Living donor liver transplantation in a pediatric patient with congenital absence of the portal vein
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2519299
- DOI: http://doi.org/10.14701/ahbps.2021.25.3.401
Abstract
- Congenital absence of the portal vein (CAPV) is a rare venous malformation in which mesenteric venous blood drains directly into the systemic circulation. We report a case of pediatric living donor liver transplantation (LDLT) for CAPV combined with focal nodular hyperplasia (FNH) and hepatocellular adenoma. A 9-year-old girl who had been diagnosed with multiple FNH had CAPV. Her blood ammonia level was raised to 137 µg/dL. However, she did not complain of any symptoms. To treat CAPV and FNH, we decided to perform LDLT. The graft was a left liver graft from 39-year-old mother of the patient. Recipient hepatectomy was performed according to standard procedures of pediatric LDLT. Portal vein reconstruction was performed using interposition of an iliac vein homograft conduit to the superior mesenteric vein-splenic vein conf luence. The CAPV-associated congenital splenorenal shunt was securely ligated. The pathology report of the explant liver showed a 2 cm-sized hepatocellular adenoma and multiple FNH lesions measuring up to 7.1 cm. The patient recovered uneventfully from the LDLT operation. The reconstructed portal vein was maintained well without any hemodynamic abnormalities. In conclusion, as CAPV patients can have various vascular anomalies, combined vascular anomalies should be thoroughly assessed before and during liver transplantation operation. The most effective reconstruction techniques should be used to achieve satisfactory results following liver transplantation.
Keyword
Figure
-
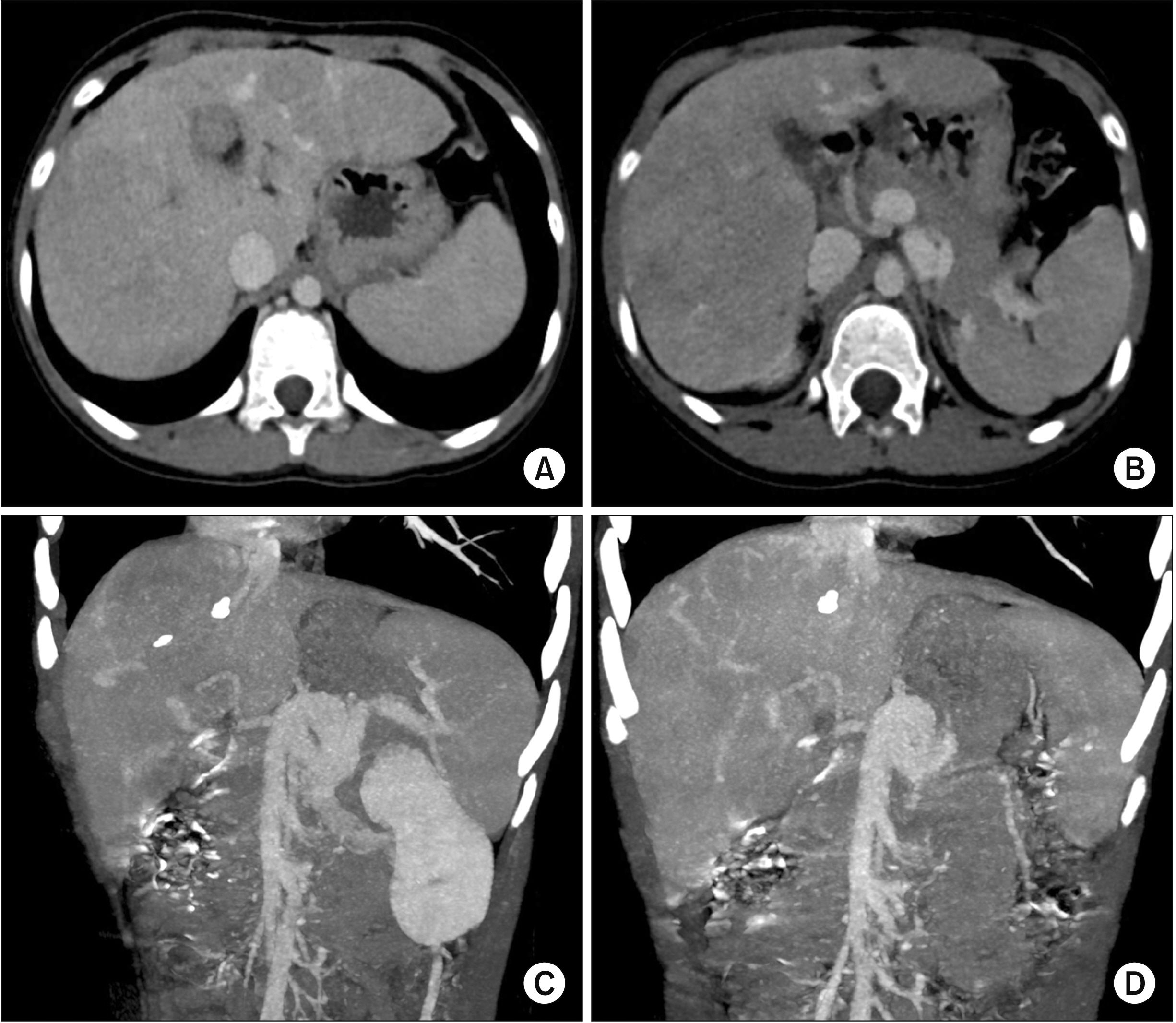
Fig. 1 Pretransplant computed tomography findings of the recipient. (A, B) Multiple liver tumors can be seen. (C, D) The portal vein is absent, which is compatible with the congenital absence of the portal vein.

Fig. 2 Preoperative computed tomography findings of the living donor. (A) The volume of the left liver is measured to be 508 mL by volumetry. (B) The diameter of the left portal vein appears unusually small (arrow).

Fig. 3 Intraoperative photographs for recipient hepatectomy and graft bench work. (A) The hepatic artery branches are meticulously dissected after transection of the common bile duct. (B) The retropancreatic space is dissected and the left renal vein (yellow vessel loop) and the insertion site of the splenorenal shunt (black silk sling) are isolated. (C) The confluence portion of the mesentero-splenic vein is meticulously dissected. (D) The graft hepatic veins are separated into three openings, which are unified to make a wide single orifice.

Fig. 4 Intraoperative photographs of the hepatic vein and portal vein venoplasty. (A) The hepatic vein orifices at the recipient inferior vena cava are unified with venoplasty using a cryopreserved saphenous vein patch. (B) The vein branches at the mesentero-splenic confluence portion are securely clamped. (C) A 1.5 cm-long longitudinal incision is made at the confluence portion. (D–F) A 4 cm-long fresh-stored iliac vein conduit is anastomosed to the confluence portion in an end-to-side fashion.

Fig. 5 Intraoperative photographs of graft implantation. (A, B) The graft hepatic vein orifice is anastomosed with the size-matched recipient hepatic vein orifice. (C, D) The portal iliac vein conduit is anastomosed with the graft portal vein. (E) The congenital splenorenal shunt is securely ligated. (F) Portal blood flow is increased after ligation of the splenorenal shunt.

Fig. 6 Intraoperative direct portography findings. (A) Portal blood flow is well maintained. (B) A collateral vein through the inferior mesenteric vein and the lumbar vein is identified and ligated.
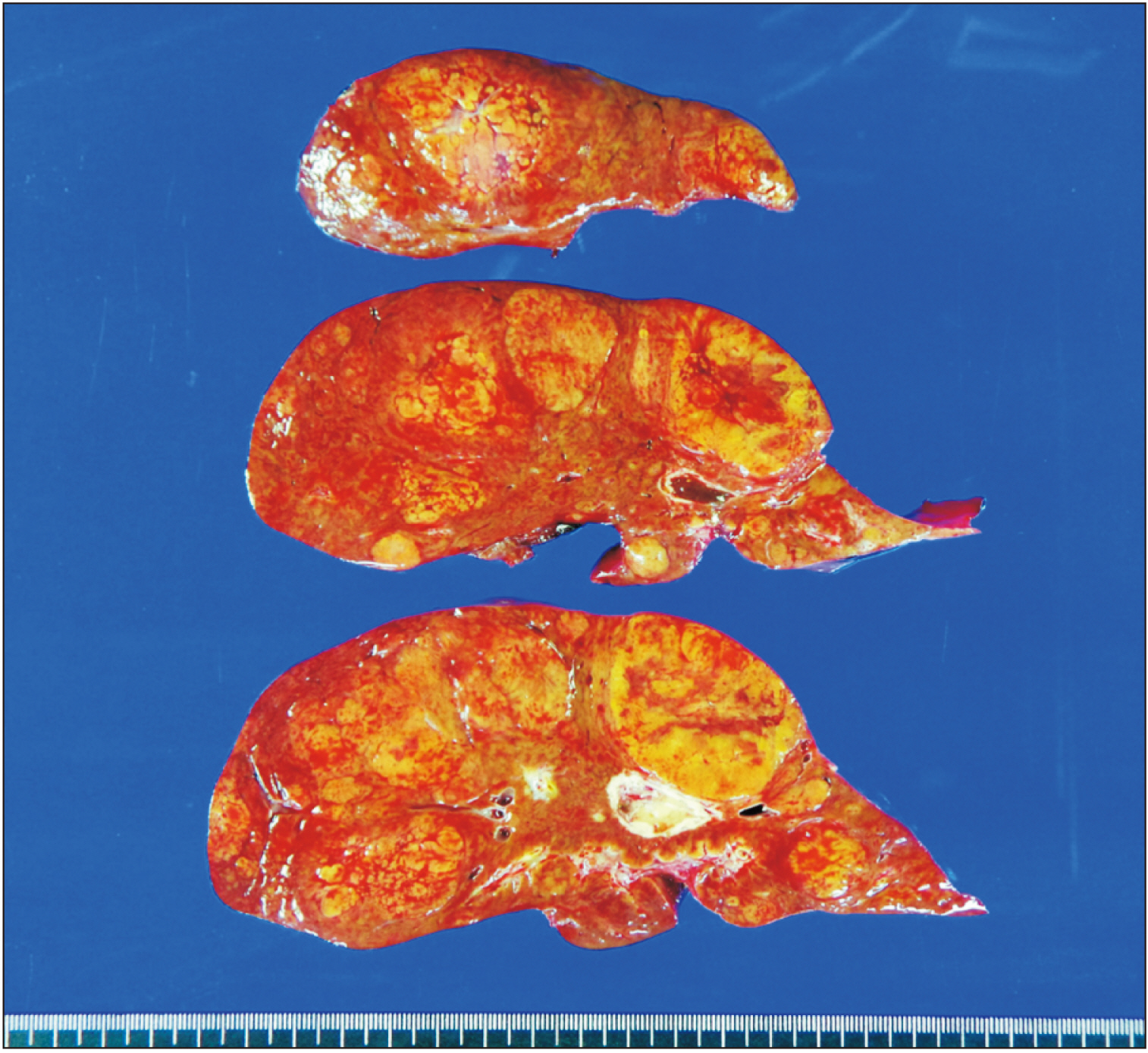
Fig. 7 Gross photographs of the explant liver. There are three types of liver nodules. A 2 cm-sized hepatocellular adenoma of beta-catenin mutated subtype is located at segment IV. Multiple focal nodular hyperplasia nodules measuring up to 7.1 cm in size are scattered over both lobes. Multiple regenerative nodules measuring up to 2.7 cm in size are also present in both lobes.

Fig. 8 Posttransplant computed tomography scan taken at four days after the transplantation. (A, B) The graft portal vein reconstruction appears smooth and streamlined. (C, D) The iliac vein conduit from the mesentero-splenic vein junction is well visualized as a newly made main portal vein.

Fig. 9 Posttransplant Doppler ultrasonography at 21 days after transplantation. (A) The contour of portal vein anastomosis appears smooth and streamlined with slight stenosis at the anastomosis site. Arrow indicates the interposed iliac vein conduit. (B) The portal vein blood flow is well maintained.
Cited by 3 articles
-
Living donor liver transplantation with graft dextro-rotation and vein interposition in a pediatric patient with congenital absence of the portal vein
Jung-Man Namgoong, Shin Hwang, Gil-Chun Park, Sang-Hoon Kim, Kyung Mo Kim, Seak Hee Oh
Ann Liver Transplant. 2023;3(1):35-43. doi: 10.52604/alt.23.0004.Living donor liver transplantation with direct collateral portal vein anastomosis in a pediatric patient with congenital absence of the portal vein
Jung-Man Namgoong, Shin Hwang, Gil-Chun Park, Do Young Lee, Kyung Mo Kim, Seak Hee Oh
Ann Liver Transplant. 2023;3(2):128-135. doi: 10.52604/alt.23.0013.Living donor liver transplantation with pericholedochal collateral vein anastomosis in a pediatric patient with congenital absence of the portal vein
Jung-Man Namgoong, Shin Hwang, Gil-Chun Park, Sujin Kang, Kyung Mo Kim, Seak Hee Oh
Ann Liver Transplant. 2023;3(2):118-127. doi: 10.52604/alt.23.0016.
Reference
-
1. Sanada Y, Mizuta K, Kawano Y, Egami S, Hayashida M, Wakiya T, et al. 2009; Living donor liver transplantation for congenital absence of the portal vein. Transplant Proc. 41:4214–4219. DOI: 10.1016/j.transproceed.2009.08.080. PMID: 32029317.
Article2. Shinkai M, Ohhama Y, Nishi T, Yamamoto H, Fujita S, Take H, et al. 2001; Congenital absence of the portal vein and role of liver transplantation in children. J Pediatr Surg. 36:1026–1031. DOI: 10.1053/jpsu.2001.24731. PMID: 11431769.
Article3. Wojcicki M, Haagsma EB, Gouw AS, Slooff MJ, Porte RJ. 2004; Orthotopic liver transplantation for portosystemic encephalopathy in an adult with congenital absence of the portal vein. Liver Transpl. 10:1203–1207. DOI: 10.1002/lt.20170. PMID: 15350015.
Article4. Ikeda S, Sera Y, Ohshiro H, Uchino S, Uchino T, Endo F. 1999; Surgical indications for patients with hyperammonemia. J Pediatr Surg. 34:1012–1015. DOI: 10.1016/S0022-3468(99)90780-7. PMID: 10392925.
Article5. Sumida W, Kaneko K, Ogura Y, Tainaka T, Ono Y, Seo T, et al. 2006; Living donor liver transplantation for congenital absence of the portal vein in a child with cardiac failure. J Pediatr Surg. 41:e9–e12. DOI: 10.1016/j.jpedsurg.2006.07.014. PMID: 17101345.
Article6. Watanabe A. 2000; Portal-systemic encephalopathy in non-cirrhotic patients: classification of clinical types, diagnosis and treatment. J Gastroenterol Hepatol. 15:969–979. DOI: 10.1046/j.1440-1746.2000.02283.x. PMID: 11059925.
Article7. Morgan G, Superina R. 1994; Congenital absence of the portal vein: two cases and a proposed classification system for portasystemic vascular anomalies. J Pediatr Surg. 29:1239–1241. DOI: 10.1016/0022-3468(94)90812-5. PMID: 7807356.
Article8. Emre S, Arnon R, Cohen E, Morotti RA, Vaysman D, Shneider BL. 2007; Resolution of hepatopulmonary syndrome after auxiliary partial orthotopic liver transplantation in Abernethy malformation. A case report. Liver Transpl. 13:1662–1668. DOI: 10.1002/lt.21349. PMID: 18044784.9. Soejima Y, Taguchi T, Ogita K, Taketomi A, Yoshizumi T, Uchiyama H, et al. 2006; Auxiliary partial orthotopic living donor liver transplantation for a child with congenital absence of the portal vein. Liver Transpl. 12:845–849. DOI: 10.1002/lt.20692. PMID: 16628685.
Article10. Namgoong JM, Hwang S, Kim DY, Ha TY, Song GW, Jung DH, et al. 2021; Pediatric liver transplantation using a hepatitis B surface antigen-positive donor liver graft for congenital absence of the portal vein. Korean J Transplant. 35:59–65. DOI: 10.4285/kjt.20.0038.
Article11. Woodle ES, Thistlethwaite JR, Emond JC, Whitington PF, Vogelbach P, Yousefzadeh DK, et al. 1990; Successful hepatic transplantation in congenital absence of recipient portal vein. Surgery. 107:475–479. PMID: 2321142.12. Ohnishi Y, Ueda M, Doi H, Kasahara M, Haga H, Kamei H, et al. 2005; Successful liver transplantation for congenital absence of the portal vein complicated by intrapulmonary shunt and brain abscess. J Pediatr Surg. 40:e1–e3. DOI: 10.1016/j.jpedsurg.2005.02.011. PMID: 15937799.
Article13. Charre L, Roggen F, Lemaire J, Mathijs J, Goffette P, Danse E, et al. 2004; Hematochezia and congenital extrahepatic portocaval shunt with absent portal vein: successful treatment by liver transplantation. Transplantation. 78:1404–1406. DOI: 10.1097/01.TP.0000137931.51504.F7. PMID: 15548983.
Article14. Benedict M, Rodriguez-Davalos M, Emre S, Walther Z, Morotti R. 2017; Congenital extrahepatic portosystemic shunt (Abernethy malformation type Ib) with associated hepatocellular carcinoma: case report and literature review. Pediatr Dev Pathol. 20:354–362. DOI: 10.1177/1093526616686458. PMID: 28727971.
Article15. Virdis M, Monteleone M, Sposito C, Cascella T, Pellegrinelli A, Mazzaferro V. 2018; Hepatocellular carcinoma in Abernethy malformation: a rare occurrence of congenital complete portosystemic shunt. J Vasc Interv Radiol. 29:1775–1778. DOI: 10.1016/j.jvir.2018.07.014. PMID: 30502882.16. Christou N, Dib N, Chuffart E, Taibi A, Durand-Fontanier S, Valleix D, et al. 2018; Stepwise management of hepatocellular carcinoma associated with Abernethy syndrome. Clin Case Rep. 6:930–934. DOI: 10.1002/ccr3.1384. PMID: 29744090. PMCID: PMC5930207.
Article17. Chiang J, Chiu HK, Moriarty JM, McWilliams JP. 2020; Hyperandrogenism and malignant degeneration of hepatic adenomas in the setting of Abernethy malformation. Radiol Case Rep. 15:2701–2705. DOI: 10.1016/j.radcr.2020.10.026. PMID: 33117471. PMCID: PMC7581830.
Article18. Rajeswaran S, Johnston A, Green J, Riaz A, Thornburg B, Mouli S, et al. 2020; Abernethy malformations: evaluation and management of congenital portosystemic shunts. J Vasc Interv Radiol. 31:788–794. DOI: 10.1016/j.jvir.2019.08.007. PMID: 32107126.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Living donor liver transplantation in a pediatric patient having intrahepatic portocaval shunt with congenital absence of the intrahepatic portal vein
- Congenital Absence of the Horizontal Segment of the Left Portal Vein
- Living donor liver transplantation with direct collateral portal vein anastomosis in a pediatric patient with congenital absence of the portal vein
- Living donor liver transplantation with graft dextro-rotation and vein interposition in a pediatric patient with congenital absence of the portal vein
- Portal vein fenestration: a case report of an unusual portal vein developmental anomaly
