Pneumothorax and pulmonary air leaks as ventilator-induced injuries in COVID-19
- Affiliations
-
- 1Intensive Care Unit U.O.C. Anestesia e Rianimazione, Department of Surgery, University Hospital of Padua, Padua, Italy
- KMID: 2513258
- DOI: http://doi.org/10.4266/acc.2020.00955
Figure
-
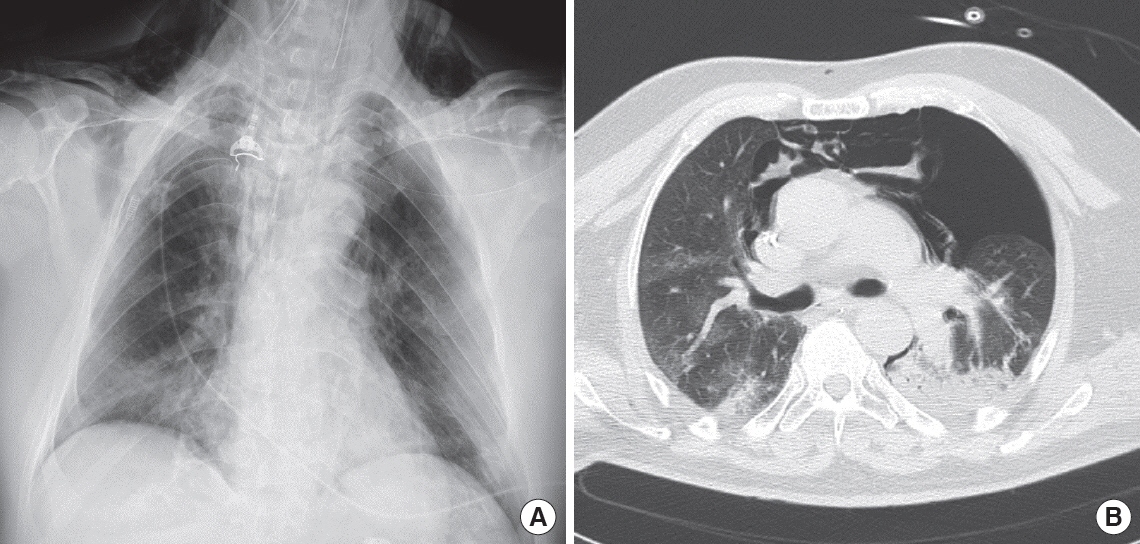
Figure 1. Chest X-ray (A) and computed tomography thoracic scan (B) of a 59-year-old male coronavirus disease 2019 (COVID-19) patient after 3 days of invasive ventilation. Ventilation occurred in pressure-control mode with the following parameters: peak inspiratory pressure, 27 cm H2O; positive end-expiratory pressure, 12 cm H2O; fraction of inspired oxygen, 0.6; inspiratory to expiratory ratio, 1:2; and respiratory rate, 16. The last measurement prior to the occurrence of pneumothorax was a plateau pressure of 25 cm H2O and static compliance of 43 L/cm H2O. Bilateral inhomogeneous parenchyma and consolidative aspects of the left lung were noted. The patient developed left pneumothorax and pneumomediastinum. On chest X-ray, subcutaneous emphysema is evident.
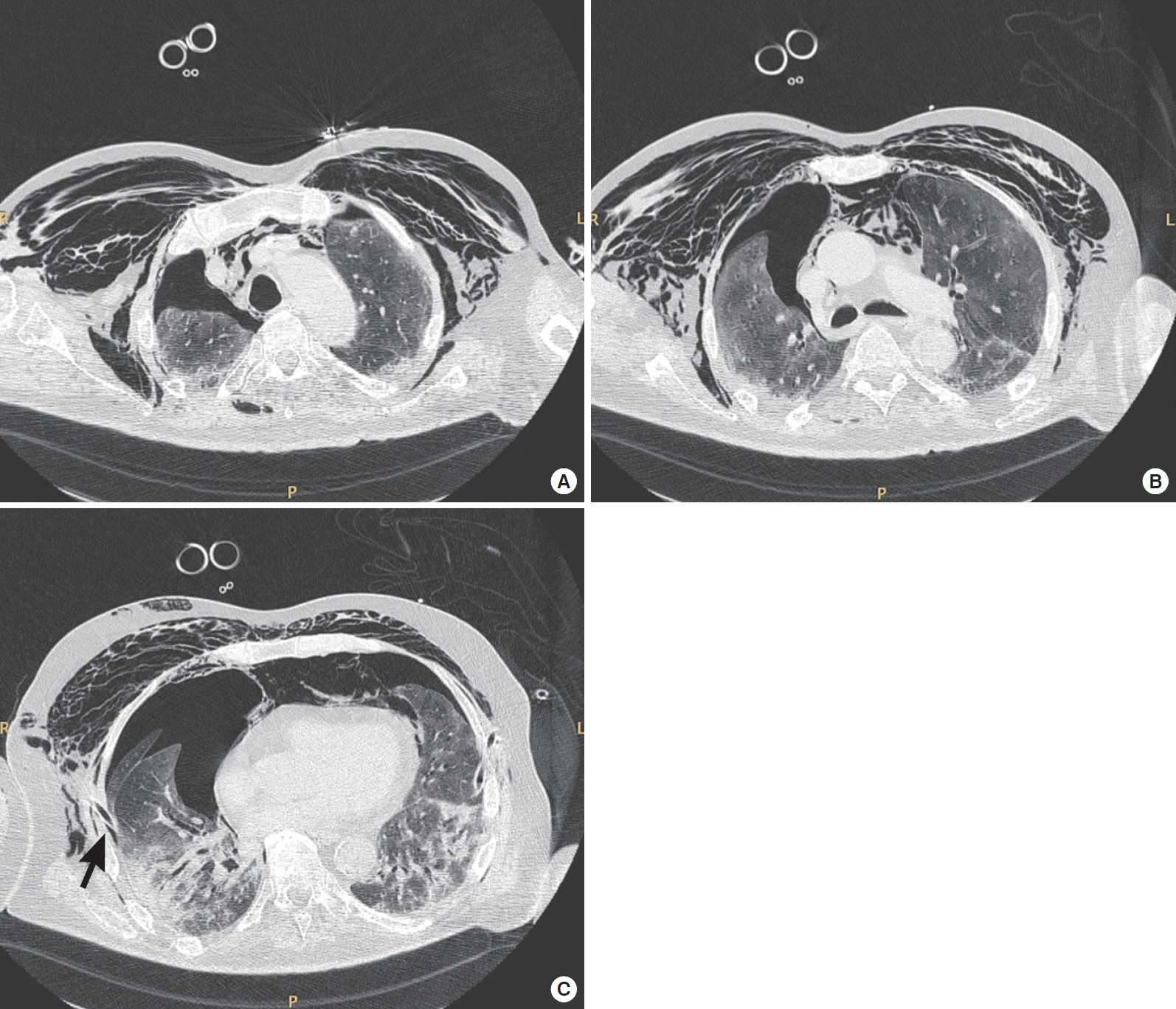
Figure 2. Thoracic computed tomography axial scans of a 75-year-old coronavirus disease 2019 (COVID-19) patient with moderate acute respiratory distress syndrome. The scans were obtained at (A) upper, (B) middle, and (C) lower thoracic level. The patient was receiving pressure support ventilation (pressure support, 14 cm H2O; positive end-expiratory pressure, 10 cm H2O; fraction of inspired oxygen, 0.75; and mean respiratory rate, 18). These scans revealed a failure of lung re-expansion after right thoracic drainage (black arrow) and persistence of pneumothorax, pneumomediastinum, and subcutaneous emphysema.
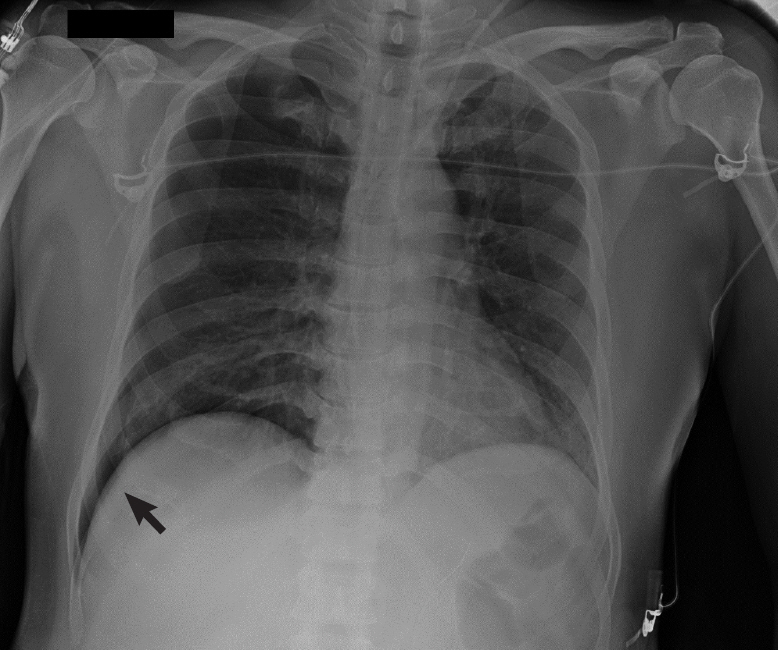
Figure 3. Chest X-ray of a 40-year-old male coronavirus disease 2019 (COVID-19) patient. Right pneumothorax of 30 mm. “Deep sulcus sign” was noted (black arrow). This patient developed pneumothorax after a cycle of non-invasive ventilation with a helmet interface. Ventilation was set at pressure support, 8 cm H2O; positive end-expiratory pressure, 10 cm H2O; and fraction of inspired oxygen, 0.55.
Reference
-
1. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020; 395:507–13.
Article2. Benson JC, Carlson ML, Lane JI. MRI of the internal auditory canal, labyrinth, and middle ear: how we do it. Radiology. 2020; 297:252–65.
Article3. Bradley BT, Maioli H, Johnston R, Chaudhry I, Fink SL, Xu H, et al. Histopathology and ultrastructural findings of fatal COVID-19 infections in Washington State: a case series. Lancet. 2020; 396:320–32.
Article4. Mead J, Takishima T, Leith D. Stress distribution in lungs: a model of pulmonary elasticity. J Appl Physiol. 1970; 28:596–608.
Article5. Cruces P, Retamal J, Hurtado DE, Erranz B, Iturrieta P, González C, et al. A physiological approach to understand the role of respiratory effort in the progression of lung injury in SARS-CoV-2 infection. Crit Care. 2020; 24:494.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Obstruction of Ventilator Exhalational Valve due to High Moisture Content in compressed Air - A case report
- Pneumomediastinum, Pneumoperitoneum and Subcutaneous Emphysema without Pneumothorax during Endotrocheal Ventilator Anesthesis
- Treatment of Prolonged Air-leak after Bilobectomy by Artificial Pneumoperitoneum
- Effect of High Frequency Ventilation on Tension Pneumothorax Induced by Conventional Ventilator
- COVID-19 Vaccination for Pilots and Air Traffic Controllers
