Ann Hepatobiliary Pancreat Surg.
2021 Feb;25(1):139-144. 10.14701/ahbps.2021.25.1.139.
Bouveret syndrome: A series of cases that illustrates a rare complication of chronic cholelithiasis
- Affiliations
-
- 1Departments of General Surgery, The Jewish Hospital of Cincinnati, Cincinnati, OH, USA
- 2Departments of Radiology, The Jewish Hospital of Cincinnati, Cincinnati, OH, USA
- KMID: 2513188
- DOI: http://doi.org/10.14701/ahbps.2021.25.1.139
Abstract
- Bouveret syndrome is defined as gastric outlet obstruction secondary to the impaction of a large gallstone in the proximal gastrointestinal tract. The obstruction occurs as result of a bilio-enteric or bilio-gastric fistula. This clinical entity is a rare variant of the more commonly recognized gallstone ileus, which tends to cause small bowel obstruction of the terminal ileum. The typical presentation of Bouveret syndrome consists of nausea, vomiting and abdominal pain secondary to obstruction. Diagnosis often requires radiographic imaging with computed tomography, which typically shows pneumobilia or a cholecystoduodenal fistula. Herein is a series consisting of three cases of Bouveret syndrome involving a bilioenteric, cholecystoduodenal, and choledochoduodenal fistula, respectfully, all of which required operative management. A discussion of the current literature regarding management of this rare syndrome follows.
Figure
-
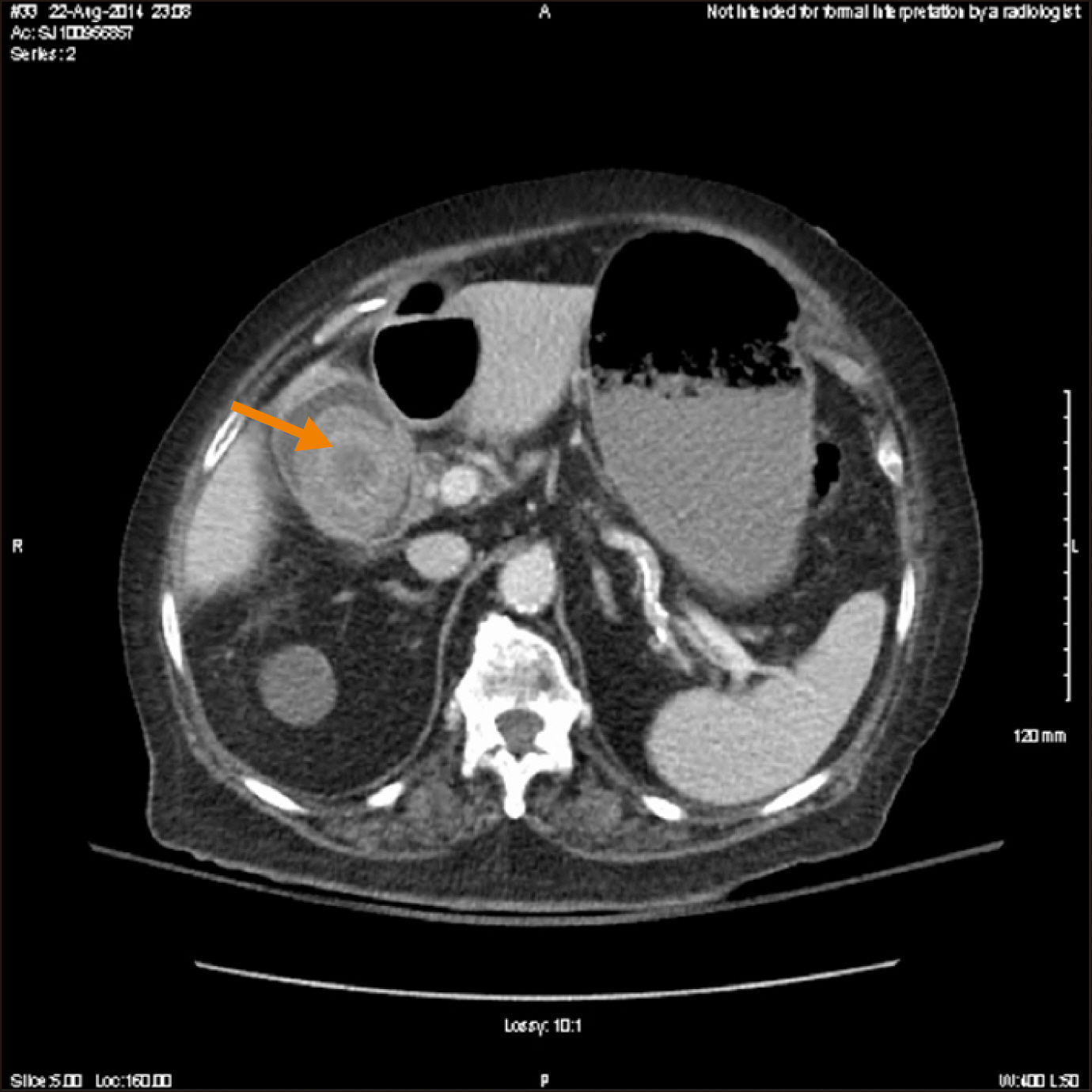
Fig. 1 Computed tomography images of an enlarging intraluminal gallstone. Axial view demonstrating interval enlargement of a gallstone within the gallbladder lumen. Arrow points to gallstone.
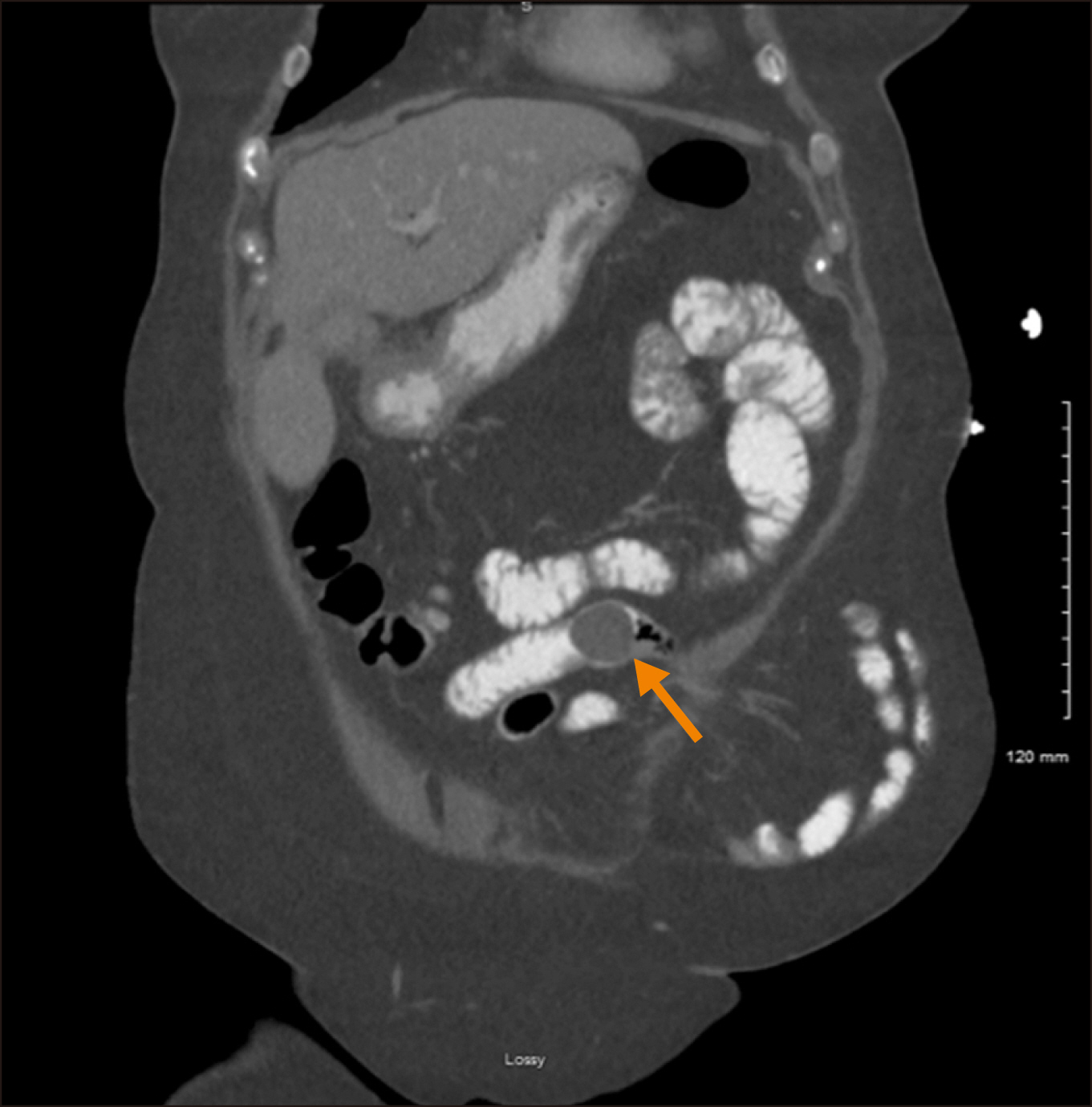
Fig. 2 Computed tomography images showing jejunal gallstone. Coronal view demonstrating distal migration of the gallstone from the duodenum to the jejunum. Arrow points to gallstone.
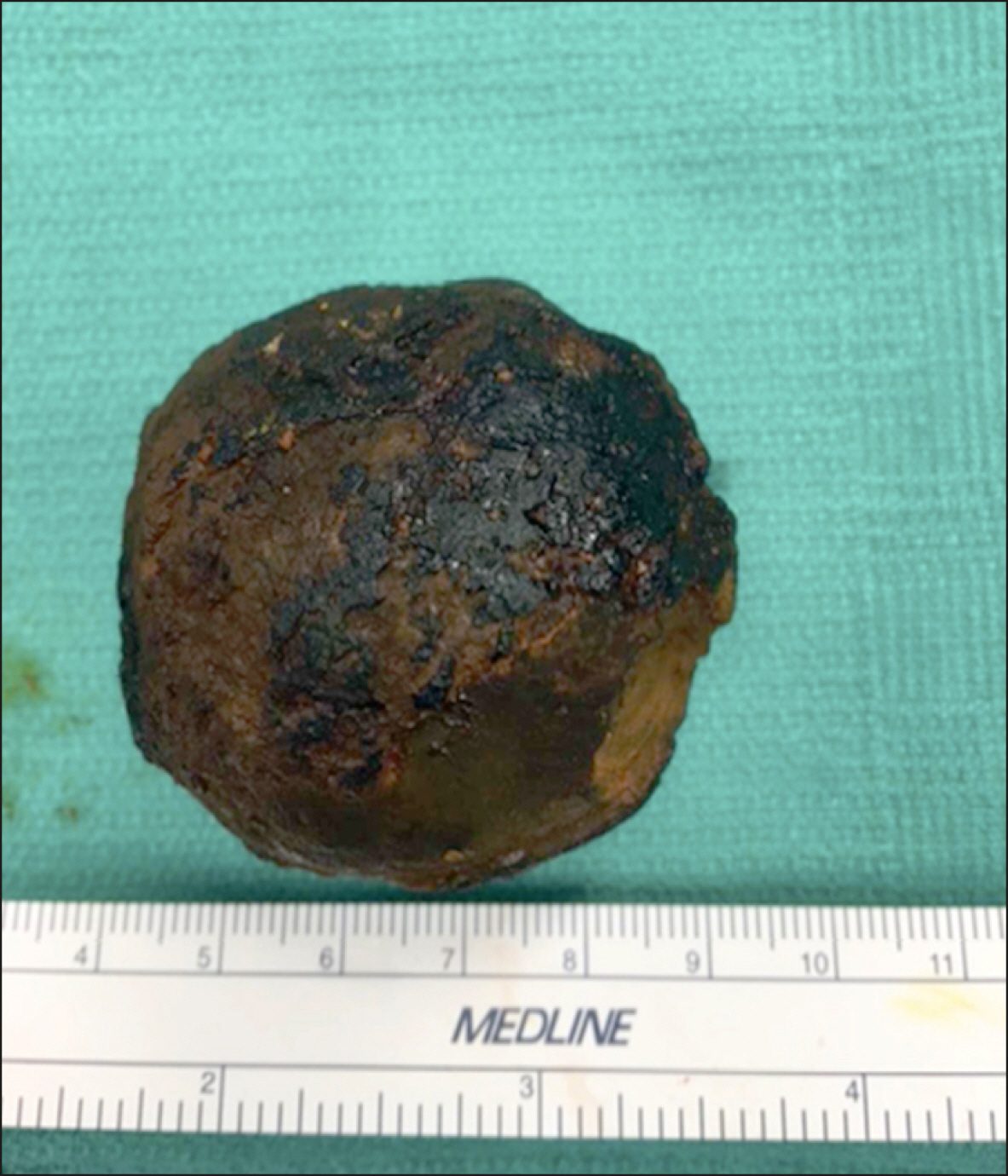
Fig. 3 Gross pathologic specimen from surgery. This image demonstrates the gross pathology of a large gallstone measuring 5 cm.
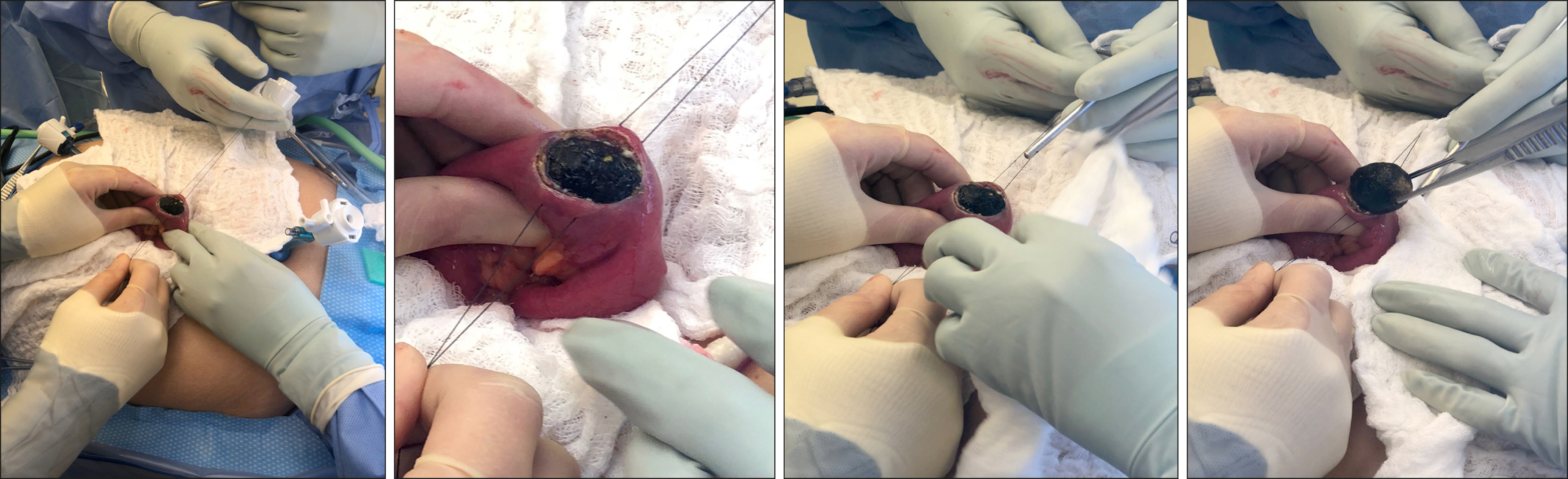
Fig. 4 Gross view of enterotomy created for stone extraction.
Reference
-
1. O'Neill C, Colquhoun P, Schlachta CM, Etemad-Rezai R, Jayaraman S. 2009; Gastric outlet obstruction secondary to biliary calculi: 2 cases of Bouveret syndrome. Can J Surg. 52:E16–E18. PMID: 19234638. PMCID: PMC2637630.2. Iancu C, Bodea R, Al Hajjar N, Todea-Iancu D, Bălă O, Acalovschi I. 2008; Bouveret syndrome associated with acute gangrenous cholecystitis. J Gastrointestin Liver Dis. 17:87–90. PMID: 18392252.3. Masannat YA, Caplin S, Brown T. 2006; A rare complication of a common disease: Bouveret syndrome, a case report. World J Gastroenterol. 12:2620–2621. DOI: 10.3748/wjg.v12.i16.2620. PMID: 16688813. PMCID: PMC4088000.
Article4. Cappell MS, Davis M. 2006; Characterization of Bouveret's syndrome: a comprehensive review of 128 cases. Am J Gastroenterol. 101:2139–2146. DOI: 10.1111/j.1572-0241.2006.00645.x. PMID: 16817848.
Article5. Ramos GP, Chiang NE. 2018; Bouveret's syndrome. N Engl J Med. 378:1335. DOI: 10.1056/NEJMicm1711592. PMID: 29617586.
Article6. Brennan GB, Rosenberg RD, Arora S. 2004; Bouveret syndrome. Radiographics. 24:1171–1175. DOI: 10.1148/rg.244035222. PMID: 15256636.
Article7. Caldwell KM, Lee SJ, Leggett PL, Bajwa KS, Mehta SS, Shah SK. 2018; Bouveret syndrome: current management strategies. Clin Exp Gastroenterol. 11:69–75. DOI: 10.2147/CEG.S132069. PMID: 29497323. PMCID: PMC5819584.
Article8. Malvaux P, Degolla R, De Saint-Hubert M, Farchakh E, Hauters P. 2002; Laparoscopic treatment of a gastric outlet obstruction caused by a gallstone (Bouveret's syndrome). Surg Endosc. 16:1108–1109. DOI: 10.1007/s004640042033. PMID: 11984680.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging Findings of Intragastric Gallstone and Bouveret's Syndrome
- The most frequent symptoms of postcholecystectomy syndrome for cholelithiasis patients older than 40 years of age
- Clinical Review of Cholelithiasis after Gastric Resection in Patients with Stomach Cancer
- Cholelithiasis in Childhood
- Bouveret's syndrome: a case report and a review of the literature
