Ruptured Pancreaticoduodenal Artery Aneurysm with Pancreatitis Treated Using Endovascular and Endoscopic Methods
- Affiliations
-
- 1Department of Surgery, Wonkwang University School of Medicine, Iksan, Korea
- KMID: 2515141
- DOI: http://doi.org/10.4166/kjg.2021.032
Abstract
- Pancreaticoduodenal artery aneurysm (PDAA) is a rare form of abdominal visceral aneurysm that accounts for approximately 2% of all cases. Most cases of PDAA are associated with celiac artery stenosis (CAS). Regardless of the size, there is a risk of rupture. Therefore, treatment should be performed immediately after discovery, even though the need to treat the accompanying CAS, if present, is controversial. The authors report a case of ruptured PDAA and accompanying pancreatitis treated using endovascular and endoscopic methods without treatment of CAS. A 50-year-old man was admitted to the emergency department of Wonkwang University Hospital with epigastric pain and hypovolemic shock. CT revealed a ruptured PDAA and a large volume hemoperitoneum. Emergency angiography was performed, and angioembolization of the PDAA was performed successfully. Follow-up CT revealed infection and pancreatitis, which were treated by surgical drainage and pancreatic duct stenting with ERCP. Because the degree of stenosis was not severe, it was decided to follow-up the accompanying CAS. After discharge, the patient was followed up without complications.
Figure
-
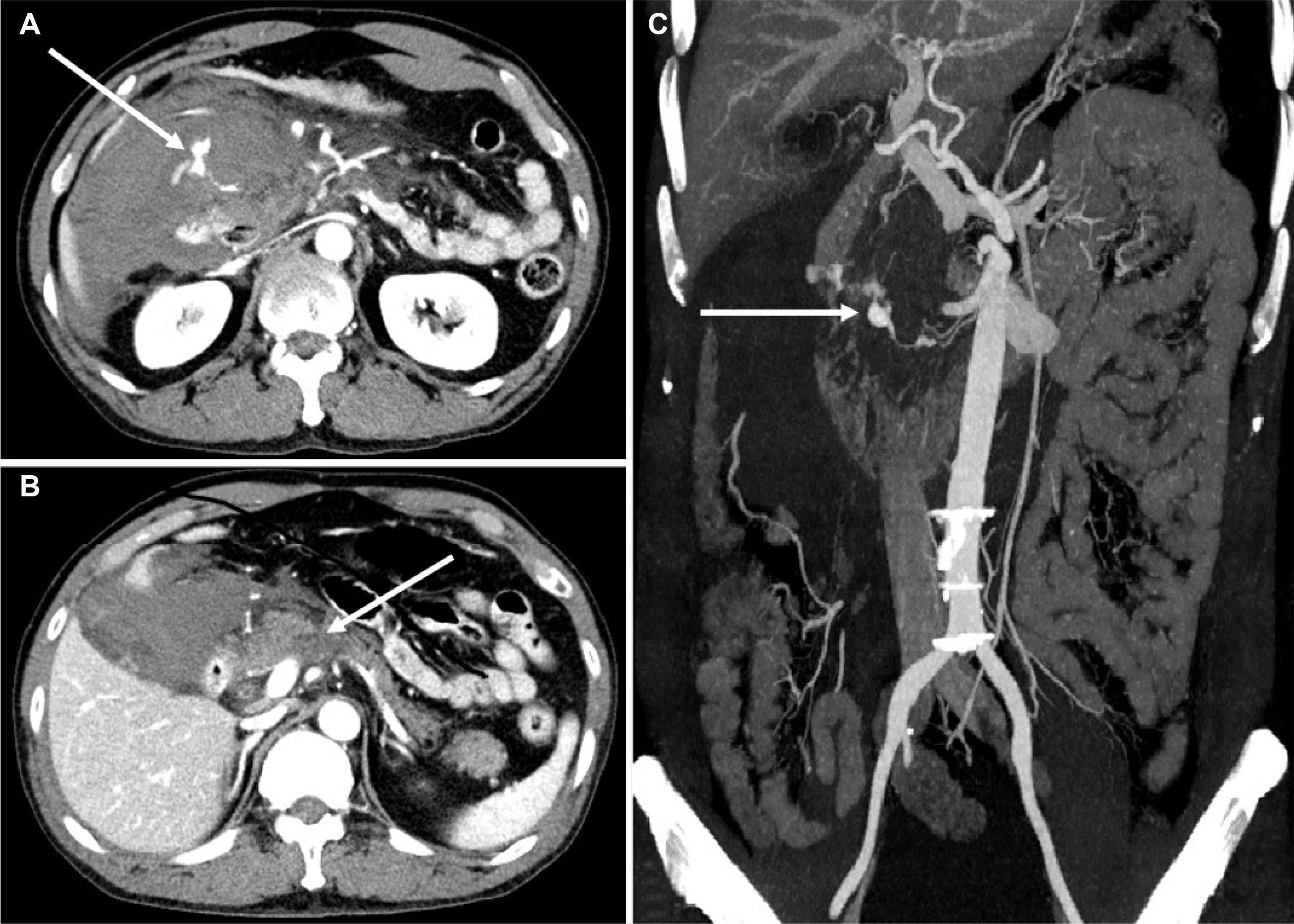
Fig. 1 Initial computed tomography (CT) performed in the emergency department. (A) Axial CT demonstrating contrast extravasation of the inferior pancreaticoduodenal artery (PDA) (arrow), which appears to be due to an aneurysmal sac, and large acute hematoma in the right anterior pararenal space and perihepatic space are shown. (B) CT revealing a mild hypodense lesion at the pancreas head, suggesting acute pancreatitis (arrow). (C) Maximum intensity projection image revealing aneurysmal dilatation of the inferior PDA (arrow).
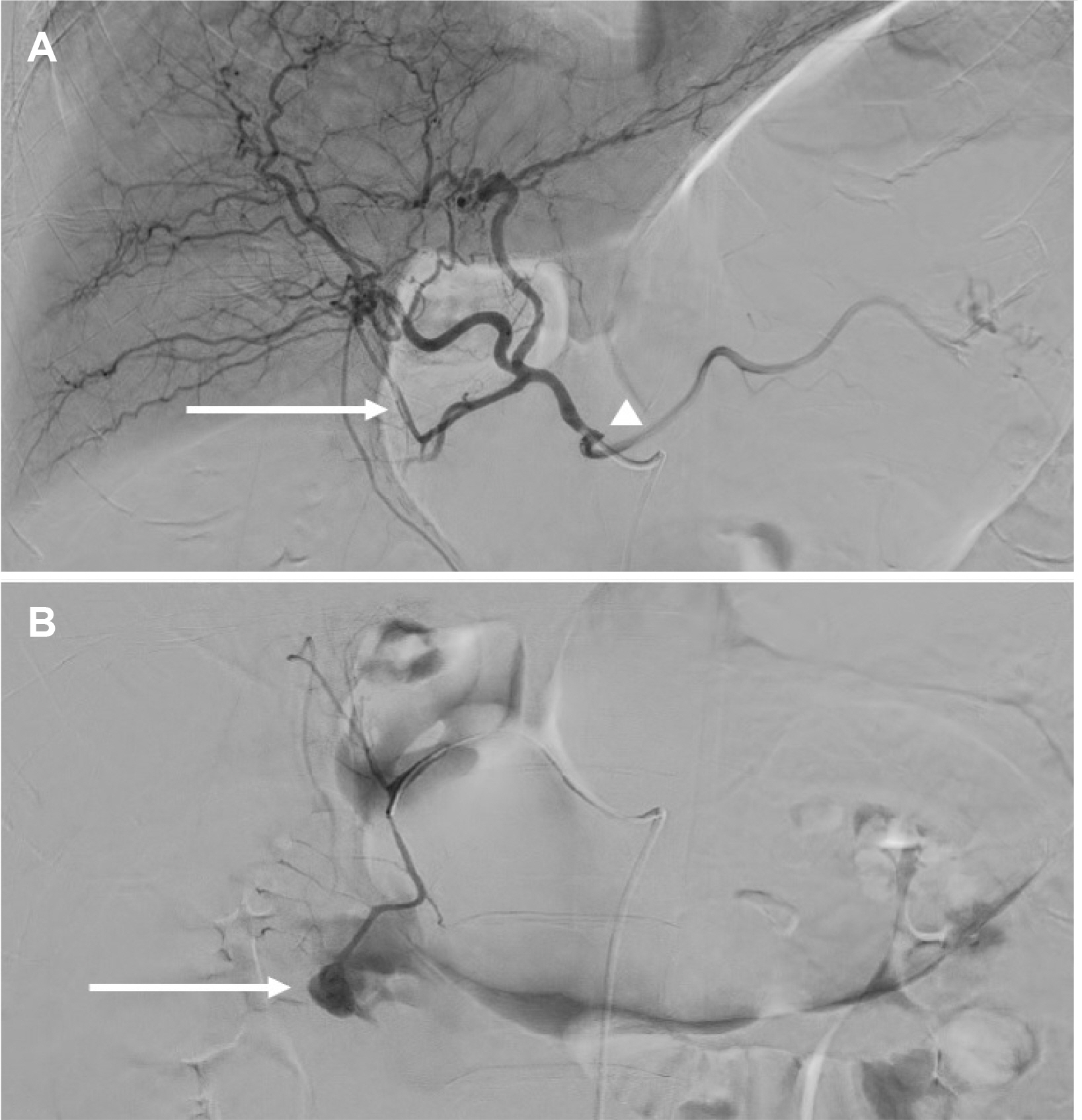
Fig. 2 Arteriography after initial resuscitation. (A) Celiac artery stenosis (CAS) (arrowhead) and hepatic arterial blood flow from the pancreaticoduodenal artery (PDA) are shown (arrow). (B) Large pseudoaneurysm and extravasation in the superior anterior PDA were detected (arrow).

Fig. 3 Vascular-aorta computed tomography angiography after 2 days of transarterial embolization. (A) Coronal image revealing slightly decreased size of hematoma in the anterior pararenal space. (B) Celiac artery stenosis is also apparent (arrow).

Fig. 4 Magnetic resonance imaging and endoscopic retrograde cholangiopancreatography (ERCP) performed to determine the etiology of the elevated serum amylase and lipase and treat pancreatitis (A) increased signal intensity in the T1-weighted image at the head of the pancreas (arrow). (B) ERCP with plastic stenting in the pancreatic duct was performed.
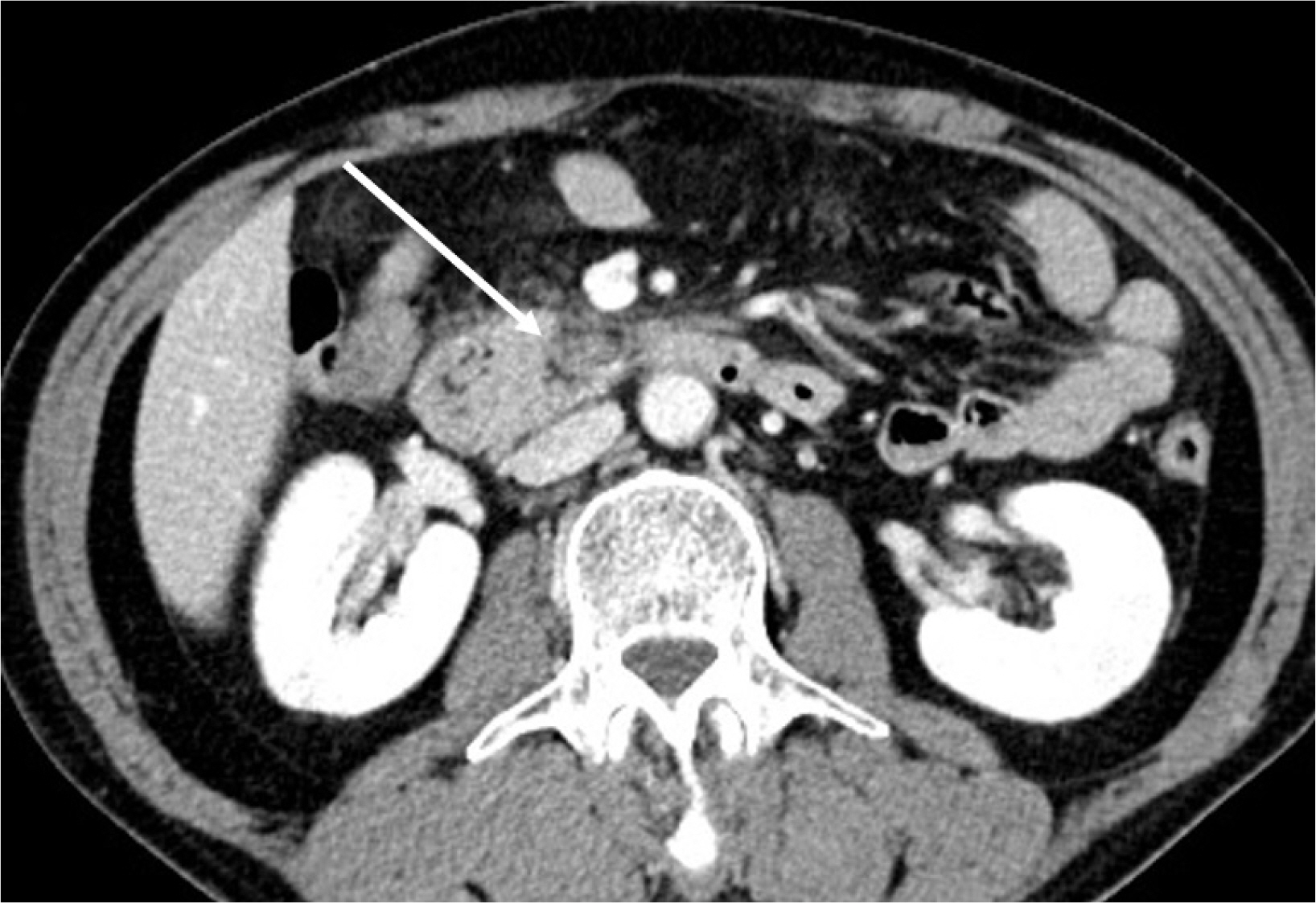
Fig. 5 Computed tomography performed 6 months after discharge. Marked decreased size of the previously noted mass-like lesion with mild haziness in the retromesenteric space, suggesting an improving state of organizing hematoma with adjacent fibrotic changes (arrow).
Reference
-
1. Stanley JC, Wakefield TW, Graham LM, Whitehouse WM Jr, Zelenock GB, Lindenauer SM. 1986; Clinical importance and management of splanchnic artery aneurysms. J Vasc Surg. 3:836–840. DOI: 10.1016/0741-5214(86)90059-5.
Article2. Corey MR, Ergul EA, Cambria RP, et al. 2016; The natural history of splanchnic artery aneurysms and outcomes after operative intervention. J Vasc Surg. 63:949–957. DOI: 10.1016/j.jvs.2015.10.066. PMID: 26792545.
Article3. de Perrot M, Berney T, Deléaval J, Bühler L, Mentha G, Morel P. 1999; Management of true aneurysms of the pancreaticoduodenal arteries. Ann Surg. 229:416–420. DOI: 10.1097/00000658-199903000-00016. PMID: 10077055. PMCID: PMC1191708.
Article4. Kalva SP, Athanasoulis CA, Greenfield AJ, et al. 2007; Inferior pancreaticoduodenal artery aneurysms in association with celiac axis stenosis or occlusion. Eur J Vasc Endovasc Surg. 33:670–675. DOI: 10.1016/j.ejvs.2006.12.021. PMID: 17276102.
Article5. Yoon HJ, Choi JS, Shin WY, Lee KY, Ahn SI. 2020; Causal relationship between celiac stenosis and pancreaticoduodenal artery aneurysm: interpretation by simulation using an electric circuit. Biomed Res Int. 2020:2738726. DOI: 10.1155/2020/2738726. PMID: 32596287. PMCID: PMC7298276.
Article6. Sakatani A, Doi Y, Kitayama T, et al. 2016; Pancreaticoduodenal artery aneurysm associated with coeliac artery occlusion from an aortic intramural hematoma. World J Gastroenterol. 22:4259–4263. DOI: 10.3748/wjg.v22.i16.4259. PMID: 27122676. PMCID: PMC4837443.
Article7. Coll DP, Ierardi R, Kerstein MD, Yost S, Wilson A, Matsumoto T. 1998; Aneurysms of the pancreaticoduodenal arteries: a change in management. Ann Vasc Surg. 12:286–291. DOI: 10.1007/s100169900155. PMID: 9588518.
Article8. Ricci G, Riu P, Attinà GM, et al. 2017; Endovascular treatment of ruptured pancreaticoduodenal artery aneurysm: the importance of collateral vessels. A case report. Int J Surg Case Rep. 41:205–208. DOI: 10.1016/j.ijscr.2017.10.036. PMID: 29096344. PMCID: PMC5686227.
Article9. Murata S, Tajima H, Fukunaga T, et al. 2006; Management of pancreaticoduodenal artery aneurysms: results of superselective transcatheter embolization. AJR Am J Roentgenol. 187:W290–W298. DOI: 10.2214/AJR.04.1726. PMID: 16928907.
Article10. Takeuchi Y, Morikage N, Samura M, et al. 2017; Treatment options for celiac stenosis and pancreaticoduodenal artery aneurysms. Ann Vasc Surg. 41:281.e21–281.e23. DOI: 10.1016/j.avsg.2016.10.036. PMID: 28238917.
Article11. Sgroi MD, Kabutey NK, Krishnam M, Fujitani RM. 2015; Pancreaticoduodenal artery aneurysms secondary to median arcuate ligament syndrome may not need celiac artery revascularization or ligament release. Ann Vasc Surg. 29:122.e1–122.e1227. DOI: 10.1016/j.avsg.2014.05.020. PMID: 24930977.
Article12. Sugae T, Fujii T, Kodera Y, et al. 2012; Classification of the celiac axis stenosis owing to median arcuate ligament compression, based on severity of the stenosis with subsequent proposals for management during pancreatoduodenectomy. Surgery. 151:543–549. DOI: 10.1016/j.surg.2011.08.012. PMID: 22001637.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anterior Superior Pancreaticoduodenal Artery Aneurysm Rupture Associated with Abdominal Pain
- Endovascular Coil Trapping of a Ruptured Dissecting Aneurysm of the Vertebral Artery Using Detachable Coils and Micro-Tornado(R) Coils
- Rupture of an Idiopathic Aneurysm of the Inferior Pancreaticoduodenal Artery Leading to an Intra-Abdominal Bleeding
- Endovascular Treatment of Multiple Pancreaticoduodenal Artery Aneurysms Associated with Celiac Artery Stenosis: A Case Report
- Retroperitoneal Hematoma Caused by Ruptured Pancreaticoduodenal Artery Aneurysm
