Temporomandibular joint reconstruction with costochondral graft: case series study
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, College of Dentistry, Wonkwang University, Iksan, Korea
- KMID: 2515311
- DOI: http://doi.org/10.5125/jkaoms.2021.47.2.128
Abstract
- Various techniques have been used to reconstruct the temporomandibular joints, including autogenous transplants and alloplastic implants. Among autogenous grafts, costochondral grafts have mainly been used. A costochondral graft has many advantages over other autogenous grafts and alloplastic implants. Harvest is easy and has minimal impact on patients. The graft can bear functional load well and biocompatibility is excellent. A costochondral graft obviates foreign body reactions and further surgery for revision of alloplastic replacements if the graft takes well. Although long-term prognosis remains unclear, it appears that for autogenous condylar reconstruction, costochondral grafts can be used with few complications and acceptable results. This article describes cases and discusses surgical techniques and considerations related to costochondral grafts.
Figure
-
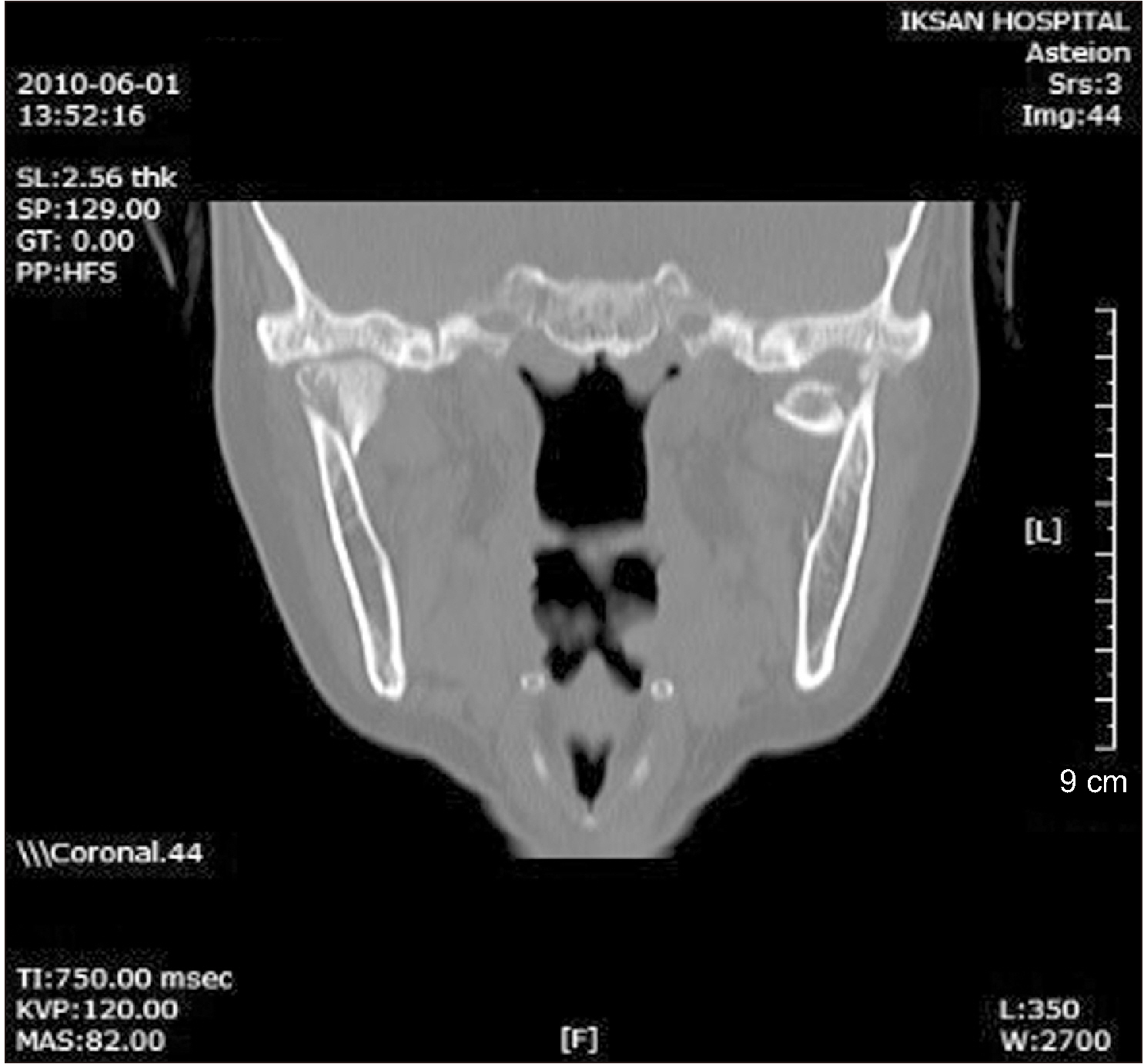
Fig. 1 On computed tomography, bilateral intracapsular condylar fractures were observed.
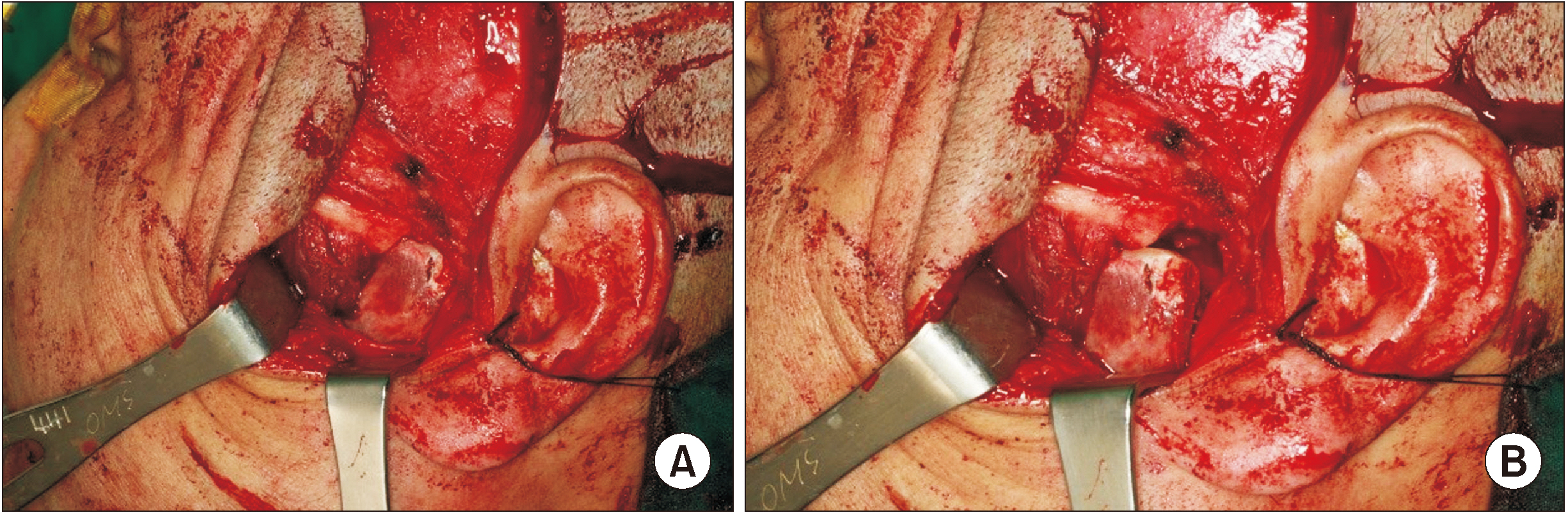
Fig. 2 A. Trimmed end portion of the costochondral graft loosely contacted the temporomandibular joint in the centric occlusion state. B. Trimmed end portion of the costochondral graft moved along the articular fossa as mouth opening increased.
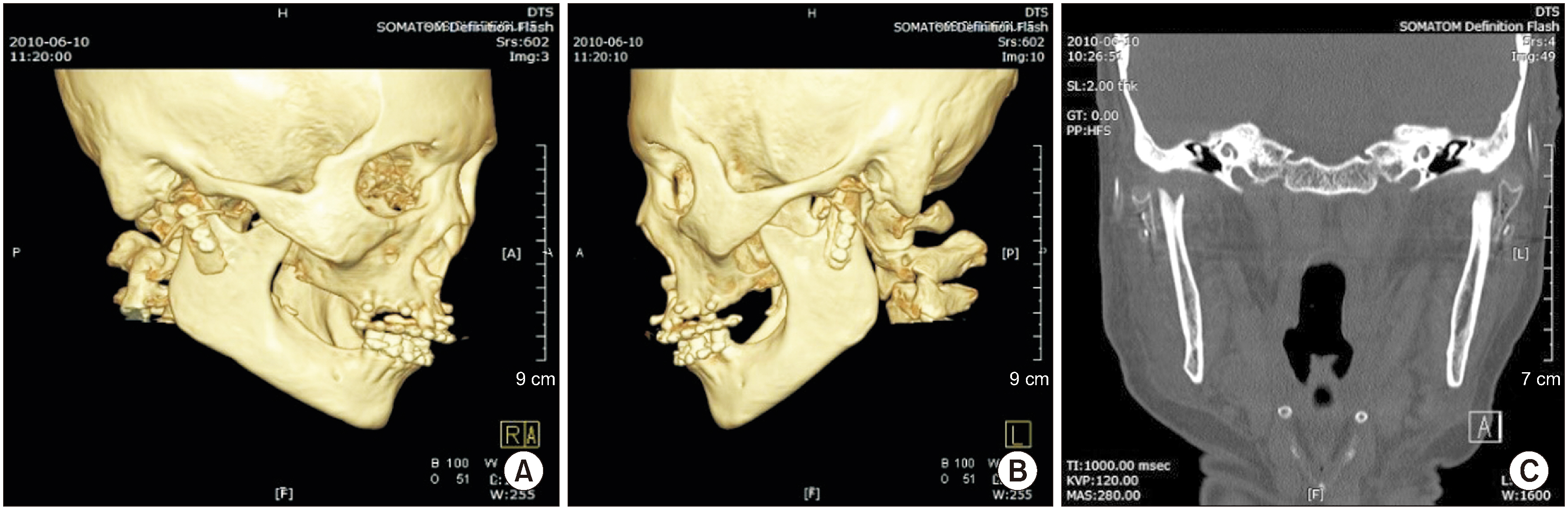
Fig. 3 A, B. On three-dimensional computed tomography, the costochondral graft was fixed in a good position. C. On coronal plane view, costochondral grafts were positioned on the lateral surface of the articular fossa.

Fig. 4 At the last visit, the patient showed near normal mandibular excursion and protrusion.
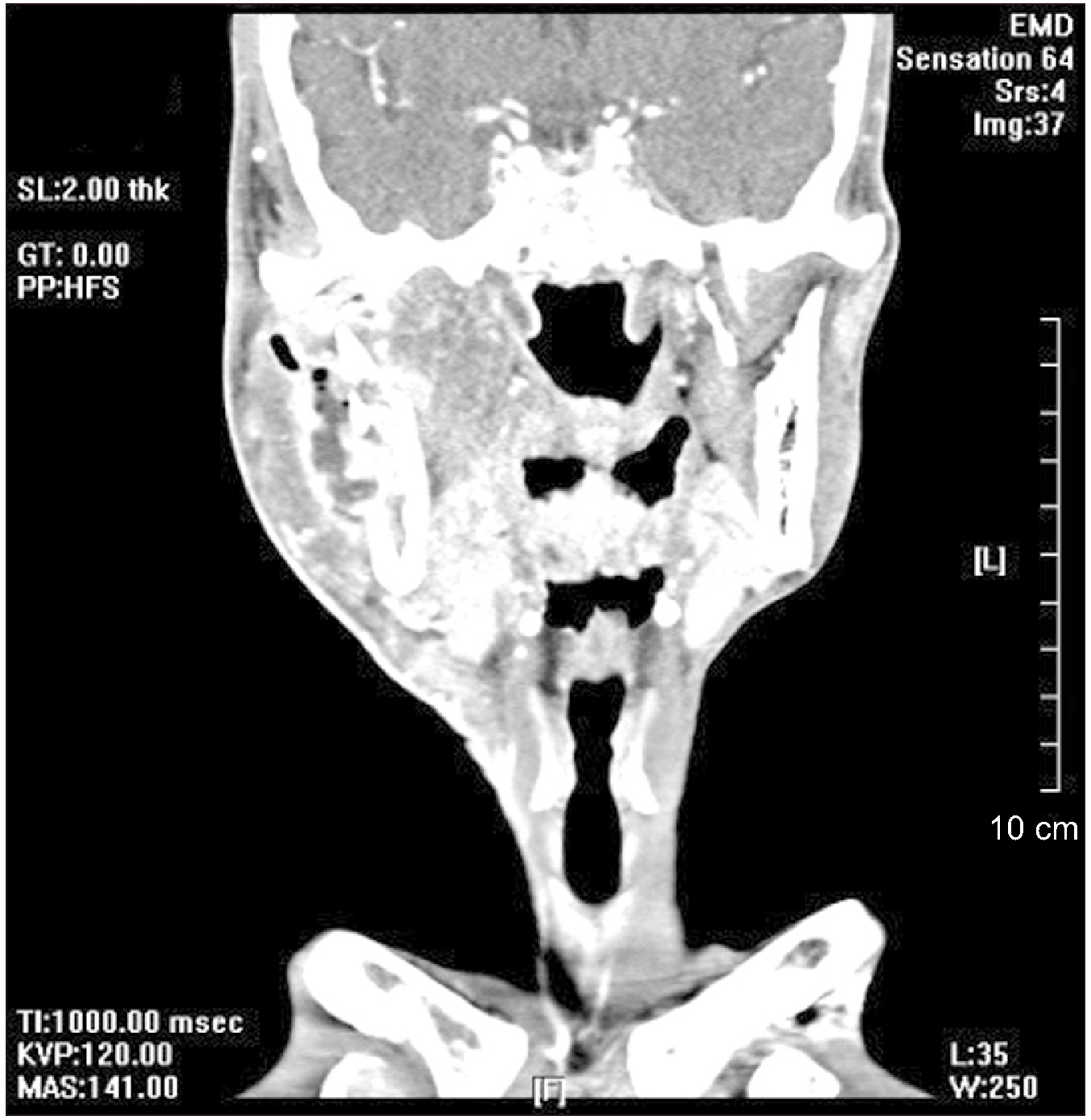
Fig. 5 On computed tomography, submasticatory space abscess and bony destruction were observed around the condyle and ramus.
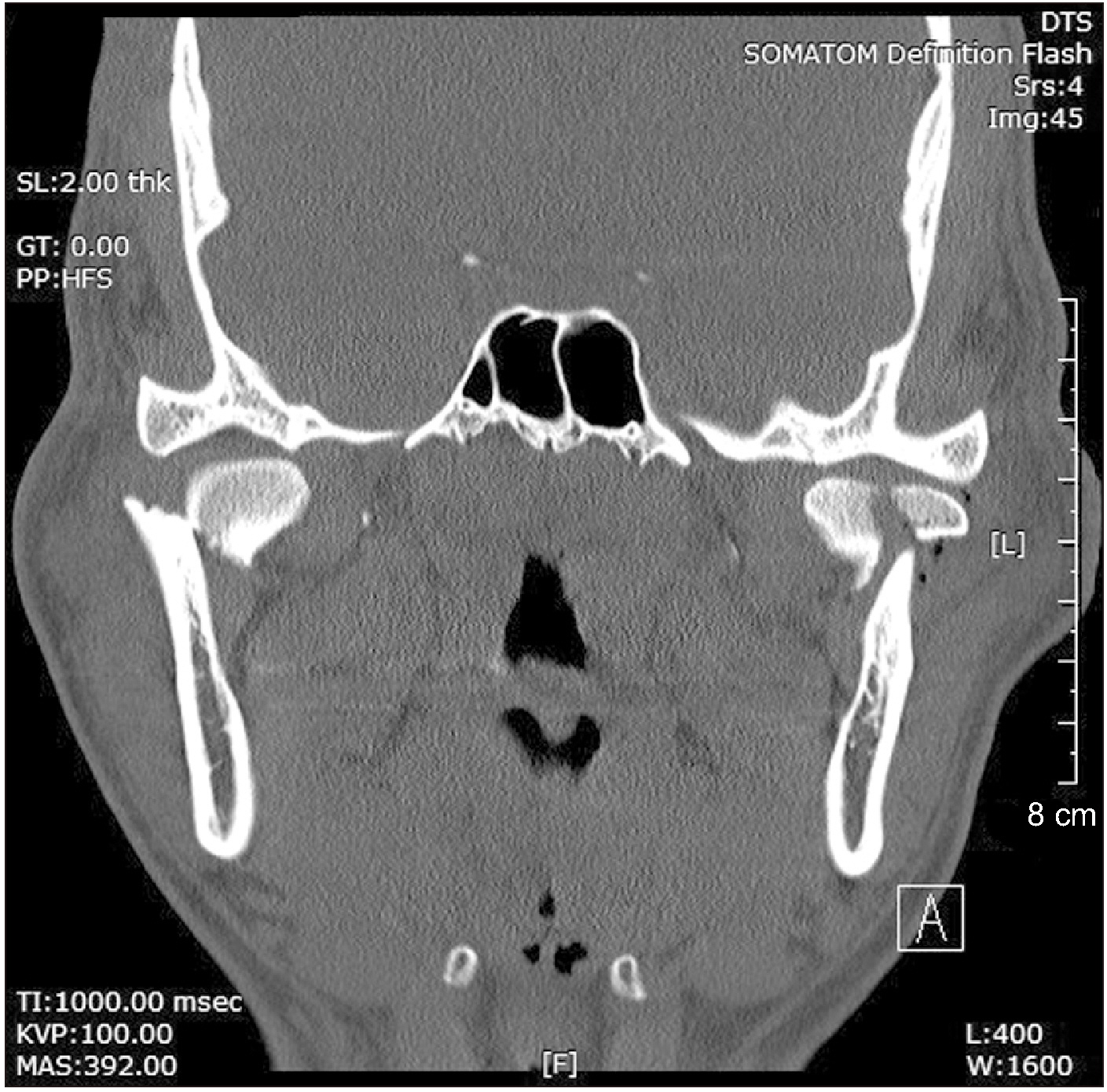
Fig. 6 On computed tomography, right and left condylar fractures were level 2, but there were multiple fragments on the left side.
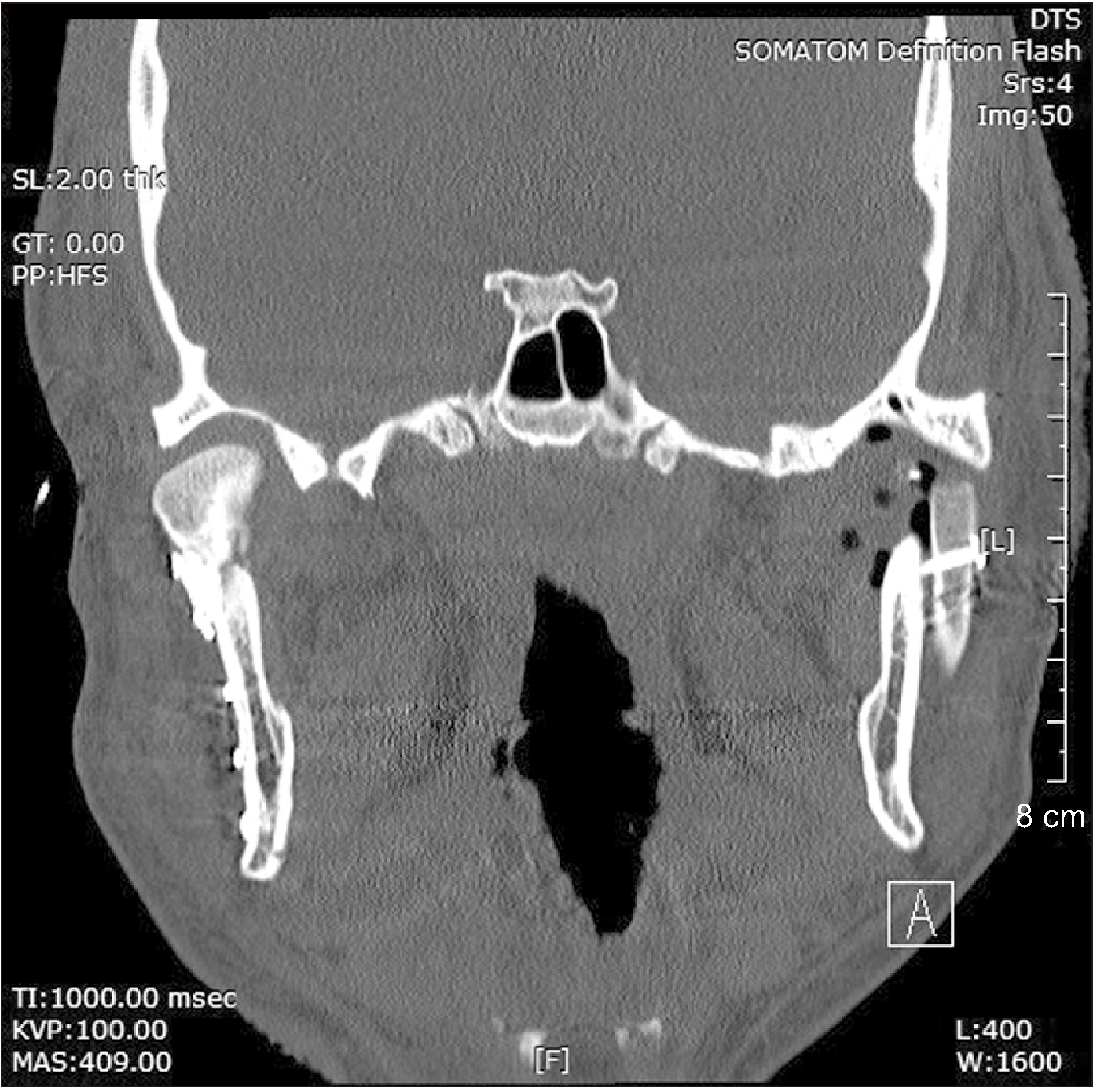
Fig. 7 The right condyle was fixed openly, and the left condyle was reconstructed with a costochondral graft. The cartilage portion of the graft was positioned well into the condylar fossa.
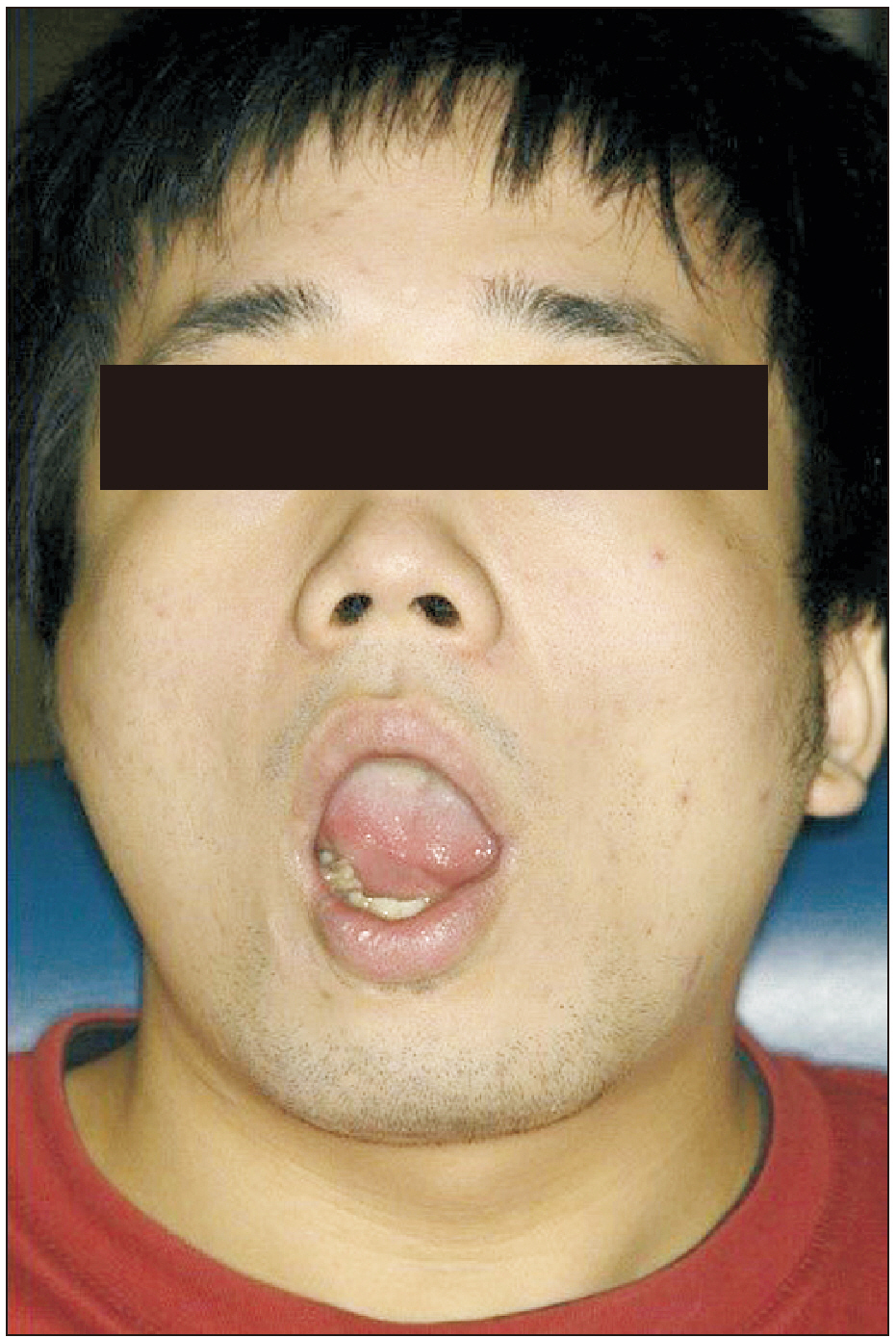
Fig. 8 Patient showed limited mandibular excursion, but maximum mouth opening was 45 mm in length.

Fig. 9 On computed tomography, submasticatory space abscess and bony destruction were observed around the condyle and ramus.
Reference
-
References
1. Saeed N, Hensher R, McLeod N, Kent J. 2002; Reconstruction of the temporomandibular joint autogenous compared with alloplastic. Br J Oral Maxillofac Surg. 40:296–9. https://doi.org/10.1016/s0266-4356(02)00139-0 . DOI: 10.1016/s0266-4356(02)00139-0. PMID: 12175828.
Article2. Khadka A, Hu J. 2012; Autogenous grafts for condylar reconstruction in treatment of TMJ ankylosis: current concepts and considerations for the future. Int J Oral Maxillofac Surg. 41:94–102. https://doi.org/10.1016/j.ijom.2011.10.018 . DOI: 10.1016/j.ijom.2011.10.018. PMID: 22088390.
Article3. Mohan MC, Prasad BR, Bhat S, Bhat SS. 2014; Reconstruction of condyle following surgical correction of temporomandibular joint ankylosis: current concepts and considerations for the future. NUJHS. 4:39–46.4. Quinn PD. 1998. Color atlas of temporomandibular joint surgery. Mosby;Louis:5. Bayat M, Badri A, Moharamnejad N. 2009; Treatment of temporomandibular joint ankylosis: gap and interpositional arthroplasty with temporalis muscle flap. Oral Maxillofac Surg. 13:207–12. https://doi.org/10.1007/s10006-009-0174-4 . DOI: 10.1007/s10006-009-0174-4. PMID: 19806372.
Article6. Jang HW, Kim NK, Lee WS, Kim HJ, Cha IH, Nam W. 2014; Mandibular condyle and infratemporal fossa reconstruction using vascularized costochondral and calvarial bone grafts. J Korean Assoc Oral Maxillofac Surg. 40:83–6. https://doi.org/10.5125/jkaoms.2014.40.2.83 . DOI: 10.5125/jkaoms.2014.40.2.83. PMID: 24868505. PMCID: PMC4028791.
Article7. Fernandes R, Fattahi T, Steinberg B. 2006; Costochondral rib grafts in mandibular reconstruction. Atlas Oral Maxillofac Surg Clin North Am. 14:179–83. https://doi.org/10.1016/j.cxom.2006.05.007 . DOI: 10.1016/j.cxom.2006.05.007. PMID: 16959605.
Article8. Chen CT, Lai JP, Chen YR. 1997; Costochondral graft in acute mandibular condylar fracture. Plast Reconstr Surg. 100:1234–9. https://doi.org/10.1097/00006534-199710000-00024 . DOI: 10.1097/00006534-199710000-00024. PMID: 9326785.
Article9. Mosby EL, Hiatt WR. 1989; A technique of fixation of costochondral grafts for reconstruction of the temporomandibular joint. J Oral Maxillofac Surg. 47:209–11. https://doi.org/10.1016/s0278-2391(89)80122-3 . DOI: 10.1016/s0278-2391(89)80122-3. PMID: 2913260.
Article10. Shetty KP, Mehta R, Mokal N. 2000; An innovative technique for fixing costochondral grafts. Plast Reconstr Surg. 106:1658–9. https://doi.org/10.1097/00006534-200012000-00048 . DOI: 10.1097/00006534-200012000-00048. PMID: 11129205.
Article11. Kaban LB, Troulis MJ. 2004. Pediatric oral and maxillofacial surgery. W.B. Saunders;Philadelphia: p. 351.12. Matukas VJ, Szymela VF, Schmidt JF. 1980; Surgical treatment of bony ankylosis in a child using a composite cartilage-bone iliac crest graft. J Oral Surg. 38:903–5. PMID: 7003077.13. Kummoona R. 1986; Chondro-osseous iliac crest graft for one stage reconstruction of the ankylosed TMJ in children. J Maxillofac Surg. 14:215–20. https://doi.org/10.1016/s0301-0503(86)80292-2 . DOI: 10.1016/s0301-0503(86)80292-2. PMID: 3525723.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- TEMPOROMANDIBULAR JOINT RECONSTRUCTION USING COSTOCHONDRAL GRAFT: CASE REPORTS
- Comparison of Costochondral Graft and Customized Total Joint Reconstruction for Treatments of Temporomandibular Joint Replacement
- Mandibular condyle and infratemporal fossa reconstruction using vascularized costochondral and calvarial bone grafts
- Autogenous auricular cartilage graft for repair of temporomandibular joint disk
- Immediate reconstruction using vertical ramus osteotomy and bone slidng after condylectomy due to osteochondroma: a case report
