Lessons Learned from a Fulminant Case of Reversible Cerebral Vasoconstriction Syndrome: Past Medical History Misleads the Diagnosis and Intra-Arterial Milrinone Offers Diagnostic Utility
- Affiliations
-
- 1Department of Neurology, Rajagiri Hospital, Kochi, India
- 2Department of Neurology, Rabindranath International Institute of Cardiac Sciences, Kolkata, India
- KMID: 2513348
- DOI: http://doi.org/10.5469/neuroint.2020.00416
Abstract
- A 34-year-old post-partum female having dermatomyositis developed headache and became comatose after a seizure episode. Magnetic resonance imaging of brain showed a massive left ganglio-capsular bleed for which decompressive surgery was done. Computed tomographic angiography showed multiple foci of narrowing and irregularities in distal cerebral vessels. In view of dermatomyositis, the diagnosis of vasculitis was considered and pulse therapy of intravenous methylprednisolone was started. The patient, however, showed no improvement and developed new brain infarcts. She was subsequently taken up for a diagnostic cerebral angiography which showed multifocal severe narrowing in bilateral major cerebral arteries. These angiographic abnormalities showed excellent reversibility to intra-arterial milrinone and hence, reversible cerebral vasoconstriction syndrome (RCVS) was diagnosed. Normal angiographic findings in the first week do not rule out the disease and a repeat angiography should be considered if the clinical suspicion of the RCVS is high. Intra-arterial milrinone has a high diagnostic utility.
Keyword
Figure
-
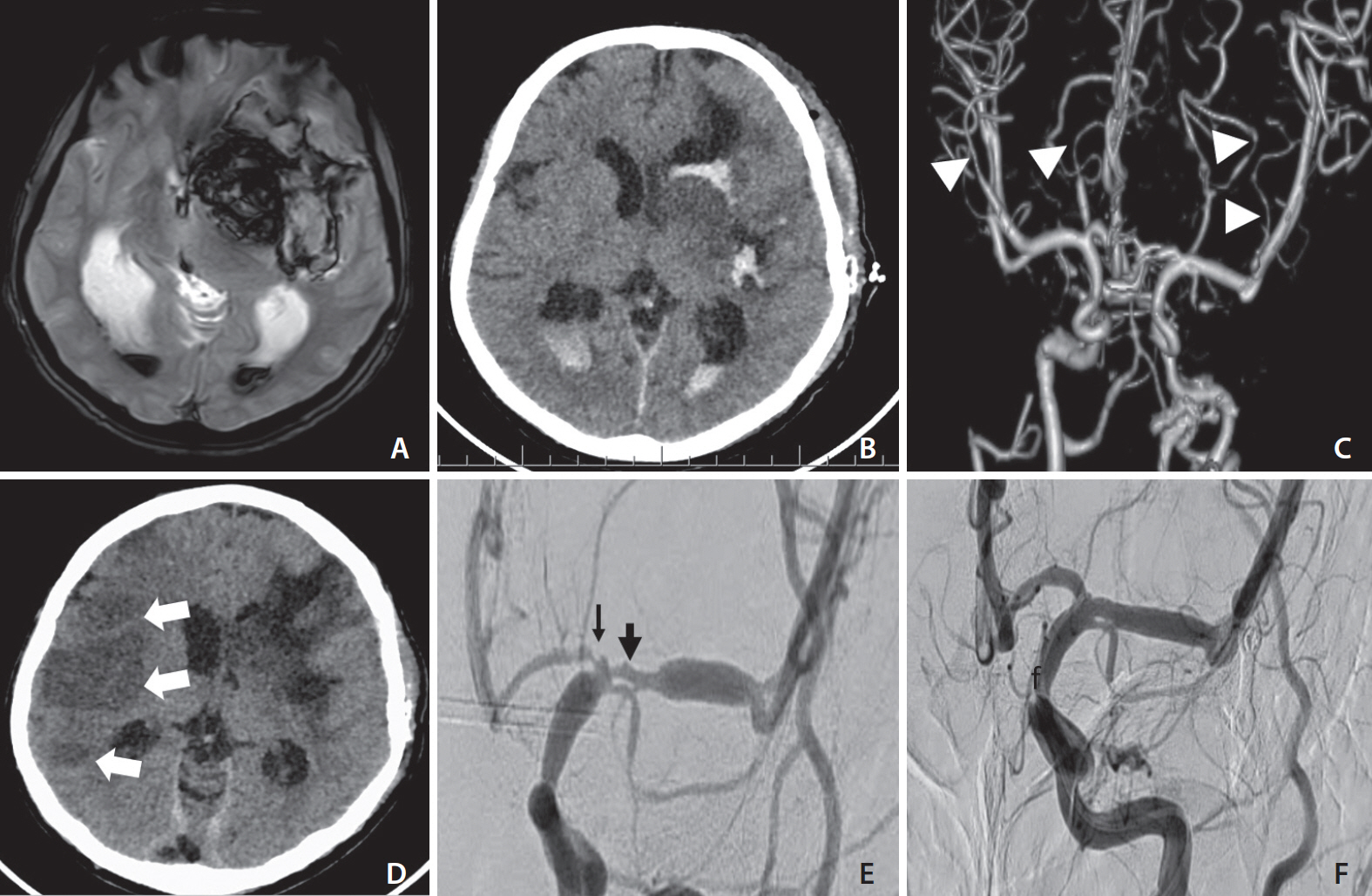
Fig. 1. (A) Magnetic resonance imaging of brain showing large intra-parenchymal hematoma involving left ganglio-capsular and frontotemporal regions with significant midline shift. (B) Post-operative computed tomography (CT) scan of brain showing hematoma evacuation. (C) CT angiography demonstrating multifocal luminal irregularities and narrowing (white arrowheads) of distal branches of bilateral middle and posterior cerebral arteries. (D) CT brain on twelfth postoperative day showing multiple acute infarcts (white arrows) in right middle cerebral arteries (MCA) territory. (E) Digital subtraction angiography performed in the second week showing severe proximal narrowing of left MCA (black thick arrow) and the anterior cerebral arteries (ACA) (black thin arrow). (F) Post intra-arterial milrinone injection of left internal carotid artery showing excellent reversibility of MCA and ACA abnormalities.
Reference
-
1. Rocha EA, Topcuoglu MA, Silva GS, Singhal AB. RCVS2 score and diagnostic approach for reversible cerebral vasoconstriction syndrome. Neurology. 2019; 92:e639–e647.
Article2. Saini M, Jeerakathil T, Butcher K. Reversible cerebral vasoconstriction syndrome. Neurol India. 2009; 57:63–65.
Article3. Ducros A. Reversible cerebral vasoconstriction syndrome. Lancet Neurol. 2012; 11:906–917.
Article4. Valencia-Mendoza M, Ramírez-Rodríguez N, Vargas-Avila N, Peña-Ortiz A, Corzo-Villamizar M, Serna-Ramírez L, et al. Fatal reversible cerebral vasoconstriction syndrome: a systematic review of case series and case reports. J Clin Neurosci. 2019; 70:183–188.
Article5. Salvarani C, Brown RD Jr, Calamia KT, Christianson TJ, Huston J 3rd, Meschia JF, et al. Primary central nervous system vasculitis presenting with intracranial hemorrhage. Arthritis Rheum. 2011; 63:3598–3606.
Article6. Singhal AB, Hajj-Ali RA, Topcuoglu MA, Fok J, Bena J, Yang D, et al. Reversible cerebral vasoconstriction syndromes: analysis of 139 cases. Arch Neurol. 2011; 68:1005–1012.7. Singhal AB, Topcuoglu MA. Glucocorticoid-associated worsening in reversible cerebral vasoconstriction syndrome. Neurology. 2017; 88:228–236.
Article8. Xing B, Lenck S, Krings T, Hengwei J, Jaigobin CS, Schaafsma JD. Angiographic characteristics of hemorrhagic and ischemic phases of reversible cerebral vasoconstriction syndrome. Clin Neuroradiol. 2020; 30:85–89.
Article9. Ducros A, Fiedler U, Porcher R, Boukobza M, Stapf C, Bousser MG. Hemorrhagic manifestations of reversible cerebral vasoconstriction syndrome: frequency, features, and risk factors. Stroke. 2010; 41:2505–2511.10. Mrozek S, Lonjaret L, Jaffre A, Januel AC, Raposo N, Boetto S, et al. Reversible cerebral vasoconstriction syndrome with intracranial hypertension: should decompressive craniectomy be considered? Case Rep Neurol. 2017; 9:6–11.
Article11. Bouchard M, Verreault S, Gariépy JL, Dupré N. Intra-arterial milrinone for reversible cerebral vasoconstriction syndrome. Headache. 2009; 49:142–145.
Article12. Nowak DA, Rodiek SO, Henneken S, Zinner J, Schreiner R, Fuchs HH, et al. Reversible segmental cerebral vasoconstriction (Call-Fleming syndrome): are calcium channel inhibitors a potential treatment option? Cephalalgia. 2003; 23:218–222.
Article13. Mijalski C, Dakay K, Miller-Patterson C, Saad A, Silver B, Khan M. Magnesium for treatment of reversible cerebral vasoconstriction syndrome: case series. Neurohospitalist. 2016; 6:111–113.14. Linn J, Fesl G, Ottomeyer C, Straube A, Dichgans M, Bruckmann H, et al. Intra-arterial application of nimodipine in reversible cerebral vasoconstriction syndrome: a diagnostic tool in select cases? Cephalalgia. 2011; 31:1074–1081.
Article15. Ducros A, Boukobza M, Porcher R, Sarov M, Valade D, Bousser MG. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain. 2007; 130(Pt 12):3091–3101.
Article16. Chen SP, Fuh JL, Chang FC, Lirng JF, Shia BC, Wang SJ. Transcranial color doppler study for reversible cerebral vasoconstriction syndromes. Ann Neurol. 2008; 63:751–757.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reversible Cerebral Vasoconstriction Syndrome in a Professional Rugby Player: A Case Report
- Hemorrhagic Reversible Cerebral Vasoconstriction Syndrome: Clinical Presentation, Differential Diagnosis, Mechanism, and Treatment
- Dynamic Arterial Change of Cerebral Vasoconstriction in Reversible Cerebral Vasoconstriction Syndrome
- Reversible Cerebral Vasoconstriction Syndrome Combined with Posterior Encephalopathy Syndrome, and Transient Splenial Lesion after Delivery
- Bilateral Anterior Cerebral Artery Infarction Associated with Reversible Cerebral Vasoconstriction Syndrome
