J Korean Assoc Oral Maxillofac Surg.
2021 Apr;47(2):145-148. 10.5125/jkaoms.2021.47.2.145.
Sialolithiasis of minor salivary gland: a challenging diagnostic dilemma
- Affiliations
-
- 1Department of Oral Medicine and Pathology, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece
- 2Department of Oral and Maxillofacial Surgery, School of Dentistry, University of Athens, Athens, Greece
- KMID: 2515314
- DOI: http://doi.org/10.5125/jkaoms.2021.47.2.145
Abstract
- Minor salivary gland sialolithiasis (MSGS) is a not uncommon oral mucosal disease. Its clinical appearance may mimic a mucocyst or other benign submucosal overgrowth. Stasis of saliva, which accompanies MSGS, usually results in minor salivary gland inflammation, with a chronic sialadenitis appearance. MSGS typically is a painless lesion but can become painful when the salivary gland parenchyma or excretory duct becomes infected, with or without pus. However, misdiagnosis of this condition is rather common, as the clinical appearance is asymptomatic. The most common location is the upper lip, and MSGS affects males and females, with a slight predilection for males. The sialolith causing MSGS may be obvious during surgical excision, as in the case reported. In other cases, sialolith may be absent or fragmented. Differential diagnosis includes mucocele, swelling due to local irritation like fibroma and diapneusia, chronic abscess of the oral mucosa, and neoplasms either benign (lymphangioma, pleiomorphic adenoma) or malignant. Histopathological examination is needed to establish clinical diagnosis.
Keyword
Figure
-

Fig. 1 A whitewish submucosal nodule, on the left side of the upper lip.

Fig. 2 A global (spherical) sialolith, whitish in color avulsed under the excision.
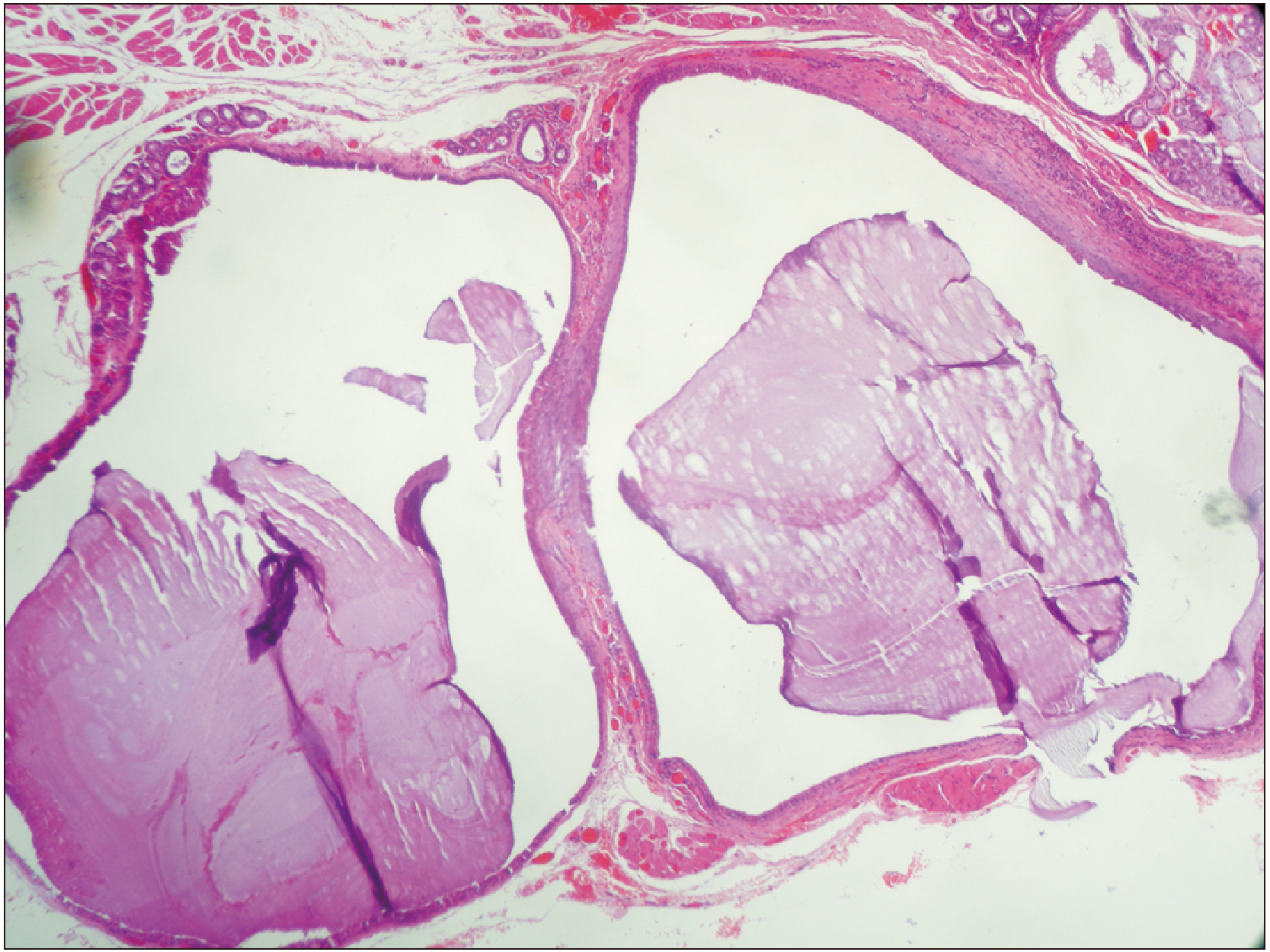
Fig. 3 Chronic sialadenitis with lobular atrophy, ductal dilatation and severe lymphocytic infiltration in stroma with lymph follicle formation (H&E staining, ×100).
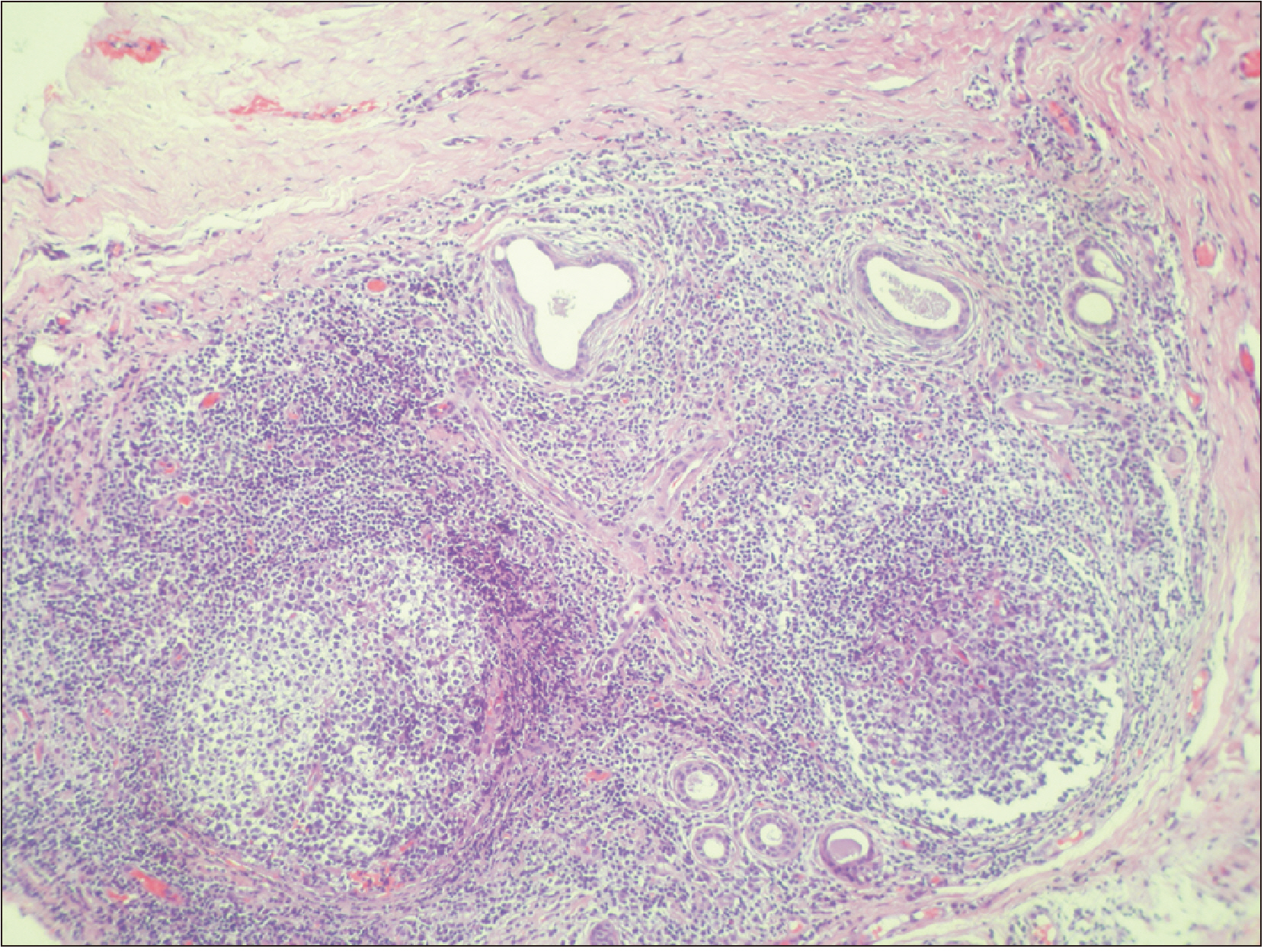
Fig. 4 Chronic sialadenitis, due to sialolithiasis, with severe dilatation of the ducts (H&E staining, ×50).
Reference
-
References
1. van der Waal I. 1971; Sialolithiasis of minor salivary glands: how rare? Report of two cases. J Oral Surg. 29:815–6. PMID: 5286538.2. Pullon PA, Miller AS. 1972; Sialolithiasis of accessory salivary glands: review of 55 cases. J Oral Surg. 30:832–4. PMID: 4507238.3. Ben Lagha N, Alantar A, Samson J, Chapireau D, Maman L. 2005; Lithiasis of minor salivary glands: current data. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 100:345–8. https://doi.org/10.1016/j.tripleo.2004.12.023 . DOI: 10.1016/j.tripleo.2004.12.023. PMID: 16122664.
Article4. Holst E. 1971; The clinical entity of sialolithiasis of the minor salivary glands. Acta Odontol Scand. 29:75–84. https://doi.org/10.3109/00016357109026324 . DOI: 10.3109/00016357109026324. PMID: 5280619.
Article5. Anneroth G, Hansen LS. 1983; Minor salivary gland calculi. A clinical and histopathological study of 49 cases. Int J Oral Surg. 12:80–9. https://doi.org/10.1016/s0300-9785(83)80002-7 . DOI: 10.1016/s0300-9785(83)80002-7. PMID: 6409828.
Article6. Brazao-Silva MT, Prosdocimi FC, Lemos-Junior CA, de Sousa SO. 2015; Clinicopathological aspects of 25 cases of sialolithiasis of minor salivary glands. Gen Dent. 63:e22–6. PMID: 25945774.7. Wang WC, Chen CY, Hsu HJ, Kuo JH, Lin LM, Chen YK. 2016; Sialolithiasis of minor salivary glands: a review of 17 cases. J Dent Sci. 11:152–5. https://doi.org/10.1016/j.jds.2015.10.006 . DOI: 10.1016/j.jds.2015.10.006. PMID: 30894964. PMCID: PMC6395286.
Article8. Lee LT, Wong YK. 2010; Pathogenesis and diverse histologic findings of sialolithiasis in minor salivary glands. J Oral Maxillofac Surg. 68:465–70. https://doi.org/10.1016/j.joms.2009.03.041 . DOI: 10.1016/j.joms.2009.03.041. PMID: 20116725.
Article9. Ng SY, Pinto P. 2000; Ultrasound-guided retrieval of labial minor salivary gland sialoliths. Dentomaxillofac Radiol. 29:319–22. https://doi.org/10.1038/sj/dmfr/4600545 . DOI: 10.1038/sj/dmfr/4600545. PMID: 10980569.
Article10. Okada H, Yokokawa M, Komiya M, Akimoto Y, Kaneda T, Yamamoto H. 2011; A rare case of sialolithiasis of the lower lip simulating a mucocele and review of the literature. Quintessence Int. 42:589–94. PMID: 21716987.11. Boyd AS. 2013; Sialolith of a minor salivary gland. J Cutan Pathol. 40:695–8. DOI: 10.1111/cup.12191. PMID: 23859700.
Article12. Suh DW, Lee EJ, Lew BL, Sim WY. 2013; Minor salivary gland sialolithiasis of the upper lip. Ann Dermatol. 25:502–4. https://doi.org/10.5021/ad.2013.25.4.502 . DOI: 10.5021/ad.2013.25.4.502. PMID: 24371404. PMCID: PMC3870225.
Article13. Barnett ML. 1971; Sialolithiasis of a labial gland. Oral Surg Oral Med Oral Pathol. 32:22–8. https://doi.org/10.1016/0030-4220(71)90246-5 . DOI: 10.1016/0030-4220(71)90246-5. PMID: 5281554.
Article14. Ho V, Currie WJ, Walker A. 1992; Sialolithiasis of minor salivary glands. Br J Oral Maxillofac Surg. 30:273–5. https://doi.org/10.1016/0266-4356(92)90275-n . DOI: 10.1016/0266-4356(92)90275-n. PMID: 1510906.
Article15. Su CH, Lee KS, Tseng TM, Hung SH. 2015; Endoscopic holmium:YAG laser-assisted lithotripsy: a preliminary report. B-ENT. 11:57–61. PMID: 26513949.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple sialolithiasis in sublingual gland: report of a case
- Minor Salivary Gland Sialolithiasis of the Upper Lip
- Recurrent Sialolithiasis on Remnant Wharton's Duct Following Submandibular Gland Resection
- Sialolithiasis Mimicking Metastatic Thyroid Cancer
- A Case of Multiple Sialoliths in Sublingual Gland Misdiagnosed as Sialoliths in Submandibular Gland
