Do Patients Maintain Proper Long-Term Cardiopulmonary Fitness Levels After Cardiac Rehabilitation? A Retrospective Study Using Medical Records
- Affiliations
-
- 1Department of Rehabilitation Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
- 2Department of Rehabilitation Medicine, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
- 3Department of Internal Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
- KMID: 2515396
- DOI: http://doi.org/10.5535/arm.20123
Abstract
Objective
To examine whether patients who participated in a cardiac rehabilitation (CR) program after hospitalization for acute coronary syndrome maintained cardiorespiratory fitness (CRF) in the community.
Methods
We conducted a retrospective study including 78 patients who underwent percutaneous coronary intervention or coronary artery bypass graft surgery at our hospital’s cardiovascular center and participated in a CR program and a 5-year follow-up evaluation. Patients were divided into a center-based CR (CBCR) group, participating in an electrocardiography-monitored exercise training in a hospital setting, and a home-based CR (HBCR) group, receiving aerobic exercise training and performed self-exercise at home.
Results
No significant differences were found between groups (p>0.05), except the proportion of non-smokers (CBCR 59.5% vs. HBCR 31.7%; p=0.01). In both groups, the maximal oxygen consumption (VO2max) increased significantly during the first 12 weeks of follow-up and remained at a steady state for the first year, but it decreased after the 1-year follow-up. Particularly, VO2max at 5 years decreased below the baseline value in the HBCR group. In the low CRF group, the CRF level significantly improved at 12 weeks, peaked at 1 year, and was still significantly different from the baseline value after 5 years. The high CRF group did not show any significant increase over time relative to the baseline value, but most patients in the high CRF group maintained relatively appropriate CRF levels after 5 years.
Conclusion
Continuous support should be provided to patients to maintain optimal CRF levels after completing a CR program.
Figure
-

Fig. 1. Flow diagram of the study participants. ACS, acute coronary syndrome; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft; CPX, cardiopulmonary exercise; CR, cardiac rehabilitation.
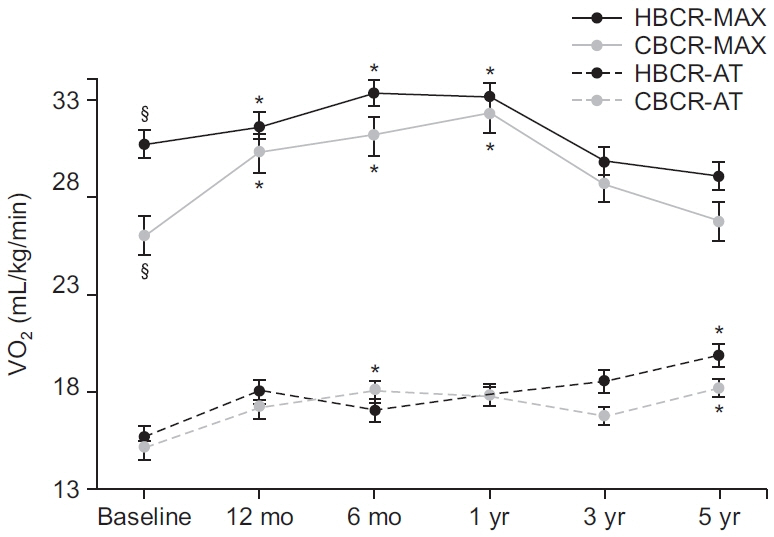
Fig. 2. Five-year trends of VO2max and VO2AT in the CBCR and HBCR groups. CBCR, center-based cardiac rehabilitation; HBCR, home-based cardiac rehabilitation; MAX, maximal oxygen consumption; AT, oxygen consumption at anaerobic threshold. §p<0.05, significant difference between the two groups at the same time. *p<0.05, significantly different from the baseline value.
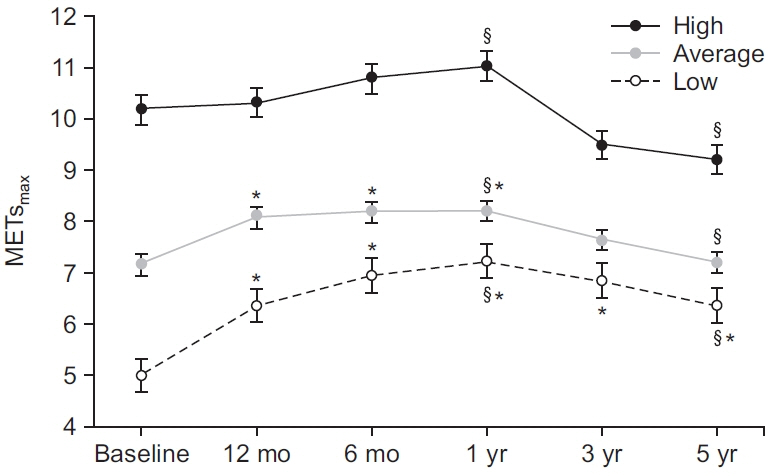
Fig. 3. Five-year trends of maximal metabolic equivalents (METsmax) in three cardiorespiratory fitness groups: high (≥8 METs), average, (≥6 METs and <8 METs), and low (<6 METs). §p<0.05, significant difference between two periods in the same group. *p<0.05, significantly different from the baseline value.
Cited by 3 articles
-
The Effect of Home-Based Cardiac Rehabilitation on Cardiovascular Risk Factors Management
Chul Kim, Seok Hyeon Lee
Ann Rehabil Med. 2023;47(4):272-281. doi: 10.5535/arm.23041.Fact Sheet on Cardiac Rehabilitation for Cardiovascular Disease in South Korea
Ki-Hong Kim, Jae-Young Han
Ann Rehabil Med. 2023;47(5):318-325. doi: 10.5535/arm.23050.The Accessibility and Effect of Cardiac Rehabilitation in COVID-19 Pandemic Era
Chul Kim, Jun Hyeong Song, Seung Hyoun Kim
Ann Rehabil Med. 2024;48(4):249-258. doi: 10.5535/arm.240021.
Reference
-
1. Oldridge NB, Guyatt GH, Fischer ME, Rimm AA. Cardiac rehabilitation after myocardial infarction. Combined experience of randomized clinical trials. JAMA. 1988; 260:945–50.
Article2. Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2001; (1):CD001800.
Article3. Taylor RS, Brown A, Ebrahim S, Jolliffe J, Noorani H, Rees K, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med. 2004; 116:682–92.
Article4. Conn VS, Hafdahl AR, Moore SM, Nielsen PJ, Brown LM. Meta-analysis of interventions to increase physical activity among cardiac subjects. Int J Cardiol. 2009; 133:307–20.
Article5. Kim JH, Chae SC, Oh DJ, Kim HS, Kim YJ, Ahn Y, et al. Multicenter cohort study of acute myocardial infarction in Korea: interim analysis of the Korea Acute Myocardial Infarction Registry–National Institutes of Health Registry. Circ J. 2016; 80:1427–36.6. Smith SC Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association. J Am Coll Cardiol. 2011; 58:2432–46.7. Ibanez B, James S, Agewall S, Antunes MJ, BucciarelliDucci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018; 39:119–77.8. Fujimi K, Imaizumi T, Suematsu Y, Kitajima K, Ueda T, Ishida T, et al. Differential prognostic impact between completion and non-completion of a 5-month cardiac rehabilitation program in outpatients with cardiovascular diseases. Int J Cardiol. 2019; 292:13–8.
Article9. Swift DL, Lavie CJ, Johannsen NM, Arena R, Earnest CP, O’Keefe JH, et al. Physical activity, cardiorespiratory fitness, and exercise training in primary and secondary coronary prevention. Circ J. 2013; 77:281–92.
Article10. Lawler PR, Filion KB, Eisenberg MJ. Efficacy of exercise-based cardiac rehabilitation post-myocardial infarction: a systematic review and meta-analysis of randomized controlled trials. Am Heart J. 2011; 162:571–84.
Article11. Buckingham SA, Taylor RS, Jolly K, Zawada A, Dean SG, Cowie A, et al. Home-based versus centrebased cardiac rehabilitation: abridged Cochrane systematic review and meta-analysis. Open Heart. 2016; 3:e000463.12. American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines for cardiac rehabilitation and secondary prevention programs. Champaign, IL: Human Kinetics;2013.13. Park HK, Kim KH, Kim JH, Song MK, Choi IS, Han JY. Comparison of obesity related index and exercise capacity between center-based and home-based cardiac rehabilitation programs. Ann Rehabil Med. 2019; 43:297–304.
Article14. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009; 301:2024–35.15. Kaminsky LA, Arena R, Myers J. Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing: data from the Fitness Registry and the Importance of Exercise National Database. Mayo Clin Proc. 2015; 90:1515–23.16. Ross R, Blair SN, Arena R, Church TS, Despres JP, Franklin BA, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign: a scientific statement from the American Heart Association. Circulation. 2016; 134:e653–99.
Article17. Ehrman JK, Brawner CA, Al-Mallah MH, Qureshi WT, Blaha MJ, Keteyian SJ. Cardiorespiratory fitness change and mortality risk among black and white patients: Henry Ford Exercise Testing (FIT) Project. Am J Med. 2017; 130:1177–83.
Article18. Smith KM, McKelvie RS, Thorpe KE, Arthur HM. Six-year follow-up of a randomised controlled trial examining hospital versus home-based exercise training after coronary artery bypass graft surgery. Heart. 2011; 97:1169–74.
Article19. Baek S, Ha Y, Mok J, Park HW, Son HR, Jin MS. Community-based cardiac rehabilitation conducted in a public health center in South Korea: a preliminary study. Ann Rehabil Med. 2020; 44:481–92.
Article20. Lee YH, Hur SH, Sohn J, Lee HM, Park NH, Cho YK, et al. Impact of home-based exercise training with wireless monitoring on patients with acute coronary syndrome undergoing percutaneous coronary intervention. J Korean Med Sci. 2013; 28:564–8.
Article21. Huang K, Liu W, He D, Huang B, Xiao D, Peng Y, et al. Telehealth interventions versus center-based cardiac rehabilitation of coronary artery disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2015; 22:959–71.
Article22. Blair SN, Kohl HW 3rd, Barlow CE, Paffenbarger RS Jr, Gibbons LW, Macera CA. Changes in physical fitness and all-cause mortality: a prospective study of healthy and unhealthy men. JAMA. 1995; 273:1093–8.23. Erikssen G, Liestol K, Bjornholt J, Thaulow E, Sandvik L, Erikssen J. Changes in physical fitness and changes in mortality. Lancet. 1998; 352:759–62.
Article24. Lee DC, Sui X, Artero EG, Lee IM, Church TS, McAuley PA, et al. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study. Circulation. 2011; 124:2483–90.25. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002; 346:793–801.
Article26. Balady GJ, Larson MG, Vasan RS, Leip EP, O’Donnell CJ, Levy D. Usefulness of exercise testing in the prediction of coronary disease risk among asymptomatic persons as a function of the Framingham risk score. Circulation. 2004; 110:1920–5.
Article27. Arthur HM, Smith KM, Kodis J, McKelvie R. A controlled trial of hospital versus home-based exercise in cardiac patients. Med Sci Sports Exerc. 2002; 34:1544–50.
Article28. Sandercock G, Hurtado V, Cardoso F. Changes in cardiorespiratory fitness in cardiac rehabilitation patients: a meta-analysis. Int J Cardiol. 2013; 167:894–902.
Article29. Wilson JR, Groves J, Rayos G. Circulatory status and response to cardiac rehabilitation in patients with heart failure. Circulation. 1996; 94:1567–72.
Article30. Kavanagh T, Mertens DJ, Hamm LF, Beyene J, Kennedy J, Corey P, et al. Peak oxygen intake and cardiac mortality in women referred for cardiac rehabilitation. J Am Coll Cardiol. 2003; 42:2139–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Integrating Cardiac Rehabilitation with Neurorehabilitation in a Patient with Ischemic Stroke after Cardiac Surgery: a Case Report
- The Effects of Cardiac Rehabilitation in Patients with ST Elevation Myocardial Infarction and Non-ST Elevation Myocardial Infarction
- Fact Sheet on Cardiac Rehabilitation for Cardiovascular Disease in South Korea
- Lance-Adams Syndrome
- Long-term Prognosis and Neuro-psychosocial Deficits in Post-cardiac arrest Patients
