Endoscopically-Assisted Scar-Free Midline Neck Mass Excision
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Dankook University College of Medicine, Cheonan, Korea
- KMID: 2519179
- DOI: http://doi.org/10.21053/ceo.2020.02446
Abstract
- Traditional open surgery is indicated for the treatment of selected tumor subsites in the head and neck. However, it can cause major cosmetic problems and functional pathologies. The endoscopically-assisted transoral approach is increasingly preferred in some surgical fields due to its superior cosmetic and functional outcomes. Nonetheless, endoscopically-assisted transoral approach is not yet standard in the head and neck due to their anatomical complexity. The transoral surgical approach has been used for head and neck masses since the 1960s, and its application continues to evolve with changing disease conditions and recent innovations in surgical instruments. The potential for wide application of transoral surgery continues to be investigated, with a focus on minimizing occurrence of the complications. This review presents details of the surgical procedure and postoperative clinical outcomes, as well as endoscopically-assisted scar-free techniques for the resection of midline neck masses.
Keyword
Figure
-
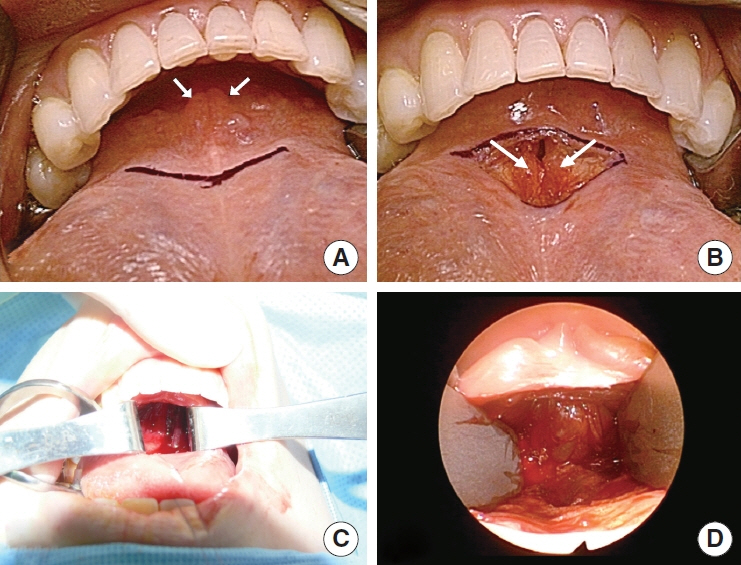
Fig. 1. (A-D) Transoral approach. After frenotomy, the genioglossus muscle (white arrows) is located and retracted bilaterally to facilitate the approach to the anterior neck area.
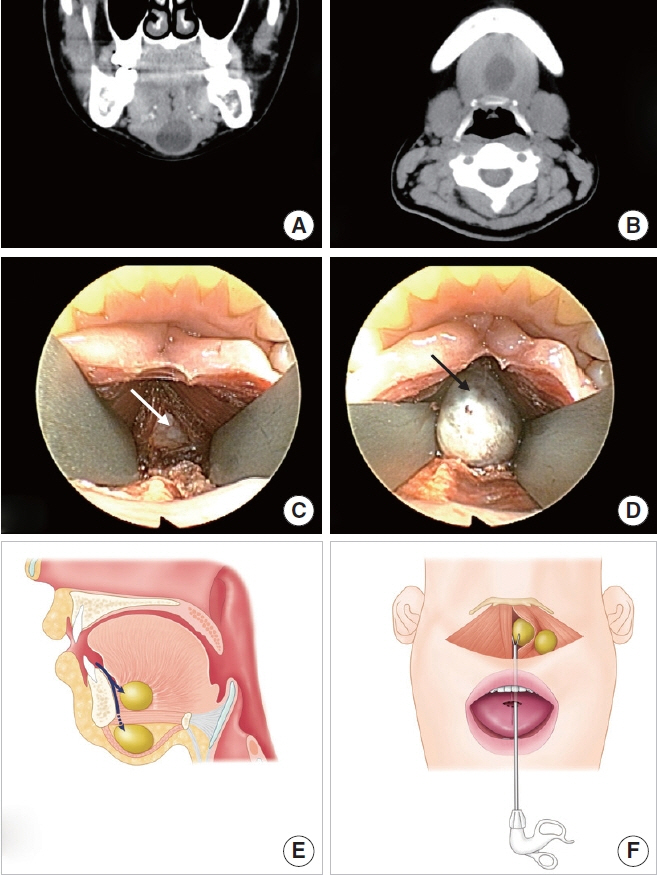
Fig. 2. Transoral approach via a midline incision in the floor of the oral cavity. (A, B) Computed tomography reveals a neck mass beneath the mylohyoid muscle. (C) An incision is made in the midline of the floor of the oral cavity through a frenulum. After dissecting the soft tissue of the floor of the mouth, the genioglossus muscle is separated at the midline and retracted bilaterally (white arrow). The mylohyoid muscle is then exposed. Endoscopic guidance can identify mass-like lesions after mylohyoid muscle resection. (D) After dissecting the soft tissue around the mass (black arrow), it is removed. (E) Transoral approach for a neck mass at the floor of mouth and above the mylohyoid muscle. Anatomical view. Surgical approach to locate dermoid cysts below or above the mylohyoid muscle (arrows). (F) Surgical view. Removal of a dermoid cyst using an endoscopic dissector through the mucosal horizontal incision at the tongue frenulum.
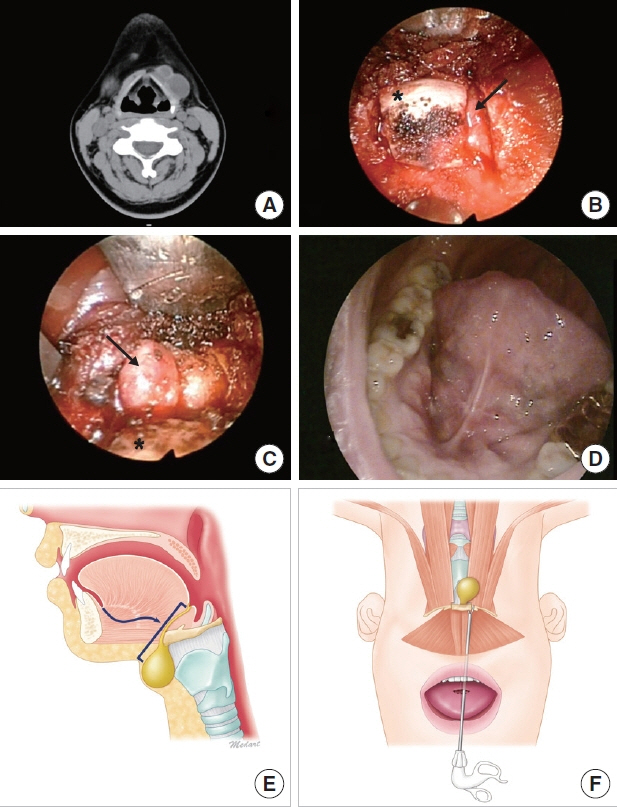
Fig. 3. Transoral thyroglossal ductal cyst excision. (A) Computed tomography reveals two thyroglossal ductal cysts as midline neck masses. (B) A vertical incision is made through the frenulum at the midline of the floor of the oral cavity. After dissecting the soft tissue, the hyoid bone (asterisk) and thyroglossal duct cyst (TGDC; arrow) are identified. (C) After cutting the hyoid bone with a 1-mm osteopunch rongeur, the TGDC (arrow) attached to the hyoid bone (asterisk) is removed via careful incision of the cyst, while pulling the hyoid bone upward. (D) Oral cavity scar at 1 month postoperatively. (E) Transoral approach for neck mass below the geniohyoid. Anatomical view. Surgical approach to locate the TGDC (arrow) and overall range of surgery. (F) Surgical view. Removal of the TGDC altogether with the dissected hyoid bone.

Fig. 4. Transoral thyroidectomy. (A) Safety zone and incision line (red dots). (B) The subplatysmal flap is retracted superiorly after creating a surgical path. (C) Operative view of transoral thyroidectomy. (D) Removal of the thyroid endoscopically. (E) Transoral approach for thyroid and perithyroid area. Anatomical view. Surgical approach to locate the thyroid gland. Elevation of a lower lip flap with a Sofield retractor. (F) Surgical view. Endoscopic dissector through the mucosal horizontal incision at the lower lip.

Fig. 5. Transoral thyroidectomy. (A) The subplatysmal flap is lifted to expose the strap muscle and thyroid (asterisk). (B) Dissection of the recurrent laryngeal nerve (white arrow). (C) Removal of the thyroid mass (asterisk). (D) One week after transoral thyroidectomy.
Reference
-
1. Park JO. Facelift approach for resecting benign upper neck masses. World J Surg. 2017; Jun. 41(6):1488–93.
Article2. Rumsey N, Clarke A, White P. Exploring the psychosocial concerns of outpatients with disfiguring conditions. J Wound Care. 2003; Jul. 12(7):247–52.
Article3. Gagner M, Inabnet WB 3rd. Endoscopic thyroidectomy for solitary thyroid nodules. Thyroid. 2001; Feb. 11(2):161–3.
Article4. Lee HS, Lee D, Koo YC, Shin HA, Koh YW, Choi EC. Endoscopic resection of upper neck masses via retroauricular approach is feasible with excellent cosmetic outcomes. J Oral Maxillofac Surg. 2013; Mar. 71(3):520–7.
Article5. Kim JP, Lee DK, Moon JH, Park JJ, Woo SH. Transoral dermoid cyst excision: a multicenter prospective observational study. Otolaryngol Head Neck Surg. 2018; Dec. 159(6):981–6.
Article6. Kim JP, Park JJ, Jeon SY, Ahn SK, Hur DG, Kim DW, et al. Endoscopeassisted intraoral resection of external dermoid cyst. Head Neck. 2012; Jun. 34(6):907–10.
Article7. Kim JP, Park JJ, Lee EJ, Woo SH. Intraoral removal of a thyroglossal duct cyst using a frenotomy incision. Thyroid. 2011; Dec. 21(12):1381–4.
Article8. Kim JP, Park JJ, Park HW, Woo SH. Endoscopy-assisted resection of a submandibular gland mass via a thyroidectomy incision. Ear Nose Throat J. 2015; Sep. 94(9):E30–3.9. Kim JP, Park JJ, Woo SH. No-scar transoral thyroglossal duct cyst excision in children. Thyroid. 2018; Jun. 28(6):755–61.
Article10. Woo SH. Endoscopic-assisted total thyroidectomy via lateral keloid scar incision. Clin Exp Otorhinolaryngol. 2014; Dec. 7(4):338–41.
Article11. Woo SH. Endoscope-assisted transoral thyroidectomy using a frenotomy incision. J Laparoendosc Adv Surg Tech A. 2014; May. 24(5):345–9.
Article12. Woo SH. Endoscope-assisted transoral accessory parotid mass excision. Head Neck. 2016; Jan. 38(1):E7–12.
Article13. Woo SH, Jeong HS, Kim JP, Park JJ, Baek CH. Endoscope-assisted intraoral removal of ectopic thyroid tissue using a frenotomy incision. Thyroid. 2013; May. 23(5):605–8.
Article14. Woo SH, Jeong HS, Kim JP, Park JJ, Baek CH. Endoscope-assisted frenotomy approach to median upper neck masses: clinical outcomes and safety (from a phase II clinical trial). Head Neck. 2014; Jul. 36(7):985–91.
Article15. Woo SH, Kim JP, Baek CH. Endoscope-assisted extracapsular dissection of benign parotid tumors using hairline incision. Head Neck. 2016; Mar. 38(3):375–9.
Article16. Clark MP, Qayed ES, Kooby DA, Maithel SK, Willingham FF. Natural orifice translumenal endoscopic surgery in humans: a review. Minim Invasive Surg. 2012; 2012:189296.
Article17. Anuwong A. Transoral endoscopic thyroidectomy vestibular approach: a series of the first 60 human cases. World J Surg. 2016; Mar. 40(3):491–7.
Article18. Anuwong A, Ketwong K, Jitpratoom P, Sasanakietkul T, Duh QY. Safety and outcomes of the transoral endoscopic thyroidectomy vestibular approach. JAMA Surg. 2018; Jan. 153(1):21–7.
Article19. Kim HY, Chai YJ, Dionigi G, Anuwong A, Richmon JD. Transoral robotic thyroidectomy: lessons learned from an initial consecutive series of 24 patients. Surg Endosc. 2018; Feb. 32(2):688–94.
Article20. Turetschek K, Hospodka H, Steiner E. Case report: epidermoid cyst of the floor of the mouth: diagnostic imaging by sonography, computed tomography and magnetic resonance imaging. Br J Radiol. 1995; Feb. 68(806):205–7.21. Zachariades N, Skoura-Kafoussia C. A life-threatening epidermoid cyst of the floor of the mouth: report of a case. J Oral Maxillofac Surg. 1990; Apr. 48(4):400–3.
Article22. Calderon S, Kaplan I. Concomitant sublingual and submental epidermoid cysts: a case report. J Oral Maxillofac Surg. 1993; Jul. 51(7):790–2.
Article23. Longo F, Maremonti P, Mangone GM, De Maria G, Califano L. Midline (dermoid) cysts of the floor of the mouth: report of 16 cases and review of surgical techniques. Plast Reconstr Surg. 2003; Nov. 112(6):1560–5.
Article24. Ariyoshi Y, Shimahara M. Magnetic resonance imaging of a submental dermoid cyst: report of a case. J Oral Maxillofac Surg. 2003; Apr. 61(4):507–10.
Article25. Bodner L, Woldenberg Y, Sion-Vardy N. Dermoid cyst of the maxilla. Int J Oral Maxillofac Surg. 2005; Jun. 34(4):453–5.
Article26. Woo SH, Park JJ, Kwon M, Kim JP. “Hidden scar” submandibular gland excision using an endoscope-assisted hairline approach. Oral Oncol. 2017; Feb. 65:83–8.
Article27. Kim HS, Chung SM, Pae SY, Park HS. Endoscope assisted submandibular sialadenectomy: the face-lift approach. Eur Arch Otorhinolaryngol. 2011; Apr. 268(4):619–22.
Article28. Akao I, Nobukiyo S, Kobayashi T, Kikuchi H, Koizuka I. A case of large dermoid cyst in the floor of the mouth. Auris Nasus Larynx. 2003; Feb. 30 Suppl:S137–9.
Article29. Leveque H, Saraceno CA, Tang CK, Blanchard CL. Dermoid cysts of the floor of the mouth and lateral neck. Laryngoscope. 1979; Feb. 89(2 Pt 1):296–305.
Article30. Radkowski D, Arnold J, Healy GB, McGill T, Treves ST, Paltiel H, et al. Thyroglossal duct remnants: preoperative evaluation and management. Arch Otolaryngol Head Neck Surg. 1991; Dec. 117(12):1378–81.
Article31. Allard RH. The thyroglossal cyst. Head Neck Surg. 1982; Nov-Dec. 5(2):134–46.
Article32. Sammarco GJ, Mc Kenna J. Thyroglossal duct cysts in the elderly. Geriatrics. 1970; Aug. 25(8):98–101.33. Hussain K, Henney S, Tzifa K. A ten-year experience of thyroglossal duct cyst surgery in children. Eur Arch Otorhinolaryngol. 2013; Nov. 270(11):2959–61.
Article34. Marianowski R, Ait Amer JL, Morisseau-Durand MP, Manach Y, Rassi S. Risk factors for thyroglossal duct remnants after Sistrunk procedure in a pediatric population. Int J Pediatr Otorhinolaryngol. 2003; Jan. 67(1):19–23.
Article35. Woo SH, Park JJ, Hong JC, Wang SG, Park GC, Eun YG, et al. Endoscope-assisted transoral removal of a thyroglossal duct cyst using a frenotomy incision: a prospective clinical trial. Laryngoscope. 2015; Dec. 125(12):2730–5.
Article36. Lin ST, Tseng FY, Hsu CJ, Yeh TH, Chen YS. Thyroglossal duct cyst: a comparison between children and adults. Am J Otolaryngol. 2008; Mar-Apr. 29(2):83–7.
Article37. Maddalozzo J, Venkatesan TK, Gupta P. Complications associated with the Sistrunk procedure. Laryngoscope. 2001; Jan. 111(1):119–23.
Article38. Mondin V, Ferlito A, Muzzi E, Silver CE, Fagan JJ, Devaney KO, et al. Thyroglossal duct cyst: personal experience and literature review. Auris Nasus Larynx. 2008; Mar. 35(1):11–25.
Article39. Perkins JA, Inglis AF, Sie KC, Manning SC. Recurrent thyroglossal duct cysts: a 23-year experience and a new method for management. Ann Otol Rhinol Laryngol. 2006; Nov. 115(11):850–6.
Article40. Shah R, Gow K, Sobol SE. Outcome of thyroglossal duct cyst excision is independent of presenting age or symptomatology. Int J Pediatr Otorhinolaryngol. 2007; Nov. 71(11):1731–5.
Article41. Brousseau VJ, Solares CA, Xu M, Krakovitz P, Koltai PJ. Thyroglossal duct cysts: presentation and management in children versus adults. Int J Pediatr Otorhinolaryngol. 2003; Dec. 67(12):1285–90.
Article42. Lee JS, Kim JP, Ryu JS, Woo SH. Effect of wound massage on neck discomfort and voice changes after thyroidectomy. Surgery. 2018; Nov. 164(5):965–71.
Article43. Huscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997; Aug. 11(8):877.
Article44. Henry JF, Sebag F. Lateral endoscopic approach for thyroid and parathyroid surgery. Ann Chir. 2006; Jan. 131(1):51–6.45. Yang HM, Shin KJ, Min J, Woo SH. Anatomical study of gasless transoral thyroidectomy and clinical application. Surg Endosc. 2020; Aug. 34(8):3414–23.
Article46. Woo SH. Endoscope-assisted intraoral removal of the thyroid isthmus mass using a frenotomy incision. J Laparoendosc Adv Surg Tech A. 2013; Sep. 23(9):787–90.
Article47. Tae K. Complications of transoral thyroidectomy: overview and update. Clin Exp Otorhinolaryngol. 2021; May. 14(2):169–78.
Article48. Hong YT, Woo SH. Robotic modified radical neck dissection through the bilateral axillary breast approach. Clin Exp Otorhinolaryngol. 2021; Feb. 14(1):13–4.
Article49. Kim SI, Min HK, Kang DW, Choi SY, Kang HJ, Lee YC, et al. Modified transoral endoscopic thyroidectomy technique using trapdoor suspension sutures. Clin Exp Otorhinolaryngol. 2021 Mar 30 [Epub]. https://doi.org/10.21053/ceo.2021.00101.
Article50. Tae K. Transoral thyroidectomy: is it a real game changer. Clin Exp Otorhinolaryngol. 2020; May. 13(2):93–4.
Article51. Tae K, Ji YB, Song CM, Ryu J. Robotic and endoscopic thyroid surgery: evolution and advances. Clin Exp Otorhinolaryngol. 2019; Feb. 12(1):1–11.
Article52. Padalhin AR. Lasers and robots: recent developments in transoral laser and transoral robotic surgery. Med Lasers. 2020; Dec. 9(2):103–9.
Article53. Lee SJ, Chung PS, Chung SY, Woo SH. Transoral laser excision of a pyriform sinus cyst. Med Lasers. 2019; Dec. 8(2):84–6.
Article54. Hong JC, Lee KD. Transoral laser surgery for supraglottic carcinoma. Med Lasers. 2013; Jun. 2(1):1–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transoral Thyroglossal Duct Cyst Excision
- Breast Reconstruction Using Bipedicled free TRAM in Patients with Subumbilical Vertical Midline Scar
- Endoscopically Assisted Transumbilical Subpectoral Augmentation Mammoplasty
- A stepwise approach to robotic assisted excision of a cesarean scar pregnancy
- Scar Revision of Wide Facial Scar by Serial Excision Using the Sure-Closure(R)
