Indication and surgical techniques of bypass choledochojejunostomy for intractable choledocholithiasis
- Affiliations
-
- 1Departments of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Departments of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2516247
- DOI: http://doi.org/10.14701/ahbps.2021.25.2.259
Abstract
- Despite development in endoscopic treatment and minimally invasive surgery for choledocholithiasis, there remains a small number of patients who require bypass Roux-en-Y choledochojejunostomy (RYCJ) because of the intractable occurrence of common bile duct (CBD) stones. We herein present the detailed procedures of open RYCJ customized for intractable choledocholithiasis. The first method is a side-to-end choledochojejunostomy with intraluminal closure of the distal CBD. This method was applied to a 79-year-old female patient who underwent endoscopic retrograde cholangiopancreatography (ERCP) more than 10 times in the past 14 years (Case No. 1). The distal CBD was explored through choledochotomy and then the distal CBD lumen was occluded with internal running sutures. A large-sized choledochojejunostomy was performed. The patient recovered uneventfully and has been doing well for the past 2 years. The second method is an end-to-end choledochojejunostomy with segmental CBD resection. It was applied to a 75-year-old male patient who underwent ERCP 9 times in the past 10 years (Case No. 2). The CBD was resected segmentally and a large-sized choledochojejunostomy was performed. The patient also recovered uneventfully and has been doing well for the past 2 years. In conclusion, the primary indication of bypass RYCJ is intractable choledocholithiasis which requires numerous sessions of endoscopic stone removal over a long period. Open RYCJ is the preferred procedure to date. If the papilla is patulous, the distal CBD should be occluded or resected to prevent reflux ascending cholangitis. We recommend to resect the intrapancreatic distal CBD if it is markedly dilated like choledochal cyst.
Keyword
Figure
-
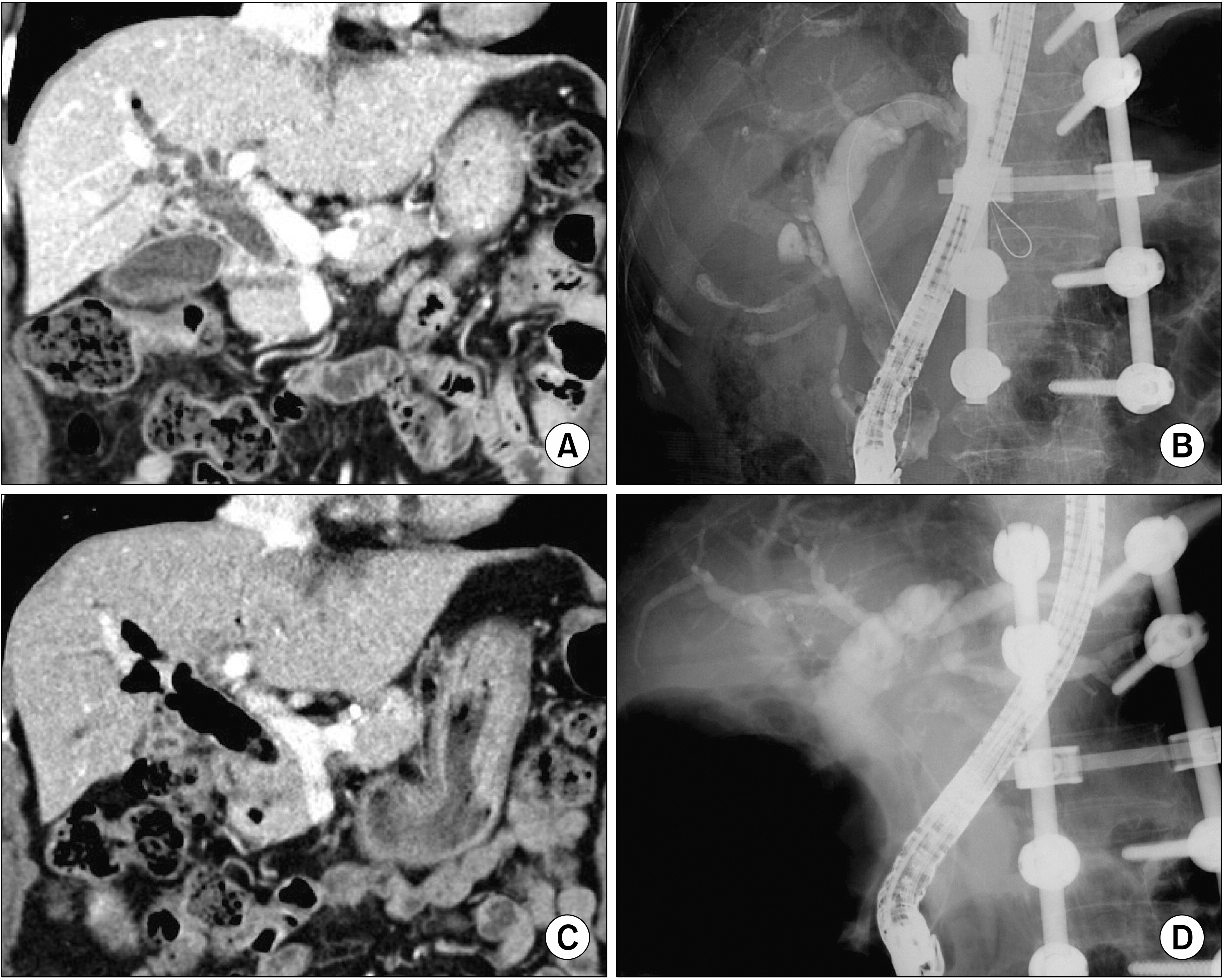
Fig. 1 The preoperative finding of Case No. 1. Computed tomo-graphy (CT) and endoscopic retrograde cholangiopancreato-graphy (ERCP) taken 7 years before surgery (A, B) show marked dilatation of the com-mon bile duct with the patulous sphincter. CT scan and ERCP taken 1 month before surgery (C, D) show further dilatation of the common bile duct filled with air and sludges, indicating reflux ascending cholangitis. The spine was externally fixed 11 years before due to spine fracture.

Fig. 2 Intraoperative photograph showing the procedure of side-to-end choledochojejunostomy with intraluminal closure of the distal common bile duct (CBD) in Case No. 1. (A) The dilated CBD is visible after cholecystectomy. (B) The mid-portion of the CBD is incised longitudinally, showing markedly thickened CBD wall indicating repeated episodes of cholangitis. (C) The distal CBD is explored with curved stone forceps to examine the opening status of the sphincter. (D, E) The lumen of the distal CBD at the upper board of the pancreas is securely closed with 5-0 Prolene running sutures twice. The suture knots are made at the outer surface of the CBD (arrow). A part of the anterior wall of the CBD is excised to widen the opening. (F-H) A Roux-en-Y jejunal limb is anastomosed to the CBD opening in a side-to-side fashion.
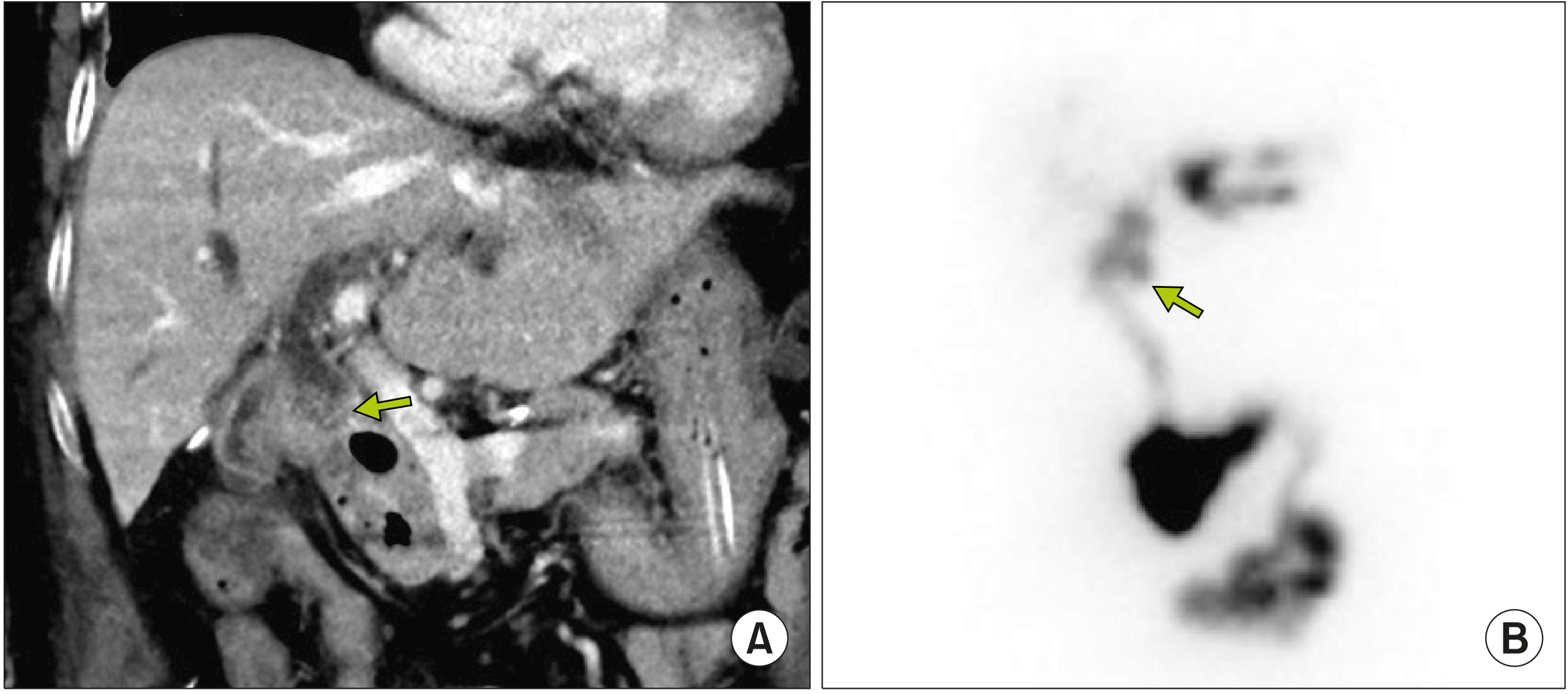
Fig. 3 Postoperative findings at two weeks after surgery in Case No. 1. (A) Computed tomography scan shows uneventful drainage of the bile from to proximal common bile duct (CBD) to the jejunal limb. The distal CBD is occluded (arrow). (B) Hepato-biliary scintigraphy shows a normal biliary excretion rate of 92.5% at 90 minutes. The distal CBD is occluded (arrow).
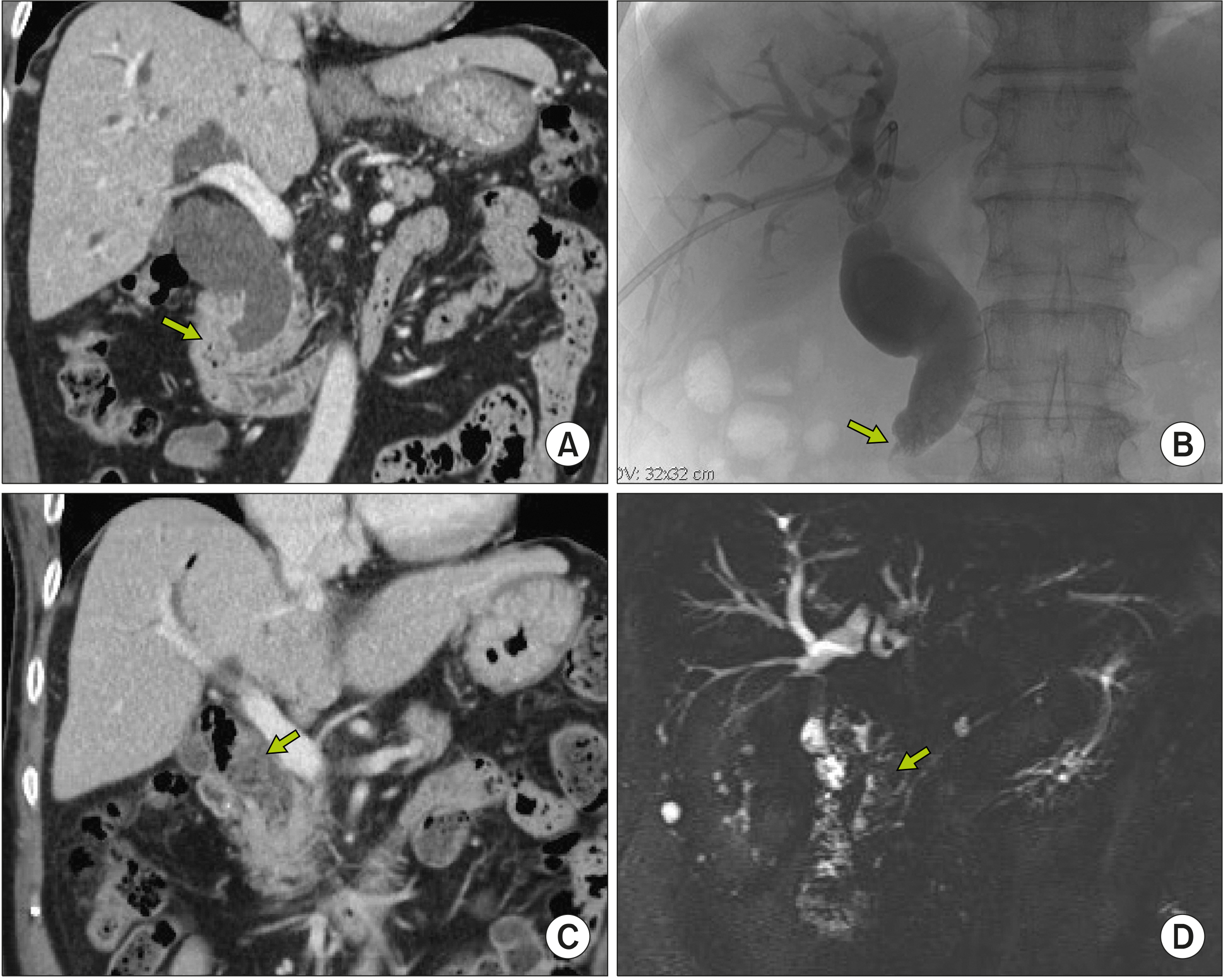
Fig. 4 The preoperative finding of Case No. 2. Computed tomo-graphy (CT) and direct cholan-giography taken 10 years before surgery (A, B) show marked dilatation of the common bile duct with an obstructing mass at the sphincter (arrows), which was later proven to be a benign stricture. CT scan and magnetic resonance cholangiography taken 1 month before surgery (C, D) show that the common bile duct is filled with stones and sludges (arrows).
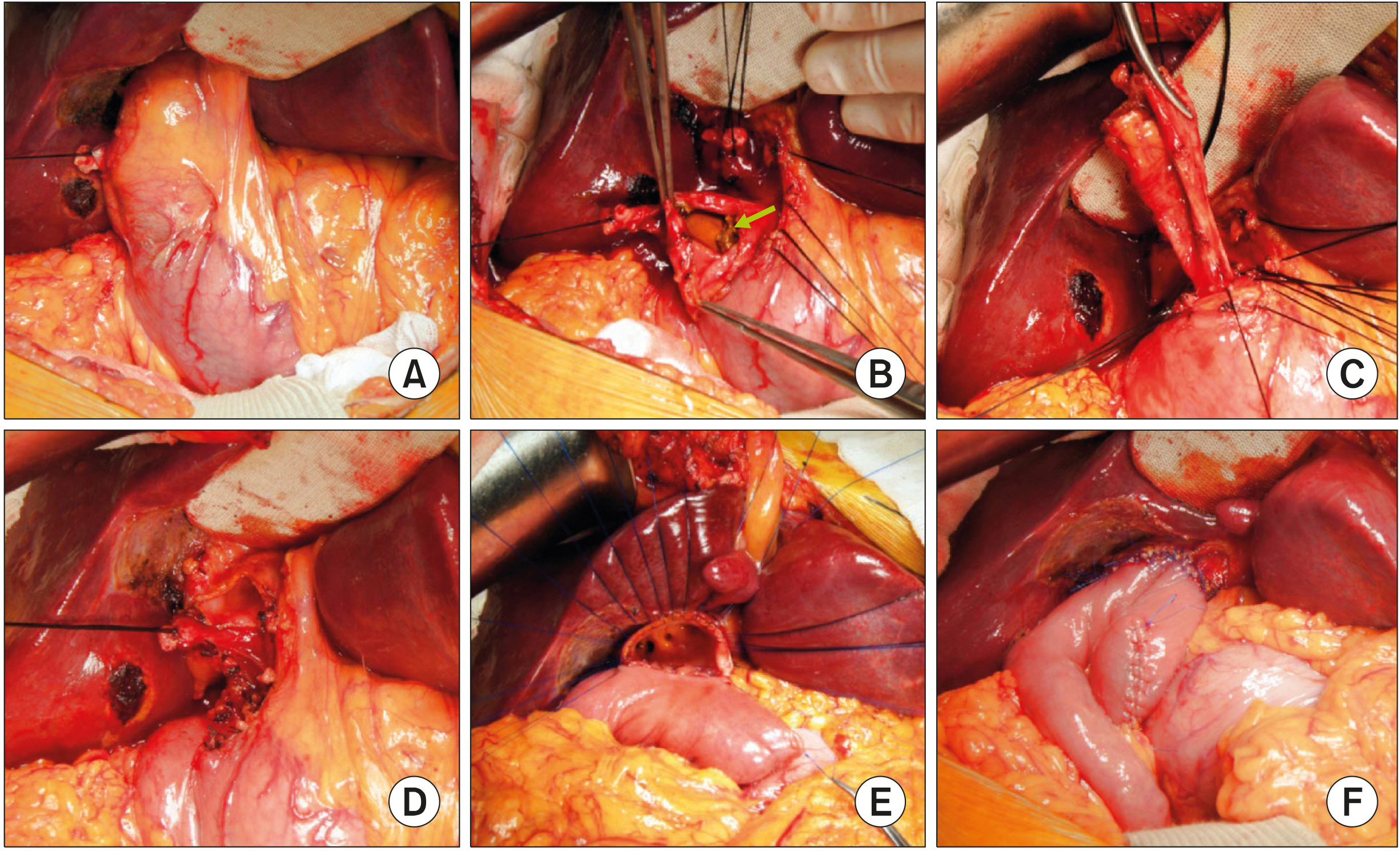
Fig. 5 Intraoperative photograph showing the procedure of end-to-end choledochojejunostomy with segmental resection of the common bile duct (CBD) in Case No. 2. (A) The dilated CBD is visible after cholecystectomy. (B) The mid-portion of the CBD is incised longitudinally, showing multiple CBD stones and sludges. (C) The distal CBD is dissected and transected at the narrow portion of the intrapancreatic bile duct, and then securely closed with 5-0 Prolene sutures. (D) The proximal CBD was also transected at the level of the right hepatic artery to make a large proximal bile duct opening. (E, F) A Roux-en-Y jejunal limb is anastomosed to the CBD opening in an end-to-side fashion.

Fig. 6 Postoperative findings at 10 days after surgery in Case No. 2. (A) Computed tomogra-phy shows uneventful drainage of the bile from to proximal common bile duct to the jejunal limb. (B) Hepatobiliary scinti-graphy shows a biliary excre-tion rate of 89.2% at 90 min-utes.
Reference
-
1. Costi R, Gnocchi A, Di Mario F, Sarli L. 2014; Diagnosis and management of choledocholithiasis in the golden age of imaging, endoscopy and laparoscopy. World J Gastroenterol. 20:13382–13401. DOI: 10.3748/wjg.v20.i37.13382. PMID: 25309071. PMCID: PMC4188892.
Article2. Nathanson LK, O'Rourke NA, Martin IJ, Fielding GA, Cowen AE, Roberts RK, et al. 2005; Postoperative ERCP versus laparoscopic choledochotomy for clearance of selected bile duct calculi: a randomized trial. Ann Surg. 242:188–192. DOI: 10.1097/01.sla.0000171035.57236.d7. PMID: 16041208. PMCID: PMC1357723.3. Urbach DR, Khajanchee YS, Jobe BA, Standage BA, Hansen PD, Swanstrom LL. 2001; Cost-effective management of common bile duct stones: a decision analysis of the use of endoscopic retrograde cholangiopancreatography (ERCP), intraoperative cholangiography, and laparoscopic bile duct exploration. Surg Endosc. 15:4–13. DOI: 10.1007/s004640000322. PMID: 11178753.4. Pring CM, Skelding-Millar L, Goodall RJ. 2005; Expectant treatment or cholecystectomy after endoscopic retrograde cholangiopancreatography for choledocholithiasis in patients over 80 years old? Surg Endosc. 19:357–360. DOI: 10.1007/s00464-004-9089-1. PMID: 15645324.
Article5. Maple JT, Ikenberry SO, Anderson MA, Appalaneni V, Decker GA, Early D, et al. 2011; The role of endoscopy in the management of choledocholithiasis. Gastrointest Endosc. 74:731–744. DOI: 10.1016/j.gie.2011.04.012. PMID: 21951472.
Article6. Shim CS. 2010; How should biliary stones be managed? Gut Liver. 4:161–172. DOI: 10.5009/gnl.2010.4.2.161. PMID: 20559517. PMCID: PMC2886934.
Article7. Sugiyama M, Atomi Y. 2000; Endoscopic sphincterotomy for bile duct stones in patients 90 years of age and older. Gastrointest Endosc. 52:187–191. DOI: 10.1067/mge.2000.107285. PMID: 10922089.
Article8. Moon JH, Cha SW, Ryu CB, Kim YS, Hong SJ, Cheon YK, et al. 2004; Endoscopic treatment of retained bile-duct stones by using a balloon catheter for electrohydraulic lithotripsy without cholangioscopy. Gastrointest Endosc. 60:562–566. DOI: 10.1016/S0016-5107(04)02012-7.
Article9. Sugiyama M, Suzuki Y, Abe N, Masaki T, Mori T, Atomi Y. 2004; Endoscopic retreatment of recurrent choledocholithiasis after sphincterotomy. Gut. 53:1856–1859. DOI: 10.1136/gut.2004.041020. PMID: 15542528. PMCID: PMC1774317.
Article10. Kadaba RS, Bowers KA, Khorsandi S, Hutchins RR, Abraham AT, Sarker SJ, et al. 2017; Complications of biliary-enteric anastomoses. Ann R Coll Surg Engl. 99:210–215. DOI: 10.1308/rcsann.2016.0293. PMID: 27659373. PMCID: PMC5450270.
Article11. Vogt DP, Hermann RE. 1981; Choledochoduodenostomy, choledochojejunostomy or sphincteroplasty for biliary and pancreatic disease. Ann Surg. 193:161–168. DOI: 10.1097/00000658-198102000-00006. PMID: 7469551. PMCID: PMC1345035.
Article12. Hori T, Aisu Y, Yamamoto M, Yasukawa D, Iida T, Yagi S, et al. 2019; Laparoscopic approach for choledochojejunostomy. Hepatobiliary Pancreat Dis Int. 18:285–288. DOI: 10.1016/j.hbpd.2019.04.004. PMID: 31023579.
Article13. Hori T. 2019; Comprehensive and innovative techniques for laparoscopic choledocholithotomy: a surgical guide to successfully accomplish this advanced manipulation. World J Gastroenterol. 25:1531–1549. DOI: 10.3748/wjg.v25.i13.1531. PMID: 30983814. PMCID: PMC6452235.
Article14. Han HS, Yi NJ. 2004; Laparoscopic Roux-en-Y choledochojejunostomy for benign biliary disease. Surg Laparosc Endosc Percutan Tech. 14:80–84. DOI: 10.1097/00129689-200404000-00006. PMID: 15287605.
Article15. Ruurda JP, van Dongen KW, Dries J, Borel Rinkes IH, Broeders IA. 2003; Robot-assisted laparoscopic choledochojejunostomy. Surg Endosc. 17:1937–1942. DOI: 10.1007/s00464-003-9008-x. PMID: 14569457.
Article16. Benzie AL, Sucandy I, Spence J, Ross S, Rosemurgy A. 2019; Robotic choledochoduodenostomy for benign distal common bile duct stricture: how we do it. J Robot Surg. 13:713–716. DOI: 10.1007/s11701-019-00957-8. PMID: 30989618.
Article17. Misra SP, Dwivedi M. 2009; Reflux of duodenal contents and cholangitis in patients undergoing self-expanding metal stent placement. Gastrointest Endosc. 70:317–321. DOI: 10.1016/j.gie.2008.12.054. PMID: 19539920.
Article18. Hwang S, Ha TY, Song GW, Jung DH. 2016; Cluster hepaticojejunostomy with radial spreading anchoring traction technique for secure reconstruction of widely opened hilar bile ducts. Korean J Hepatobiliary Pancreat Surg. 20:66–70. DOI: 10.14701/kjhbps.2016.20.2.66. PMID: 27212993. PMCID: PMC4874047.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Study of Residual Stone in Choledocholithiasis
- A clinical review of choledocholithiasis
- Optimal Evaluation of Suspected Choledocholithiasis: Does This Patient Really Have Choledocholithiasis?
- Surgical Treatments of Benign Paroxysmal Positional Vertigo
- 128 Cases of Endoscopic Sphincterotomy (EST)
