J Korean Neurosurg Soc.
2021 Mar;64(2):261-270. 10.3340/jkns.2020.0149.
Clinical Significance of Decompressive Craniectomy Surface Area and Side
- Affiliations
-
- 1Department of Neurosurgery, Bucheon St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- 2Department of Neurosurgery, Eunpyeong St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2513857
- DOI: http://doi.org/10.3340/jkns.2020.0149
Abstract
Objective
: Decompressive craniectomy (DC) can partially remove the unyielding skull vault and make affordable space for the expansion of swelling brain contents. The objective of this study was to compare clinical outcome according to DC surface area (DC area) and side.
Methods
: A total of 324 patients underwent different surgical methods (unilateral DC, 212 cases and bilateral DC, 112 cases) were included in this retrospective analysis. Their mean age was 53.4±16.6 years (median, 54 years). Neurological outcome (Glasgow outcome scale), ventricular intracranial pressure (ICP), and midline shift change (preoperative minus postoperative) were compared according to surgical methods and total DC area, DC surface removal rate (DC%) and side.
Results
: DC surgery was effective for ICP decrease (32.3±16.7 mmHg vs. 19.2±13.4 mmHg, p<0.001) and midline shift change (12.5±7.6 mm vs. 7.8±6.9 mm, p<0.001). The bilateral DC group showed larger total DC area (125.1±27.8 cm2 for unilateral vs. 198.2±43.0 cm2 for bilateral, p<0.001). Clinical outcomes were nonsignificant according to surgical side (favorable outcome, p=0.173 and mortality, p=0.470), significantly better when total DC area was over 160 cm2 and DC% was 46% (p=0.020 and p=0.037, respectively).
Conclusion
: DC surgery is effective in decrease the elevated ICP, decrease the midline shift and improve the clinical outcome in massive brain swelling patient. Total DC area and removal rate was larger in bilateral DC than unilateral DC but clinical outcome was not influenced by DC side. DC area more than 160 cm2 and DC surface removal rate more than 46% were more important than DC side.
Figure
-
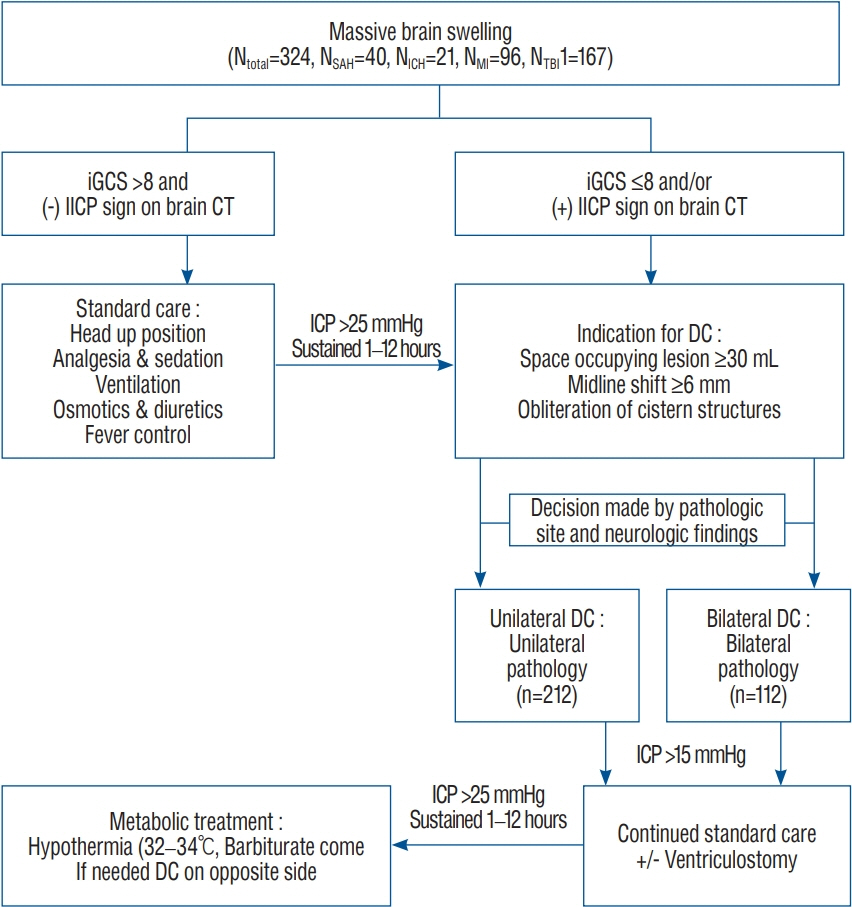
Fig. 1. Flow sheet of treatment protocol. SAH : subarachnoid hemorrhage, ICH : intracerebral hemorrhage, MI : major infarction, TBI : traumatic brain injury, iGCS : initial Glasgow coma scale, iICP : intracranial pressure after ventricular puncture, CT : computed tomography, DC : decompressive craniectomy.
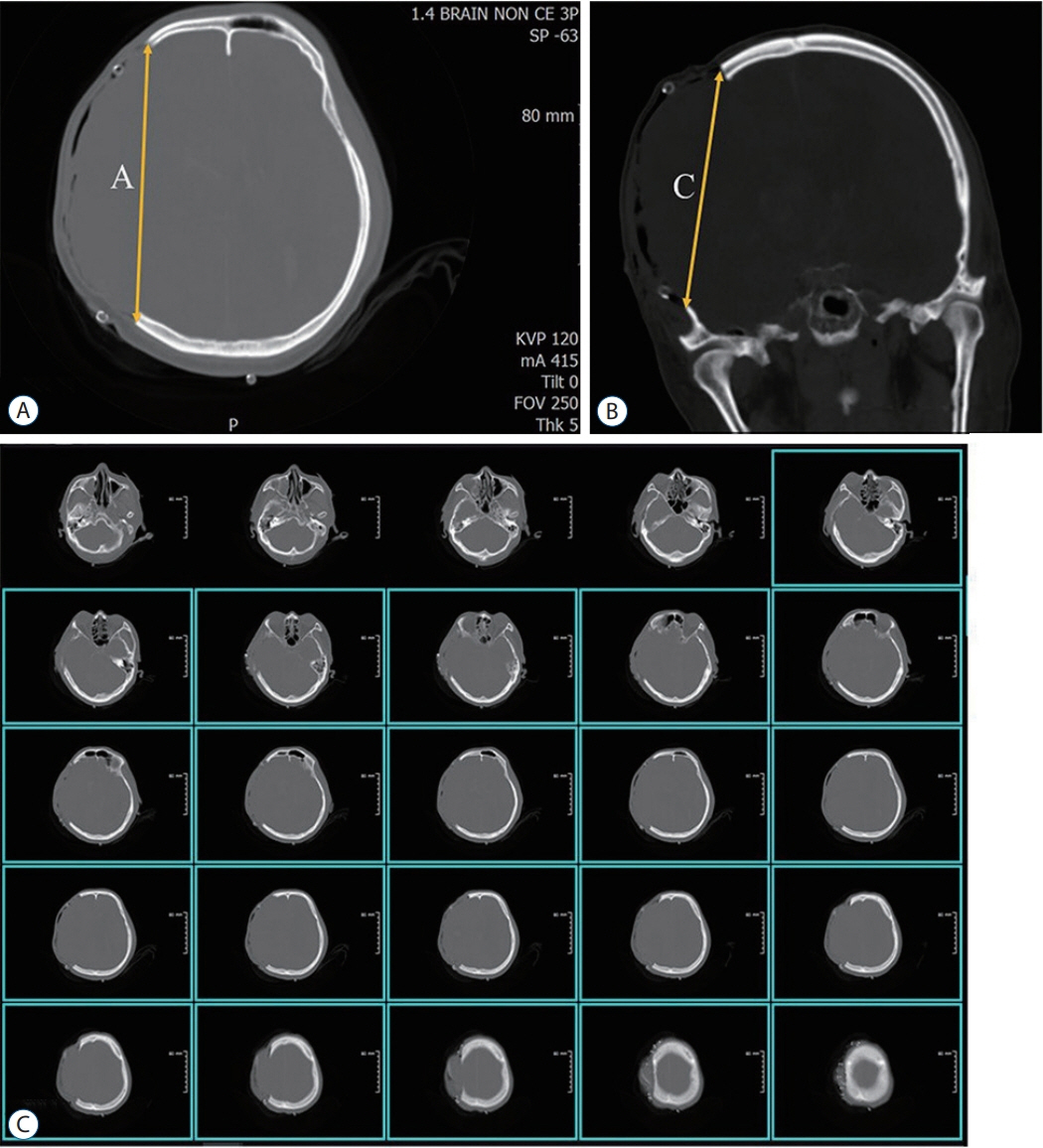
Fig. 2. The simple AC methods for calculating DC area. A : A was the longest length of craniectomy on the axial slices. B : C was the longest length of craniectomy on the coronal slice. C : C could be calculated the number of axial cuts (the number of blue box) by craniectomy and slice thickness (red box, 5 mm). DC : decompressive craniectomy.
Reference
-
References
1. Andrews PJ, Sinclair HL, Rodriguez A, Harris BA, Battison CG, Rhodes JK, et al. Hypothermia for intracranial hypertension after traumatic brain injury. N Engl J Med. 373:2403–2412. 2015.
Article2. Bor-Seng-Shu E, Figueiredo EG, Amorim RL, Teixeira MJ, Valbuza JS, de Oliveira MM, et al. Decompressive craniectomy: a meta-analysis of influences on intracranial pressure and cerebral perfusion pressure in the treatment of traumatic brain injury. J Neurosurg. 117:589–596. 2012.
Article3. Bor-Seng-Shu E, Figueiredo EG, Fonoff ET, Fujimoto Y, Panerai RB, Teixeira MJ. Decompressive craniectomy and head injury: brain morphometry, ICP, cerebral hemodynamics, cerebral microvascular reactivity, and neurochemistry. Neurosurg Rev. 36:361–370. 2013.
Article4. Bösel J, Zweckberger K, Hacke W. Haemorrhage and hemicraniectomy: refining surgery for stroke. Curr Opin Neurol. 28:16–22. 2015.5. Brain Trauma Foundation; American Association of Neurological Surgeons; Congress of Neurological Surgeons. Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 24 Suppl 1:S1–S106. 2007.6. Brain Trauma Foundation; American Association of Neurological Surgeons; Joint Section on Neurotrauma and Critical Care. Guidelines for the management of severe head injury. J Neurotrauma. 13:641–734. 1996.7. Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA, Hartl R, et al. Guidelines for the management of severe traumatic brain injury. VIII. Intracranial pressure thresholds. J Neurotrauma 24 Suppl. 1:S55–S58. 2007.8. Carney N, Totten AM, O'Reilly C, Ullman JS, Hawryluk GW, Bell MJ, et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery. 80:6–15. 2017.
Article9. Clifton GL, Allen S, Barrodale P, Plenger P, Berry J, Koch S, et al. A phase II study of moderate hypothermia in severe brain injury. J Neurotrauma. 10:263–271. discussion 273. 1993.
Article10. Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D'Urso P, et al. Decompressive craniectomy in diffuse traumatic brain injury. N Engl J Med. 364:1493–1502. 2011.
Article11. El Ahmadieh TY, Adel JG, El Tecle NE, Daou MR, Aoun SG, Nanney AD 3rd, et al. Surgical treatment of elevated intracranial pressure: decompressive craniectomy and intracranial pressure monitoring. Neurosurg Clin N Am. 24:375–391. 2013.12. Ferro JM, Crassard I, Coutinho JM, Canhão P, Barinagarrementeria F, Cucchiara B, et al. Decompressive surgery in cerebrovenous thrombosis: a multicenter registry and a systematic review of individual patient data. Stroke. 42:2825–2831. 2011.13. Frank JI, Schumm LP, Wroblewski K, Chyatte D, Rosengart AJ, Kordeck C, et al. Hemicraniectomy and durotomy upon deterioration from infarction-related swelling trial: randomized pilot clinical trial. Stroke. 45:781–787. 2014.
Article14. Gerber LM, Chiu YL, Carney N, Härtl R, Ghajar J. Marked reduction in mortality in patients with severe traumatic brain injury. J Neurosurg. 119:1583–1590. 2013.
Article15. Güresir E, Schuss P, Seifert V, Vatter H. Decompressive craniectomy in children: single-center series and systematic review. Neurosurgery. 70:881–888. discussion 888-889. 2012.16. Ho MY, Tseng WL, Xiao F. Estimation of the craniectomy surface area by using postoperative images. Int J Biomed Imaging. 2018:5237693. 2018.
Article17. Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB, et al. Surgical decompression for space-occupying cerebral infarction (the hemicraniectomy after middle cerebral artery infarction with life-threatening edema trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 8:326–333. 2009.
Article18. Honeybul S, Ho KM. The current role of decompressive craniectomy in the management of neurological emergencies. Brain Inj. 27:979–991. 2013.
Article19. Hutchinson PJ, Kolias AG, Timofeev IS, Corteen EA, Czosnyka M, Timothy J, et al. Trial of decompressive craniectomy for traumatic intracranial hypertension. N Engl J Med. 375:1119–1130. 2016.
Article20. Jiang JY, Xu W, Li WP, Xu WH, Zhang J, Bao YH, et al. Efficacy of standard trauma craniectomy for refractory intracranial hypertension with severe traumatic brain injury: a multicenter, prospective, randomized controlled study. J Neurotrauma. 22:623–628. 2005.
Article21. Jüttler E, Schwab S, Schmiedek P, Unterberg A, Hennerici M, Woitzik J, et al. Decompressive surgery for the treatment of malignant infarction of the middle cerebral artery (DESTINY): a randomized, controlled trial. Stroke. 38:2518–2525. 2007.
Article22. Kakar V, Nagaria J, John Kirkpatrick P. The current status of decompressive craniectomy. Br J Neurosurg. 23:147–157. 2009.
Article23. Kenning TJ, Gooch MR, Gandhi RH, Shaikh MP, Boulos AS, German JW. Cranial decompression for the treatment of malignant intracranial hypertension after ischemic cerebral infarction: decompressive craniectomy and hinge craniotomy. J Neurosurg. 116:1289–1298. 2012.
Article24. Kim KT, Park JK, Kang SG, Cho KS, Yoo DS, Jang DK, et al. Comparison of the effect of decompressive craniectomy on different neurosurgical diseases. Acta Neurochir (Wien). 151:21–30. 2009.
Article25. Lang SS, Kofke WA, Stiefel MF. Monitoring and intraoperative management of elevated intracranial pressure and decompressive craniectomy. Anesthesiol Clin. 30:289–310. 2012.
Article26. Lazaridis C, Czosnyka M. Cerebral blood flow, brain tissue oxygen, and metabolic effects of decompressive craniectomy. Neurocrit Care. 16:478–484. 2012.
Article27. Lazaridis C, DeSantis SM, Vandergrift AW, Krishna V. Cerebral blood flow velocity changes and the value of the pulsatility index post decompressive craniectomy. J Clin Neurosci. 19:1052–1054. 2012.
Article28. Marshall LF, Smith RW, Shapiro HM. The outcome with aggressive treatment in severe head injuries. Part I: the significance of intracranial pressure monitoring. J Neurosurg. 50:20–25. 1979.29. Missori P, Morselli C, Domenicucci M, Paolini S, Peschillo S, Scapeccia M, et al. Measurement of bone flap surface area and midline shift to predict overall survival after decompressive craniectomy. World Neurosurg. 96:11–14. 2016.
Article30. Morgalla MH, Will BE, Roser F, Tatagiba M. Do long-term results justify decompressive craniectomy after severe traumatic brain injury? J Neurosurg. 109:685–690. 2008.
Article31. Neugebauer H, Fiss I, Pinczolits A, Hecht N, Witsch J, Dengler NF, et al. Large size hemicraniectomy reduces early herniation in malignant middle cerebral artery infarction. Cerebrovasc Dis. 41:283–290. 2016.
Article32. Rahme R, Zuccarello M, Kleindorfer D, Adeoye OM, Ringer AJ. Decompressive hemicraniectomy for malignant middle cerebral artery territory infarction: is life worth living? J Neurosurg. 117:749–754. 2012.
Article33. Rosenfeld JV, Maas AI, Bragge P, Morganti-Kossmann MC, Manley GT, Gruen RL. Early management of severe traumatic brain injury. Lancet. 380:1088–1098. 2012.
Article34. Saul TG, Ducker TB. Effect of intracranial pressure monitoring and aggressive treatment on mortality in severe head injury. J Neurosurg. 56:498–503. 1982.
Article35. Schirmer CM, Hoit DA, Malek AM. Decompressive hemicraniectomy for the treatment of intractable intracranial hypertension after aneurysmal subarachnoid hemorrhage. Stroke. 38:987–992. 2007.
Article36. The Brain Trauma Foundation; The American Association of Neurological Surgeons; The Joint Section on Neurotrauma and Critical Care. Intracranial pressure treatment threshold. J Neurotrauma. 17:493–495. 2000.37. Ucar T, Akyuz M, Kazan S, Tuncer R. Role of decompressive surgery in the management of severe head injuries: prognostic factors and patient selection. J Neurotrauma. 22:1311–1318. 2005.
Article38. Vahedi K, Vicaut E, Mateo J, Kurtz A, Orabi M, Guichard JP, et al. Sequential-design, multicenter, randomized, controlled trial of early decompressive craniectomy in malignant middle cerebral artery infarction (DECIMAL trial). Stroke. 38:2506–2517. 2007.
Article39. Won YD, Yoo DS, Kim KT, Kang SG, Lee SB, Kim DS, et al. Cranioplasty effect on the cerebral hemodynamics and cardiac function. Acta Neurochir Suppl. 102:15–20. 2008.
Article40. Xiao B, Wu FF, Zhang H, Ma YB. A randomized study of urgent computed tomography-based hematoma puncture and aspiration in the emergency department and subsequent evacuation using craniectomy versus craniectomy only. J Neurosurg. 117:566–573. 2012.
Article41. Yoo DS, Kim DS, Cho KS, Huh PW, Park CK, Kang JK. Ventricular pressure monitoring during bilateral decompression with dural expansion. J Neurosurg. 91:953–959. 1999.
Article42. Zhao J, Su YY, Zhang Y, Zhang YZ, Zhao R, Wang L, et al. Decompressive hemicraniectomy in malignant middle cerebral artery infarct: a randomized controlled trial enrolling patients up to 80 years old. Neurocrit Care. 17:161–171. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Significance of Bifrontotemporal Decompressive Craniectomy in the Treatment of Severe Refractory Posttraumatic Brain Swelling
- Paradoxical Herniation after Decompressive Craniectomy for Acute Subdural Hematoma
- Decompressive Craniectomy in Traumatic Brain Injury: A Review Article
- Paradoxical Transtentorial Herniation Caused by Lumbar Puncture after Decompressive Craniectomy
- Does the Size of Unilateral Decompressive Craniectomy Impact Clinical Outcomes in Patients with Intracranial Mass Effect after Severe Traumatic Brain Injury?
