The Effect of Smoking on the Outcomes of Vascularized Bone Graft Surgery in Scaphoid Nonunion through Meta-analysis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Uijeongbu Eulji Medical Center, Eulji University School of Medicine, Uijeongbu, Korea
- KMID: 2519466
- DOI: http://doi.org/10.12790/ahm.21.0106
Abstract
- Purpose
A vascularized bone graft is an option showing a good result to treat scaphoid nonunion. The analysis of the effects of smoking, which affects vascular and union of fracture, has been limited. We tried to analyze the effect of smoking on the outcomes of vascularized bone graft in scaphoid nonunion through meta-analysis
Methods
Two researchers analyzed 923 papers searched for ‘scaphoid AND (vascularized OR vascularised OR flap OR pedicled)’ on MEDLINE and Embase (until November 2020). We selected 31 papers which contain that vascularized bone graft was performed for scaphoid nonunion, and the number or proportion of smokers could be confirmed. Through meta-regression analysis and subgroup analysis, whether the smoker’s rate had an effect on union rate, union period, functional score, imaging evaluation, range of motion, and complications rate was analyzed
Results
A significant negative correlation between smoking and bone union rate was confirmed in pedicled vascularized bone grafting, and a significant positive correlation between smoking and bone union duration was confirmed in free vascularized bone grafting.
Conclusion
It is necessary to have caution for nonunion when considering pedicled vascularized bone graft in smoking patients with scaphoid nonunion.
Keyword
Figure
-

Fig. 1. (A) Thirty-one studies were finally enrolled following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) guidelines. (B) The risk of bias was assessed by RoBANS (Risk of Bias Assessment tool for Non-randomized Study). Enrolled studies were measured unclear risk of bias in the measurement of exposure and confounding variables.

Fig. 2. (A) The union rate of vascularized bone graft in 908 patients (31 studies for scaphoid nonunion) was announced from 27.3% to 100%. Average of the union rate was analyzed as 82.1% (95% confidence interval [CI], 0.77–0.86). (B) The funnel plot showed asymmetry which suggests the existence of publication bias.
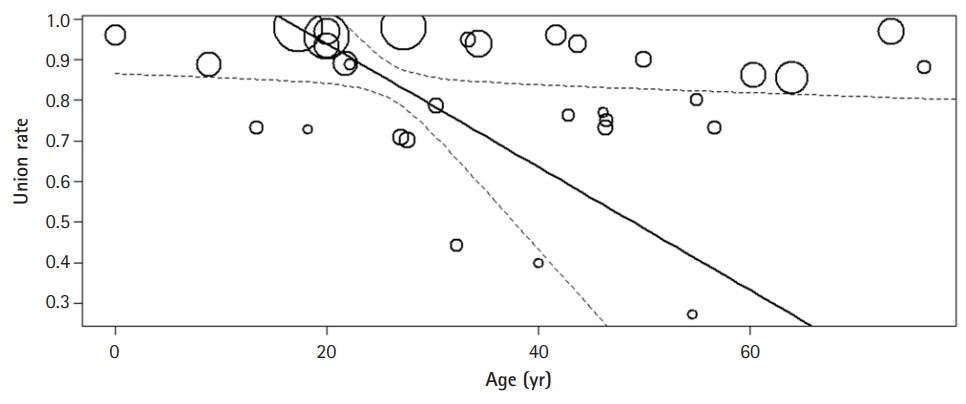
Fig. 3. The correlation of age and the union rate showed a negative correlation (correlation coefficient [r]=–0.0151 95% confidence interval, –0.0294 to –0.0008) in that union rate decreased with older age.

Fig. 4. (A) In the subgroup analysis of free vascularized bone graft, the correlation of smoking rate and the bone union period showed a positive correlation (correlation coefficient, 0.8581; 95% confidence interval [CI], 0.4561–1.2601). (B) The average union rate was analyzed as 87.3% (95% CI, 0.80–0.92) in the free vascularized bone graft group.
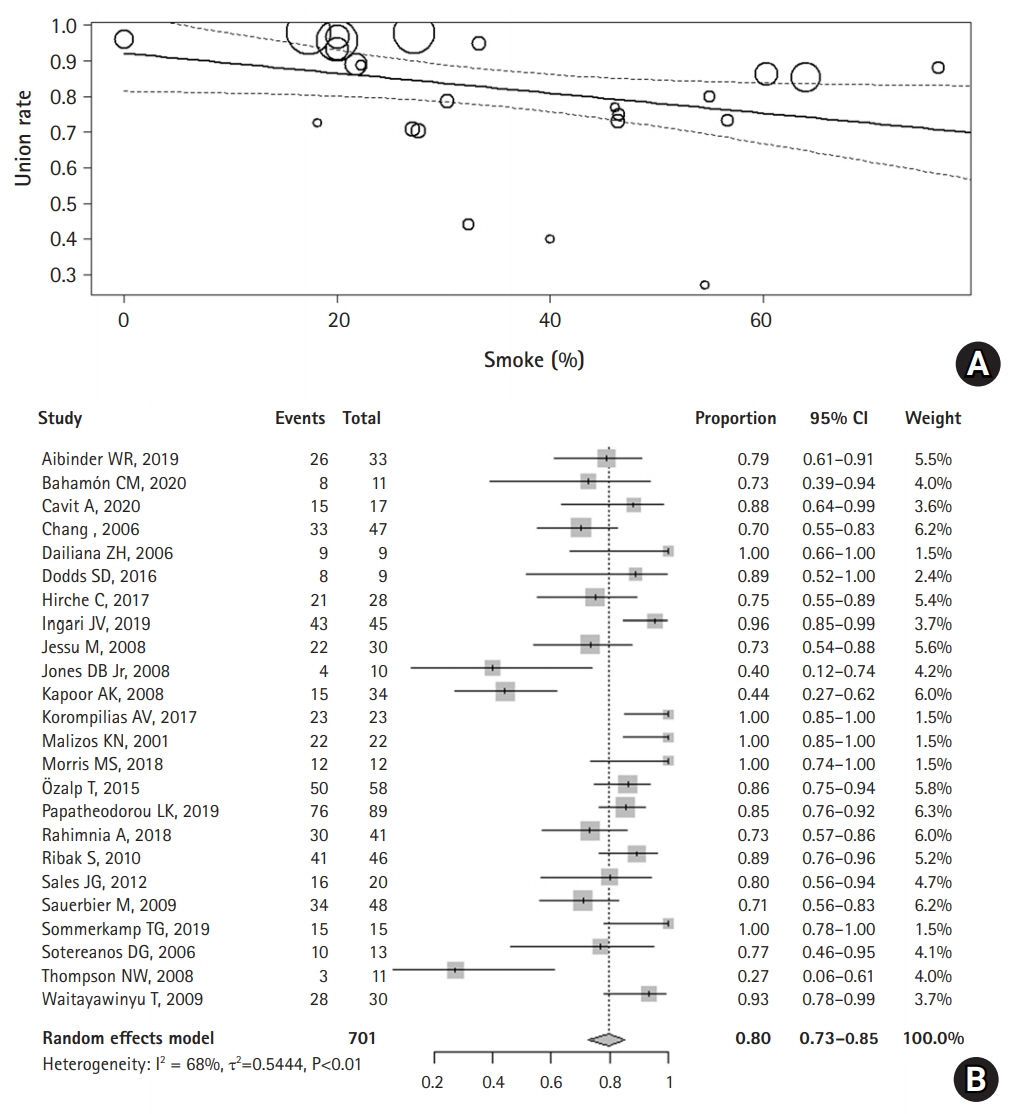
Fig. 5. (A) The correlation of smoking rate and the union rate showed a negative correlation (correlation coefficient [r]=–0.0028; 95% confidence interval, -0.0055 to -0.0001) in the subgroup analysis of pedicled vascularized bone graft. (B) The average union rate was analyzed as 79.6% (95% CI, 0.73-0.85) in the pedicled vascularized bone graft group.
Reference
-
1. Sgromolo NM, Rhee PC. The role of vascularized bone grafting in scaphoid nonunion. Hand Clin. 2019; 35:315–22.
Article2. Little CP, Burston BJ, Hopkinson-Woolley J, Burge P. Failure of surgery for scaphoid non-union is associated with smoking. J Hand Surg Br. 2006; 31:252–5.
Article3. Hwang K, Son JS, Ryu WK. Smoking and flap survival. Plast Surg (Oakv). 2018; 26:280–5.
Article4. Richardson WS, Wilson MC, Nishikawa J, Hayward RS. The well-built clinical question: a key to evidence-based decisions. ACP J Club. 1995; 123:A12–3.5. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012; 22:276–82.
Article6. Higgins JP, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions. 2nd ed. Hoboken, NJ: John Wiley & Sons;2019.7. Kim SY, Park JE, Lee YJ, et al. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J Clin Epidemiol. 2013; 66:408–14.
Article8. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997; 315:629–34.
Article9. Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000; 56:455–63.
Article10. Aibinder WR, Wagner ER, Bishop AT, Shin AY. Bone grafting for scaphoid nonunions: is free vascularized bone grafting superior for scaphoid nonunion? Hand (N Y). 2019; 14:217–22.
Article11. Arora R, Lutz M, Zimmermann R, Krappinger D, Niederwanger C, Gabl M. Free vascularised iliac bone graft for recalcitrant avascular nonunion of the scaphoid. J Bone Joint Surg Br. 2010; 92:224–9.
Article12. Bahamón CM, Valencia JA, Náquira LF, Londoño JA, Cuesta DP. Scaphoid pseudoarthrosis: experience with vascularized bone graft of the first metacarpal. Case series. Rev Colomb Ortop Traumatol. 2020; 34:60–4.13. Bürger HK, Windhofer C, Gaggl AJ, Higgins JP. Vascularized medial femoral trochlea osteocartilaginous flap reconstruction of proximal pole scaphoid nonunions. J Hand Surg Am. 2013; 38:690–700.
Article14. Bürger KH, Gaggl AJ, Kukutschki W, Mueller E. Free microvascular transfer of segmental corticocancellous femur for treatment of avascular scaphoid necrosis. Handchir Mikrochir Plast Chir. 2009; 41:44–51.15. Cavit A, Civan O, Capkin S, Kaleli T, Ozcanli H, Ozdemir H. Treatment of scaphoid nonunion with 1,2 intercompartmental supraretinacular artery vascularized graft and compression screw fixation. Injury. 2021; 52:2307–13.
Article16. Chang MA, Bishop AT, Moran SL, Shin AY. The outcomes and complications of 1,2-intercompartmental supraretinacular artery pedicled vascularized bone grafting of scaphoid nonunions. J Hand Surg Am. 2006; 31:387–96.
Article17. Chaudhry T, Uppal L, Power D, Craigen M, Tan S. Scaphoid nonunion with poor prognostic factors: the role of the free medial femoral condyle vascularized bone graft. Hand (N Y). 2017; 12:135–9.18. Dailiana ZH, Malizos KN, Zachos V, Varitimidis SE, Hantes M, Karantanas A. Vascularized bone grafts from the palmar radius for the treatment of waist nonunions of the scaphoid. J Hand Surg Am. 2006; 31:397–404.
Article19. Dodds SD, Halim A. Scaphoid plate fixation and volar carpal artery vascularized bone graft for recalcitrant scaphoid nonunions. J Hand Surg Am. 2016; 41:e191–8.
Article20. Elgammal A, Lukas B. Vascularized medial femoral condyle graft for management of scaphoid non-union. J Hand Surg Eur Vol. 2015; 40:848–54.
Article21. Higgins JP, Burger HK. Proximal scaphoid arthroplasty using the medial femoral trochlea flap. J Wrist Surg. 2013; 2:228–33.22. Hirche C, Xiong L, Heffinger C, et al. Vascularized versus non-vascularized bone grafts in the treatment of scaphoid non-union. J Orthop Surg (Hong Kong). 2017; 25:2309499016684291.
Article23. Ingari JV, Nayar SK, Taylor KF. Volar vascularized strut graft for avascular scaphoid nonunion using the 1,2 intercompartmental supraretinacular artery. Tech Hand Up Extrem Surg. 2019; 23:14–21.
Article24. Jessu M, Wavreille G, Strouk G, Fontaine C, Chantelot C. Scaphoid nonunions treated by Kuhlmann’s vascularized bone graft: radiographic outcomes and complications. Chir Main. 2008; 27:87–96.25. Jones DB Jr, Bürger H, Bishop AT, Shin AY. Treatment of scaphoid waist nonunions with an avascular proximal pole and carpal collapse. A comparison of two vascularized bone grafts. J Bone Joint Surg Am. 2008; 90:2616–25.26. Kapoor AK, Thompson NW, Rafiq I, Hayton MJ, Stillwell J, Trail IA. Vascularised bone grafting in the management of scaphoid non-union: a review of 34 cases. J Hand Surg Eur Vol. 2008; 33:628–31.27. Kollitz KM, Pulos N, Bishop AT, Shin AY. Primary medial femoral condyle vascularized bone graft for scaphoid nonunions with carpal collapse and proximal pole avascular necrosis. J Hand Surg Eur Vol. 2019; 44:600–6.
Article28. Korompilias AV, Lykissas MG, Kostas-Agnantis IP, Gkiatas I, Beris AE. An alternative graft fixation technique for scaphoid nonunions treated with vascular bone grafting. J Hand Surg Am. 2014; 39:1308–12.29. Malizos KN, Dailiana ZH, Kirou M, Vragalas V, Xenakis TA, Soucacos PN. Longstanding nonunions of scaphoid fractures with bone loss: successful reconstruction with vascularized bone grafts. J Hand Surg Br. 2001; 26:330–4.
Article30. Morris MS, Zhu AF, Ozer K, Lawton JN. Proximal pole scaphoid nonunion reconstruction with 1,2 intercompartmental supraretinacular artery vascularized graft and compression screw fixation. J Hand Surg Am. 2018; 43:770. e1-770.e8.31. Özalp T, Öz Ç, Kale G, Erkan S. Scaphoid nonunion treated with vascularised bone graft from dorsal radius. Injury. 2015; 46 Suppl 2:S47–52.
Article32. Papatheodorou LK, Sotereanos DG. Treatment for proximal pole scaphoid nonunion with capsular-based vascularized distal radius graft. Eur J Orthop Surg Traumatol. 2019; 29:337–42.
Article33. Rahimnia A, Rahimnia AH, Mobasher-Jannat A. Clinical and functional outcomes of vascularized bone graft in the treatment of scaphoid non-union. PLoS One. 2018; 13:e0197768.
Article34. Ribak S, Medina CE, Mattar R Jr, Ulson HJ, Ulson HJ, Etchebehere M. Treatment of scaphoid nonunion with vascularised and nonvascularised dorsal bone grafting from the distal radius. Int Orthop. 2010; 34:683–8.
Article35. Sales JG, Irajian M, Elmi A, Manand JS, Moradi A. Using a vascularized bone graft from the distal metaphysis of radius in treating scaphoid nonunion: first report from a developing country. Pak J Biol Sci. 2012; 15:524–9.36. Sauerbier M, Bishop AT, Ofer N. Pedicled vascularized bone grafts from the dorsum of the distal radius for treatment of scaphoid nonunions. Oper Orthop Traumatol. 2009; 21:373–85.37. Sommerkamp TG, Hastings H 2nd, Greenberg JA. Palmar radiocarpal artery vascularized bone graft for the unstable humpbacked scaphoid nonunion with an avascular proximal pole. J Hand Surg Am. 2020; 45:298–309.
Article38. Sotereanos DG, Darlis NA, Dailiana ZH, Sarris IK, Malizos KN. A capsular-based vascularized distal radius graft for proximal pole scaphoid pseudarthrosis. J Hand Surg Am. 2006; 31:580–7.
Article39. Thompson NW, Kapoor A, Thomas J, Hayton MJ. The use of a vascularised periosteal patch onlay graft in the management of nonunion of the proximal scaphoid. J Bone Joint Surg Br. 2008; 90:1597–601.
Article40. Waitayawinyu T, McCallister WV, Katolik LI, Schlenker JD, Trumble TE. Outcome after vascularized bone grafting of scaphoid nonunions with avascular necrosis. J Hand Surg Am. 2009; 34:387–94.
Article41. Scott J, Checketts JX, Cooper CM, Boose M, Wayant C, Vassar M. An evaluation of publication bias in high-impact orthopaedic literature. JB JS Open Access. 2019; 4:e0055.
Article42. Michael Pittilo R. Cigarette smoking, endothelial injury and cardiovascular disease. Int J Exp Pathol. 2000; 81:219–30.
Article43. Rancy SK, Schmidle G, Wolfe SW. Does anyone need a vascularized graft? Hand Clin. 2019; 35:323–44.
Article44. Al-Jabri T, Mannan A, Giannoudis P. The use of the free vascularised bone graft for nonunion of the scaphoid: a systematic review. J Orthop Surg Res. 2014; 9:21.
Article45. Jubbal KT, Zavlin D, Suliman A. The effect of age on microsurgical free flap outcomes: an analysis of 5,951 cases. Microsurgery. 2017; 37:858–64.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Scaphoid Fractures and Nonunions
- A Comparative Study of Three Different Bone Grafting Methods for Treatment of Scaphoid Nonunion
- Treatment of Scaphoid Nonunionusing a Pedicled Vascularized Bone Graft
- Treatment of Nonunion of Proximal Scaphoid Fractures Using Vascularized Bone Graft
- Arthroscopic Bone Grafting and Kirschner-Wires Fixation for Scaphoid Nonunion
