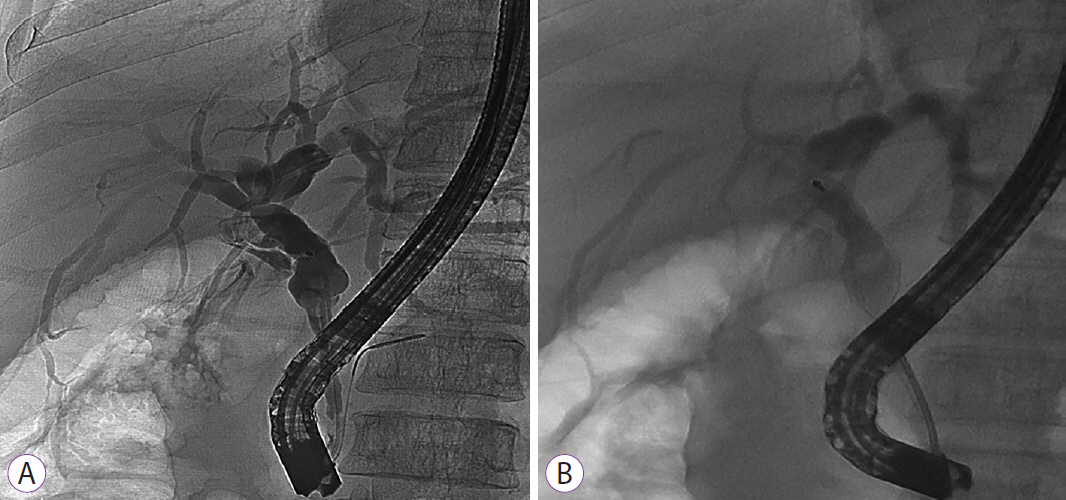
Fig. 2. Mechanical lithotripsy for a difficult bile duct stone. (A) A 1-cm stone proximal to a considerably tapered bile duct. (B) Mechanical lithotripsy was successfully performed using a through-the-scope mechanical lithotripter, and stone clearance was achieved.

Fig. 3. Laser lithotripsy guided by single-operator cholangioscopy. (A) A disposable cholangioscope operated by a single endoscopist. The laser probe is inserted through the accessory channel of the cholangioscope, which is inserted through the accessory channel of the duodenoscope. (B) Cholangioscopic view of intraductal stone fragmentation with a laser probe.
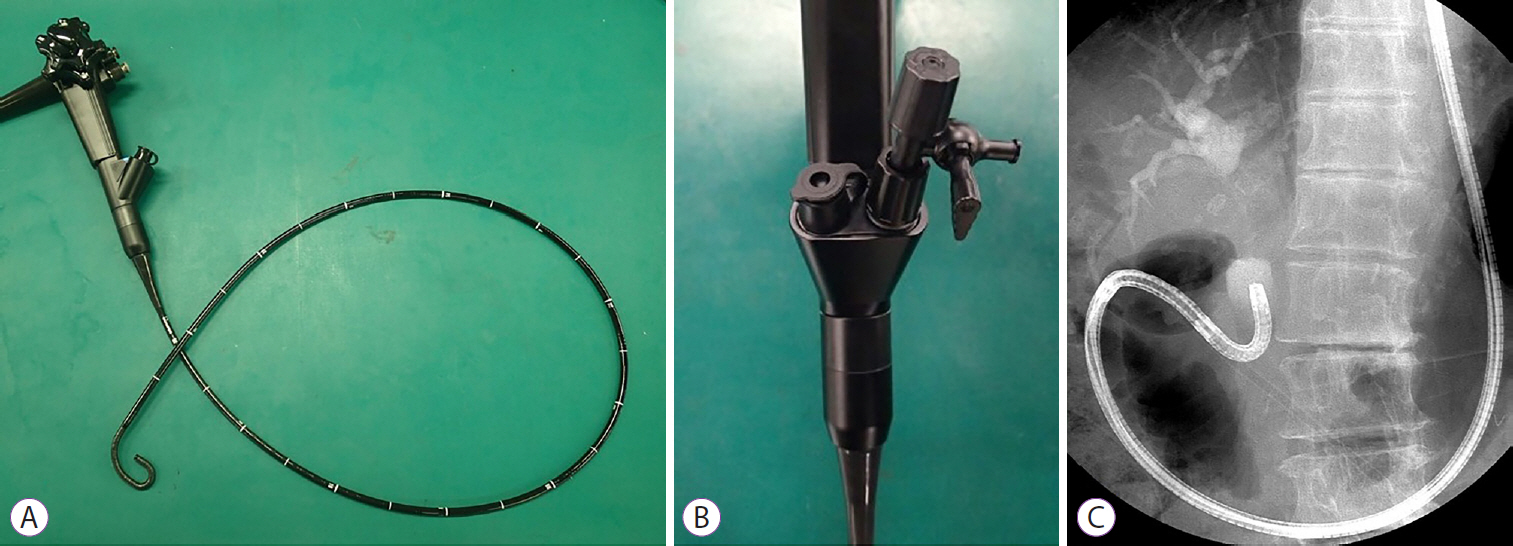
Fig. 4. Prototype of a mutibending ultra-slim scope. (A) The distal end has two bending sections for facilitating biliary insertion. (B) Two accessory channels (2.2 and 1 mm) designed to facilitate irrigation during intraductal lithotripsy. (C) Free-hand bile duct insertion of the scope. (Picture courtesy of Prof. Jong H. Moon, MD, PhD, FASGE, FJGES, Director of Digestive Disease Center, SoonChunHyang University School of Medicine, Bucheon/Seoul, Korea).
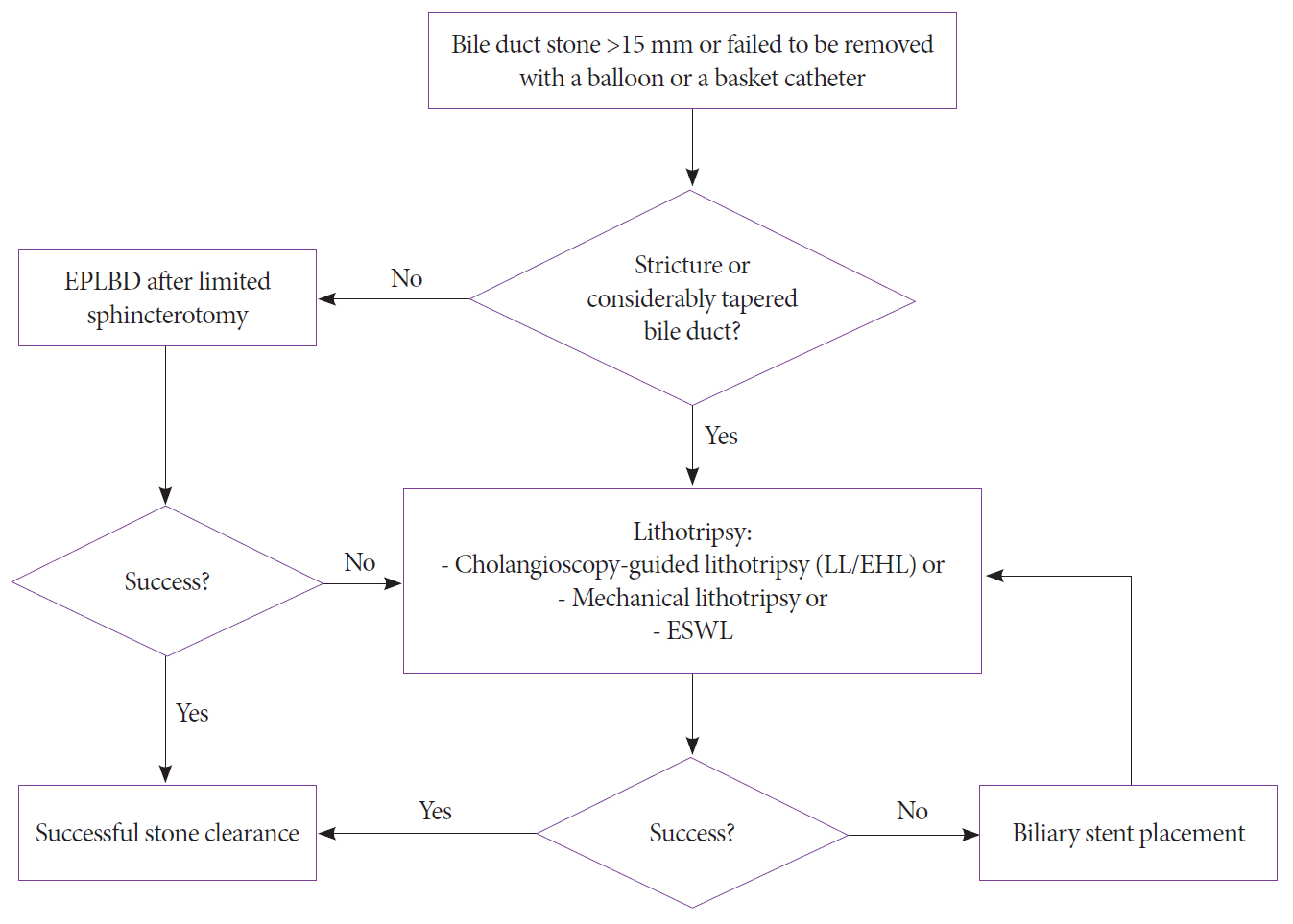
Fig. 5. Recommendation for the management of difficult bile duct stones.
Reference
-
1. Classen M, Demling L. [Endoscopic sphincterotomy of the papilla of vater and extraction of stones from the choledochal duct (author’s transl)]. Dtsch Med Wochenschr. 1974; 99:496–497.2. Kawai K, Akasaka Y, Murakami K, Tada M, Koli Y. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc. 1974; 20:148–151.
Article3. McHenry L, Lehman G. Difficult bile duct stones. Curr Treat Options Gastroenterol. 2006; 9:123–132.
Article4. Manes G, Paspatis G, Aabakken L, et al. Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019; 51:472–491.
Article5. Madhoun MF, Wani S, Hong S, Tierney WM, Maple JT. Endoscopic papillary large balloon dilation reduces the need for mechanical lithotripsy in patients with large bile duct stones: a systematic review and meta-analysis. Diagn Ther Endosc. 2014; 2014:309618.
Article6. ASGE Standards of Practice Committee, Buxbaum JL, Abbas Fehmi SM, et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest Endosc. 2019; 89:1075–1105.e15.
Article7. Kim TH, Kim JH, Seo DW, et al. International consensus guidelines for endoscopic papillary large-balloon dilation. Gastrointest Endosc. 2016; 83:37–47.
Article8. Matsubayashi CO, Ribeiro IB, de Moura DTH, et al. Is endoscopic balloon dilation still associated with higher rates of pancreatitis?: a systematic review and meta-analysis. Pancreas. 2020; 49:158–174.9. Angsuwatcharakon P, Kulpatcharapong S, Ridtitid W, et al. Digital cholangioscopy-guided laser versus mechanical lithotripsy for large bile duct stone removal after failed papillary large-balloon dilation: a randomized study. Endoscopy. 2019; 51:1066–1073.
Article10. Franzini T, Moura RN, Bonifácio P, et al. Complex biliary stones management: cholangioscopy versus papillary large balloon dilation - a randomized controlled trial. Endosc Int Open. 2018; 6:E131–E138.
Article11. Bang JY, Sutton B, Navaneethan U, Hawes R, Varadarajulu S. Efficacy of single-operator cholangioscopy-guided lithotripsy compared with large balloon sphincteroplasty in management of difficult bile duct stones in a randomized trial. Clin Gastroenterol Hepatol. 2020; 18:2349–2356.e3.12. Demling L, Seuberth K, Riemann JF. A mechanical lithotripter. Endoscopy. 1982; 14:100–101.
Article13. Siegel JH, Ben-Zvi JS, Pullano WE. Mechanical lithotripsy of common duct stones. Gastrointest Endosc. 1990; 36:351–356.
Article14. Schutz SM, Chinea C, Friedrichs P. Successful endoscopic removal of a severed, impacted Dormia basket. Am J Gastroenterol. 1997; 92:679–681.15. Riemann JF, Seuberth K, Demling L. Clinical application of a new mechanical lithotripter for smashing common bile duct stones. Endoscopy. 1982; 14:226–230.
Article16. Garg PK, Tandon RK, Ahuja V, Makharia GK, Batra Y. Predictors of unsuccessful mechanical lithotripsy and endoscopic clearance of large bile duct stones. Gastrointest Endosc. 2004; 59:601–605.
Article17. Schneider MU, Matek W, Bauer R, Domschke W. Mechanical lithotripsy of bile duct stones in 209 patients--effect of technical advances. Endoscopy. 1988; 20:248–253.
Article18. Chung SC, Leung JW, Leong HT, Li AK. Mechanical lithotripsy of large common bile duct stones using a basket. Br J Surg. 1991; 78:1448–1450.
Article19. Cipolletta L, Costamagna G, Bianco MA, et al. Endoscopic mechanical lithotripsy of difficult common bile duct stones. Br J Surg. 1997; 84:1407–1409.
Article20. Chang WH, Chu CH, Wang TE, Chen MJ, Lin CC. Outcome of simple use of mechanical lithotripsy of difficult common bile duct stones. World J Gastroenterol. 2005; 11:593–596.
Article21. Shaw MJ, Mackie RD, Moore JP, et al. Results of a multicenter trial using a mechanical lithotripter for the treatment of large bile duct stones. Am J Gastroenterol. 1993; 88:730–733.22. Thomas M, Howell DA, Carr-Locke D, et al. Mechanical lithotripsy of pancreatic and biliary stones: complications and available treatment options collected from expert centers. Am J Gastroenterol. 2007; 102:1896–1902.
Article23. Koch H, Stolte M, Walz V. Endoscopic lithotripsy in the common bile duct. Endoscopy. 1977; 9:95–98.
Article24. Lux G, Ell C, Hochberger J, Müller D, Demling L. The first successful endoscopic retrograde laser lithotripsy of common bile duct stones in man using a pulsed neodymium-YAG laser. Endoscopy. 1986; 18:144–145.
Article25. Shim CS, Neuhaus H, Tamada K. Direct cholangioscopy. Endoscopy. 2003; 35:752–758.
Article26. Chen YK, Pleskow DK. SpyGlass single-operator peroral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video). Gastrointest Endosc. 2007; 65:832–841.
Article27. McCarty TR, Gulati R, Rustagi T. Efficacy and safety of peroral cholangioscopy with intraductal lithotripsy for difficult biliary stones: a systematic review and meta-analysis. Endoscopy. 2021; 53:110–122.
Article28. Maydeo AP, Rerknimitr R, Lau JY, et al. Cholangioscopy-guided lithotripsy for difficult bile duct stone clearance in a single session of ERCP: results from a large multinational registry demonstrate high success rates. Endoscopy. 2019; 51:922–929.
Article29. Buxbaum J, Sahakian A, Ko C, et al. Randomized trial of cholangioscopy-guided laser lithotripsy versus conventional therapy for large bile duct stones (with videos). Gastrointest Endosc. 2018; 87:1050–1060.30. Li G, Pang Q, Zhai H, et al. SpyGlass-guided laser lithotripsy versus laparoscopic common bile duct exploration for large common bile duct stones: a non-inferiority trial. Surg Endosc. 2021; 35:3723–3731.
Article31. Deprez PH, Garces Duran R, Moreels T, et al. The economic impact of using single-operator cholangioscopy for the treatment of difficult bile duct stones and diagnosis of indeterminate bile duct strictures. Endoscopy. 2018; 50:109–118.
Article32. Larghi A, Waxman I. Endoscopic direct cholangioscopy by using an ultra-slim upper endoscope: a feasibility study. Gastrointest Endosc. 2006; 63:853–857.
Article33. Moon JH, Ko BM, Choi HJ, et al. Intraductal balloon-guided direct peroral cholangioscopy with an ultraslim upper endoscope (with videos). Gastrointest Endosc. 2009; 70:297–302.
Article34. Choi HJ, Moon JH, Ko BM, et al. Overtube-balloon-assisted direct peroral cholangioscopy by using an ultra-slim upper endoscope (with videos). Gastrointest Endosc. 2009; 69:935–940.
Article35. Lee YN, Moon JH, Lee TH, et al. Prospective randomized trial of a new multibending versus conventional ultra-slim endoscope for peroral cholangioscopy without device or endoscope assistance (with video). Gastrointest Endosc. 2020; 91:92–101.
Article36. Kim HI, Moon JH, Choi HJ, et al. Holmium laser lithotripsy under direct peroral cholangioscopy by using an ultra-slim upper endoscope for patients with retained bile duct stones (with video). Gastrointest Endosc. 2011; 74:1127–1132.
Article37. Moon JH, Ko BM, Choi HJ, et al. Direct peroral cholangioscopy using an ultra-slim upper endoscope for the treatment of retained bile duct stones. Am J Gastroenterol. 2009; 104:2729–2733.
Article38. Lee TY, Cheon YK, Choe WH, Shim CS. Direct cholangioscopy-based holmium laser lithotripsy of difficult bile duct stones by using an ultrathin upper endoscope without a separate biliary irrigating catheter. Photomed Laser Surg. 2012; 30:31–36.
Article39. Paramasivam RK, Angsuwatcharakon P, Soontornmanokul T, Rerknimitr R. Management of endoscopic complications, in particular perforation. Dig Endosc. 2013; 25 Suppl 2:132–136.
Article40. Efthymiou M, Raftopoulos S, Antonio Chirinos J, May GR. Air embolism complicated by left hemiparesis after direct cholangioscopy with an intraductal balloon anchoring system. Gastrointest Endosc. 2012; 75:221–223.
Article41. Bland KI, Jones RS, Maher JW, et al. Extracorporeal shock-wave lithotripsy of bile duct calculi. An interim report of the Dornier U.S. bile duct lithotripsy prospective study. Ann Surg. 1989; 209:743–753. discussion 753-755.42. Sauerbruch T, Delius M, Paumgartner G, et al. Fragmentation of gallstones by extracorporeal shock waves. N Engl J Med. 1986; 314:818–822.
Article43. Tandan M, Reddy DN, Santosh D, et al. Extracorporeal shock wave lithotripsy of large difficult common bile duct stones: efficacy and analysis of factors that favor stone fragmentation. J Gastroenterol Hepatol. 2009; 24:1370–1374.
Article44. Amplatz S, Piazzi L, Felder M, et al. Extracorporeal shock wave lithotripsy for clearance of refractory bile duct stones. Dig Liver Dis. 2007; 39:267–272.
Article45. Neuhaus H, Zillinger C, Born P, et al. Randomized study of intracorporeal laser lithotripsy versus extracorporeal shock-wave lithotripsy for difficult bile duct stones. Gastrointest Endosc. 1998; 47:327–334.
Article46. Chopra KB, Peters RA, O’Toole PA, et al. Randomised study of endoscopic biliary endoprosthesis versus duct clearance for bileduct stones in high-risk patients. Lancet. 1996; 348:791–793.
Article47. Di Giorgio P, Manes G, Grimaldi E, et al. Endoscopic plastic stenting for bile duct stones: stent changing on demand or every 3 months. A prospective comparison study. Endoscopy. 2013; 45:1014–1017.
Article48. Jang DK, Lee SH, Ahn DW, et al. Factors associated with complete clearance of difficult common bile duct stones after temporary biliary stenting followed by a second ERCP: a multicenter, retrospective, cohort study. Endoscopy. 2020; 52:462–468.
Article49. Lee TH, Han JH, Kim HJ, Park SM, Park SH, Kim SJ. Is the addition of choleretic agents in multiple double-pigtail biliary stents effective for difficult common bile duct stones in elderly patients? A prospective, multicenter study. Gastrointest Endosc. 2011; 74:96–102.
Article50. Hartery K, Lee CS, Doherty GA, et al. Covered self-expanding metal stents for the management of common bile duct stones. Gastrointest Endosc. 2017; 85:181–186.
Article51. Cerefice M, Sauer B, Javaid M, et al. Complex biliary stones: treatment with removable self-expandable metal stents: a new approach (with videos). Gastrointest Endosc. 2011; 74:520–526.
Article52. Huang C, Cai XB, Guo LL, Qi XS, Gao Q, Wan XJ. Drug-eluting fully covered self-expanding metal stent for dissolution of bile duct stones in vitro. World J Gastroenterol. 2019; 25:3370–3379.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous transheptic removal of biliary stones:clinical analysis of 16 cases
- When the Going Gets Tough: Utilization of SpyGlass, or Drainage Followed by Stone Removal
- Application of Electrohydraulic Lithotripsy for Bile Duct Stones Difficult to Remove
- Percutaneous removal of residual biliary tract stones: review of 43 cases
- Biliary stones: comparative study with sonography and ERCP
