Long Term Follow-Up after Repeated Percutaneous Transluminal Coronary Rotational Ablations for a Severe Calcified Coronary Artery Stenosis Associated with Kawasaki Disease
- Affiliations
-
- 1Department of Pediatrics, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2519154
- DOI: http://doi.org/10.4070/kcj.2021.0142
Figure
-
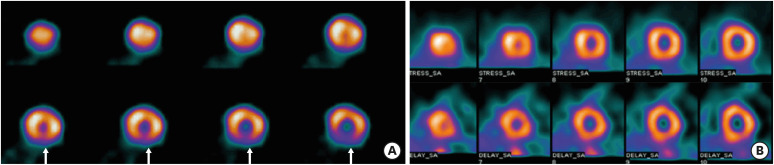
Figure 1 Dipyridamole stress thallium 201 SPECT at 8 years old showing a reversible perfusion defect (arrows) in the inferior wall of the left ventricle (A), and normal perfusion at 6 months after the PTCRA (B).PTCRA = percutaneous transluminal coronary rotational ablation; SPECT = single-photon emission computed tomography.
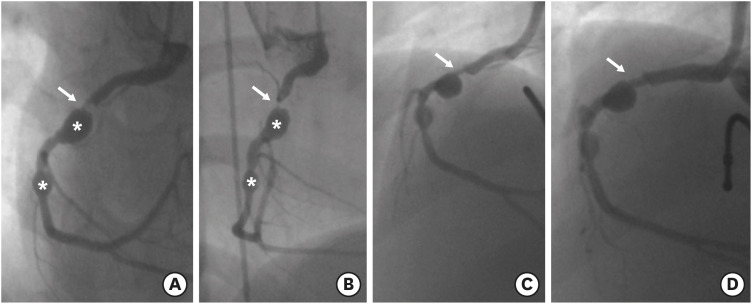
Figure 2 Coronary angiographies of RCA at 8 years of age, showing two coronary aneurysms (asterisks) and severe stenosis (>90% in diameter) at the proximal segment of the RCA (arrows) (A, B), a residual stenosis after coronary balloon angioplasty (C), and an improved coronary stenosis (arrow) after the PTCRA (D).PTCRA = percutaneous transluminal coronary rotational ablation; RCA = right coronary artery.
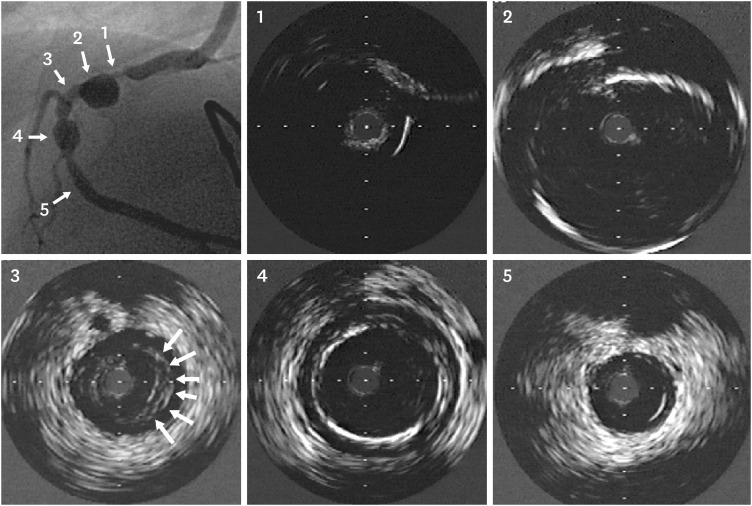
Figure 3 Intravenous ultrasound images before PTCRA at 8 years of age. Each numbered image corresponds to the sites indicated by numbers and arrows in the angiography image (far left and upper image). Severe stenosis and calcification (360°) (1), a huge aneurysm (about 7 mm in diameter), wall thickening, and calcifications (2), an intimal proliferation and thickening (arrows) (3), another aneurysm with calcification (4), and a nearly normal coronary artery (5) are demonstrated, all of which are unique characteristics of coronary artery lesions associated with Kawasaki disease.PTCRA = percutaneous transluminal coronary rotational ablation.
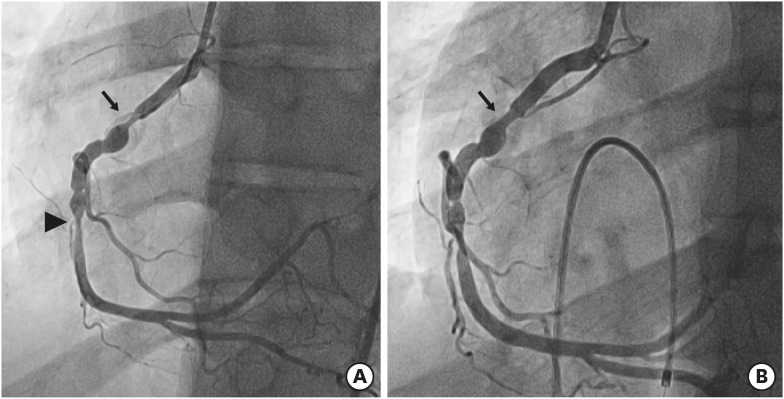
Figure 4 Coronary angiographies at 20 years of age (12 years after the first PTCRA), showing a restenosis of the target lesion (arrow) and another stenosis at the mid RCA (arrowhead) (A), and an improved target lesion stenosis after the second PTCRA (arrow) (B).PTCRA = percutaneous transluminal coronary rotational ablation; RCA = right coronary artery.
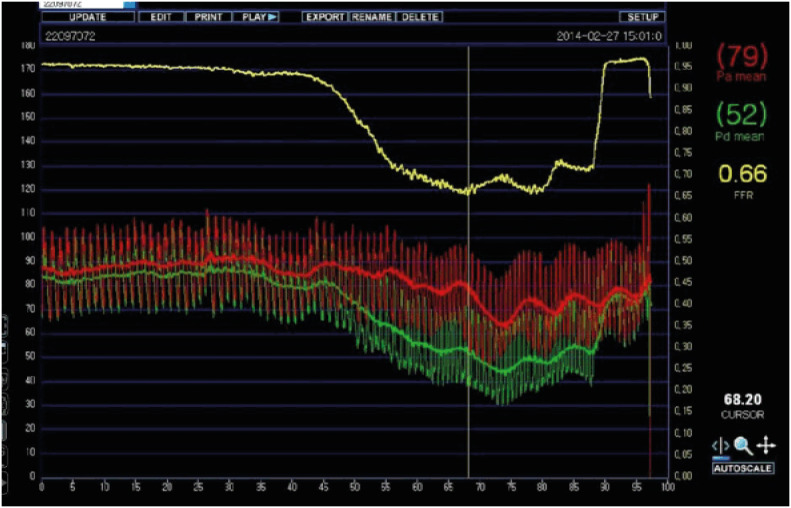
Figure 5 FFR measurement image after intracoronary adenosine administration at 20 years of age (12 years after the first PTCRA). Measured FFR was 0.66 at the time of the lowest FFR (vertical line). The yellow line, red line, and green line indicate FFR, a mean aortic pressure, and a mean coronary artery pressure distal to the target lesion stenosis in the Figure 4A (arrow), respectively.FFR = fractional flow reserve; PTCRA = percutaneous transluminal coronary rotational ablation.
Reference
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in a Young Patient with Long Term Kawasaki Disease
- Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in an Adult Kawasaki Disease with Coronary Aneurysm : A Case Report and Review
- Percutaneous transluminal coronary angioplasty for ostial stenosis of the left coronary artery
- Rotational Atherectomy through Inner Guiding Catheter System for 1.25 mm Rotational Burr Non-Crossable Heavily Calcified Coronary Stenosis
- Experience in High Speed Rotational Coronary Atherectomy
