J Korean Neurosurg Soc.
2021 Jul;64(4):524-533. 10.3340/jkns.2020.0215.
Postoperative Clipping Status after a Pterional versus Interhemispheric Approach for High-Positioned Anterior Communicating Artery Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, School of Medicine, Kyungpook National University, Daegu, Korea
- KMID: 2517685
- DOI: http://doi.org/10.3340/jkns.2020.0215
Abstract
Objective
: When treating high-positioned anterior communicating artery (ACoA) aneurysms, pterional-transsylvian and interhemispheric approaches are both viable options, yet comparative studies of these two surgical approaches are rare. Accordingly, this retrospective study investigated the surgical results of both approaches.
Methods
: Twenty-four patients underwent a pterional approach (n=11) or interhemispheric approach (n=13), including a unilateral low anterior interhemispheric approach or bifrontal interhemispheric approach, for high-positioned ACoA aneurysms with an aneurysm dome height >15 mm and aneurysm neck height >10 mm both measured from the level of the anterior clinoid process. The clinical and radiological data were reviewed to investigate the surgical results and risk factors of incomplete clipping.
Results
: The pterional patient group showed a significantly higher incidence of incomplete clipping than the interhemispheric patient group (p=0.031). Four patients (36.4%) who underwent a pterional approach showed a postclipping aneurysm remnant, whereas all the patients who experienced an interhemispheric approach showed complete clipping. In one case, the aneurysm remnant was obliterated by coiling, while follow-up of the other three cases showed the remnants remained limited to the aneurysm base. A multivariate analysis revealed that a pterional approach for a large aneurysm with a diameter >8 mm presented a statistically significant risk factor for incomplete clipping.
Conclusion
: For high-positioned ACoA aneurysms with a dome height >15 mm and neck height >10 mm above the level of the anterior clinoid process, a large aneurysm with a diameter >8 mm can be clipped more completely via an interhemispheric approach than via a pterional approach.
Figure
-
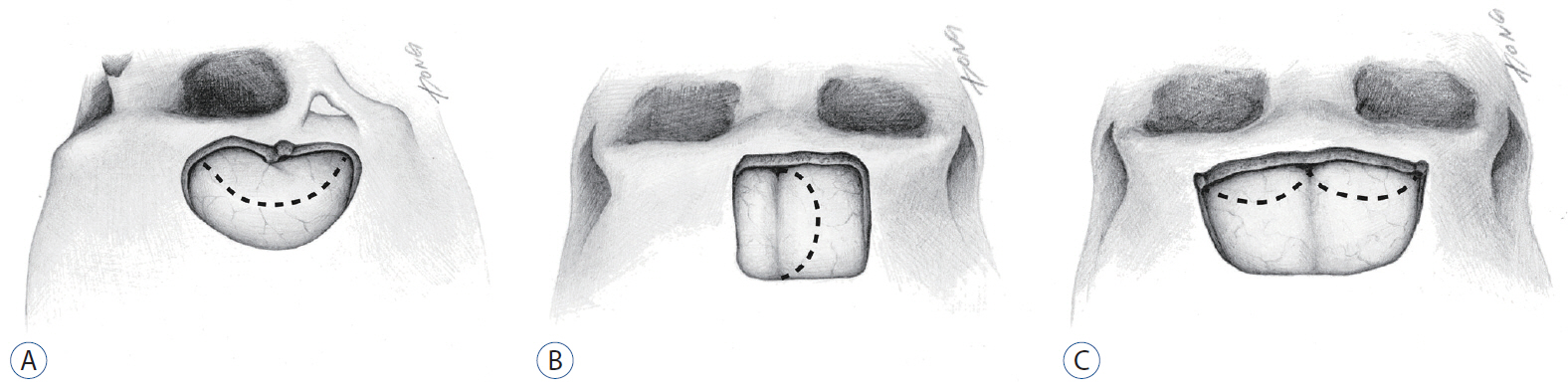
Fig. 1. Illustrations depicting the craniotomies for high-positioned anterior communicating artery aneurysms. A : Pterional approach. B : Unilateral low anterior interhemispheric approach. C : Subfrontal interhemispheric approach. Dotted lines show dural incision.

Fig. 2. Case 1 with incomplete clipping. A : DSA showing a ruptured high-positioned ACoA aneurysm (arrow) with a diameter of 8.8 mm. B : Postoperative DSA showing the incompletely clipped ACoA aneurysm with a remnant (arrow). DSA : digital subtraction angiography, ACoA : anterior communicating artery.
Reference
-
References
1. Alexander MP, Freedman M. Amnesia after anterior communicating artery aneurysm rupture. Neurology. 34:752–757. 1984.
Article2. Benke T, Köylü B, Delazer M, Trinka E, Kemmler G. Cholinergic treatment of amnesia following basal forebrain lesion due to aneurysm rupture--an open-label pilot study. Eur J Neurol. 12:791–796. 2005.
Article3. Birknes JK, Hwang SK, Pandey AS, Cockroft K, Dyer AM, Benitez RP, et al. Feasibility and limitations of endovascular coil embolization of anterior communicating artery aneurysms: morphological considerations. Neurosurgery. 59:43–52. discussion 43-52. 2006.
Article4. Diraz A, Kobayashi S, Toriyama T, Ohsawa M, Hokama M, Kitazama K. Surgical approaches to the anterior communicating artery aneurysm and their results. Neurol Res. 15:273–280. 1993.
Article5. El-Noamany H, Nakagawa F, Hongo K, Kakizawa Y, Kobayashi S. Low anterior interhemispheric approach--a narrow corridor to aneurysms of the anterior communicating artery. Acta Neurochir (Wien). 143:885–891. 2001.
Article6. Fontanella MM, Bergamasco L, Perozzo P, Priano L, Vighetti S, Griva F, et al. Neuropsychological and neurophysiological evaluation after anterior communicating artery (ACoA) aneurysm surgery. J Neurosurg Sci. 44:61–66. discussion 66-67. 2000.7. Fujitsu K, Sekino T, Sakata K, Kawasaki T. Basal interfalcine approach through a frontal sinusotomy with vein and nerve preservation. Technical note. J Neurosurg. 80:575–579. 1994.
Article8. Fujiwara H, Yasui N, Nathal-Vera E, Suzuki A. Anosmia after anterior communicating artery aneurysm surgery: comparison between the anterior interhemispheric and basal interhemispheric approaches. Neurosurgery. 38:325–328. 1996.
Article9. Gonzalez LF, Crawford NR, Horgan MA, Deshmukh P, Zabramski JM, Spetzler RF. Working area and angle of attack in three cranial base approaches: pterional, orbitozygomatic, and maxillary extension of the orbitozygomatic approach. Neurosurgery. 50:550–555. discussion 555-557. 2002.
Article10. Guglielmi G, Viñuela F, Duckwiler G, Jahan R, Cotroneo E, Gigli R. Endovascular treatment of 306 anterior communicating artery aneurysms: overall, perioperative results. J Neurosurg. 110:874–879. 2009.
Article11. Hayashi N, Sato H, Akioka N, Kurosaki K, Hori S, Endo S. Unilateral anterior interhemispheric approach for anterior communicating artery aneurysms with horizontal head position--technical note. Neurol Med Chir (Tokyo). 51:160–163. 2011.
Article12. Hedman AM, van Haren NE, Schnack HG, Kahn RS, Hulshoff Pol HE. Human brain changes across the life span: a review of 56 longitudinal magnetic resonance imaging studies. Hum Brain Mapp. 33:1987–2002. 2012.
Article13. Hernesniemi J, Dashti R, Lehecka M, Niemelä M, Rinne J, Lehto H, et al. Microneurosurgical management of anterior communicating artery aneurysms. Surg Neurol. 70:8–28. discussion 29. 2008.
Article14. Horikoshi T, Nukui H, Mitsuka S, Kaneko M. Partial resection of the gyrus rectus in pterional approach to anterior communicating artery aneurysms. Neurol Med Chir (Tokyo). 32:136–139. 1992.
Article15. Ito Z. The microsurgical anterior interhemispheric approach suitably applied to ruptured aneurysms of the anterior communicating artery in the acute stage. Acta Neurochir (Wien). 63:85–99. 1982.
Article16. Joo MS, Park DS, Moon CT, Chun YI, Song SW, Roh HG. Relationship between gyrus rectus resection and cognitive impairment after surgery for ruptured anterior communicating artery aneurysms. J Cerebrovasc Endovasc Neurosurg. 18:223–228. 2016.
Article17. Kashimura H, Kubo Y, Ogasawara K, Kakino S, Yoshida K, Ogawa A. Easy dissection of the interhemispheric fissure for treatment of the anterior communicating artery aneurysm by the pterional approach. World Neurosurg. 73:688–690. 2010.
Article18. Kempe LG, VanderArk GD. Anterior communicating artery aneurysms. Gyrus rectus approach. Neurochirurgia (Stuttg). 14:63–70. 1971.
Article19. Keogh AJ, Sharma RR, Vanner GK. The anterior interhemispheric trephine approach to anterior midline aneurysms: results of treatment in 72 consecutive patients. Br J Neurosurg. 7:5–12. 1993.
Article20. Kikuchi K, Watanabe K. Modified bifrontal interhemispheric approach to aneurysms of the anterior communicating artery with the use of a trephine craniotomy. A review of personal experience with 25 cases. Acta Neurochir (Wien). 125:127–131. 1993.
Article21. Kim BM, Park SI, Kim DJ, Kim DI, Suh SH, Kwon TH, et al. Endovascular coil embolization of aneurysms with a branch incorporated into the sac. AJNR Am J Neuroradiol. 31:145–151. 2010.
Article22. Kim H, Kim TS, Joo SP, Moon HS. Pterional-subolfactory approach for treatment of high positioned anterior communicating artery aneurysms. J Cerebrovasc Endovasc Neurosurg. 15:177–183. 2013.
Article23. Lawton MT. Seven Aneurysms: Tenets and Techniques for Clipping. New York: Thieme Medical Publishers, Inc;2011. p. 94–120.24. Long X, Liao W, Jiang C, Liang D, Qiu B, Zhang L. Healthy aging: an automatic analysis of global and regional morphological alterations of human brain. Acad Radiol. 19:785–793. 2012.25. Lubicz B, Lefranc F, Levivier M, Dewitte O, Pirotte B, Brotchi J, et al. Endovascular treatment of intracranial aneurysms with a branch arising from the sac. AJNR Am J Neuroradiol. 27:142–147. 2006.26. Mavaddat N, Sahakian BJ, Hutchinson PJ, Kirkpatrick PJ. Cognition following subarachnoid hemorrhage from anterior communicating artery aneurysm: relation to timing of surgery. J Neurosurg. 91:402–407. 1999.
Article27. Moret J, Pierot L, Boulin A, Castaings L, Rey A. Endovascular treatment of anterior communicating artery aneurysms using Guglielmi detachable coils. Neuroradiology. 38:800–805. 1996.
Article28. Murayama Y, Nien YL, Duckwiler G, Gobin YP, Jahan R, Frazee J, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years’ experience. J Neurosurg. 98:959–966. 2003.
Article29. O’Connor MG, Lafleche GM. Retrograde amnesia in patients with rupture and surgical repair of anterior communicating artery aneurysms. J Int Neuropsychol Soc. 10:221–229. 2004.
Article30. Park J, Hamm I. Anterior interhemispheric approach for distal anterior cerebral artery aneurysm surgery: preoperative analysis of the venous anatomy can help to avoid venous infarction. Acta Neurochir. 146:973–977. 2004.
Article31. Park J, Son W, Goh DH, Kang DH, Lee J, Shin IH. Height of aneurysm neck and estimated extent of brain retraction: powerful predictors of olfactory dysfunction after surgery for unruptured anterior communicating artery aneurysms. J Neurosurg. 124:720–725. 2016.
Article32. Proust F, Martinaud O, Gérardin E, Derrey S, Levèque S, Bioux S, et al. Quality of life and brain damage after microsurgical clip occlusion or endovascular coil embolization for ruptured anterior communicating artery aneurysms: neuropsychological assessment. J Neurosurg. 110:19–29. 2009.
Article33. Ravnik J, Starovasnik B, Sesok S, Pirtosek Z, Svigelj V, Bunc G, et al. Long-term cognitive deficits in patients with good outcomes after aneurysmal subarachnoid hemorrhage from anterior communicating artery. Croat Med J. 47:253–263. 2006.34. Sindou M, Auque J. The intracranial venous system as a neurosurgeon’s perspective. In : Cohadon F, editor. Advances and Technical Standards in Neurosurgery. New York: Springer;2000. 26:p. 131–216.35. Srour A, el Tantawi AM, Khouja N, Zouaoui A, Lassau JP, Philippon J, et al. Neurosurgical anatomy of the anterior interhemispheric approach for aneurysms of the anterior communicating artery (26.6.92). Surg Radiol Anat. 16:117–119. 1994.
Article36. Stenhouse LM, Knight RG, Longmore BE, Bishara SN. Long-term cognitive deficits in patients after surgery on aneurysms of the anterior communicating artery. J Neurol Neurosurg Psychiatry. 54:909–914. 1991.
Article37. Suzuki J, Mizoi K, Yoshimoto T. Bifrontal interhemispheric approach to aneurysms of the anterior communicating artery. J Neurosurg. 64:183–190. 1986.
Article38. Wright RA, Boeve BF, Malec JF. Amnesia after basal forebrain damage due to anterior communicating artery aneurysm rupture. J Clin Neurosci. 6:511–515. 1999.
Article39. Yasui N, Nathal E, Fujiwara H, Suzuki A. The basal interhemispheric approach for acute anterior communicating aneurysms. Acta Neurochir (Wien). 118:91–97. 1992.
Article40. Yeh H, Tew JM Jr. Anterior interhemispheric approach to aneurysms of the anterior communicating artery. Surg Neurol. 23:98–100. 1985.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Interhemispheric Approach for Intracranial Aneurysms
- Pterional-subolfactory Approach for Treatment of High Positioned Anterior Communicating Artery Aneurysms
- Pterional or Subfrontal Access for Proximal Vascular Control in Anterior Interhemispheric Approach for Ruptured Pericallosal Artery Aneurysms at Risk of Premature Rupture
- Clinical Assessment of Surgical Approaches for the High Positioned Anterior Communicating Artery Aneurysms
- The Optimal Surgical Direction Concerning the Pterional Approach to the Anterior Communicating Artery Aneurysms
