Esophageal Thermal Injury after Catheter Ablation for Atrial Fibrillation with High-Power (50 Watts) Radiofrequency Energy
- Affiliations
-
- 1Division of Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2512452
- DOI: http://doi.org/10.4070/kcj.2020.0323
Abstract
- Background and Objectives
Data regarding the safety of atrial fibrillation (AF) ablation using high-power (50 W) radiofrequency (RF) energy in Asian populations are limited. This study was conducted to evaluate the incidence and pattern of esophageal injury after highpower AF ablation in an Asian cohort.
Methods
We searched the prospective AF ablation registry to identify patients who underwent AF ablation with 50 W RF energy using the smart touch surround flow catheter (Biosense Webster, Diamond Bar, CA, USA). Visitag™ (Biosense Webster) was used for lesion annotation with predefined settings of catheter stability (3 mm for 5 seconds) and minimum contact force (50% of time >5 g). All patients underwent upper gastrointestinal endoscopy at 1 or 3 days after the ablation.
Results
A total of 159 patients (mean age: 63±9 years, male: 69%, paroxysmal AF: 45.3%, persistent AF: 27.7%, long-standing persistent AF: 27.0%) were analyzed. Initially, 26 patients underwent pulmonary vein isolation with 50 W for 5 seconds at each point. The remaining 133 patients underwent prolonged RF duration (anterior 10 seconds and posterior 6 seconds). The incidence rates of esophageal erythema/erosion and superficial ulceration were 1.3% for each type of the lesion. Food stasis, a suggestive finding of gastroparesis, was observed in 25 (15.7%) patients. There were no cases of cardiac tamponade, stroke, or death.
Conclusions
In Asian patients, AF ablations using 50 W resulted in very low rates of mild esophageal complications.
Figure
-
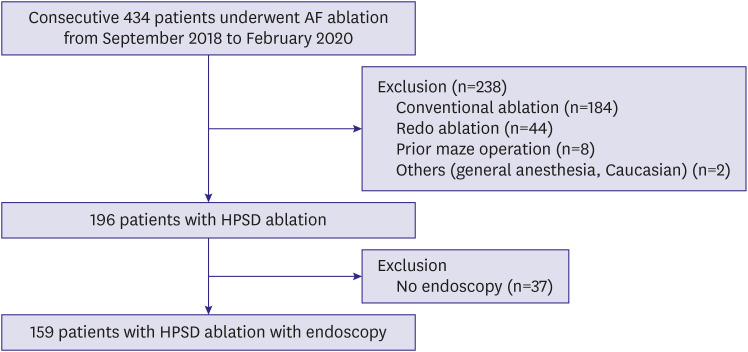
Figure 1 Study flow diagram for inclusion and exclusion.AF = atrial fibrillation; HPSD = high-power, short-duration.
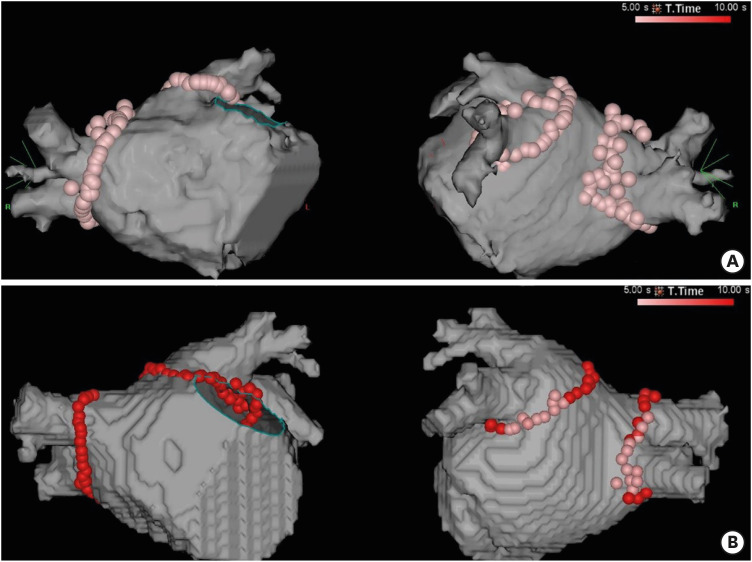
Figure 2 Representative examples of HPSD ablation. (A) shows an example of a patient who underwent PVI using the initial 5-second protocol. Automated lesion tagging with VisiTag (size of 3) was used. (B) shows an example of a patient who underwent PVI using the 6–10 seconds protocol. RF energy was delivered with 50 W for 10 seconds in the anterior and superior wall and 6 seconds in the posterior wall. A tag size of 2 was used, and further ablation was delivered to close the visual gap.HPSD = high-power, short-duration; PVI = pulmonary vein isolation; RF = radiofrequency.
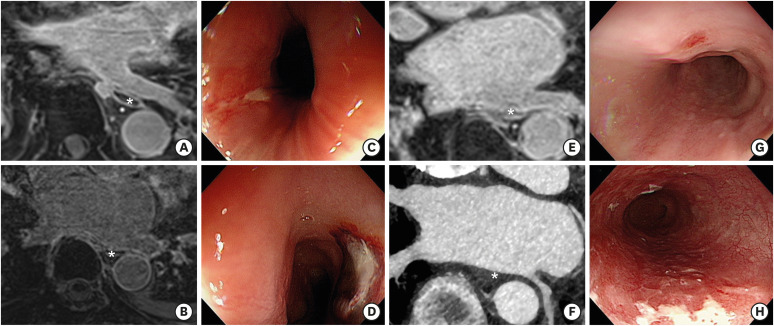
Figure 3 MR images, computed tomographic images, and endoscopic findings of patients with esophageal complications. (A, B) show the MR images of LA, LIPV, and adjacent esophagus (marked with an asterisk) of patients with an esophageal ulcer. (C, D) show the endoscopic findings of superficial esophageal ulcers located at 27 cm and 34 cm from the upper incisor, respectively. (E, F) show the CT images of the esophagus (marked with an asterisk) adjacent to LIPV and posterior wall of LA in patients with esophageal erosion. (G, H) are endoscopic findings of esophageal erosions.CT = computed tomography; LA = left atrium; LIPV = left inferior pulmonary vein; MR = magnetic resonance.
Cited by 1 articles
-
Esophageal Endoscopy after High-power and Short-duration Ablation in Atrial Fibrillation Patients
Dong Geum Shin, Hong Euy Lim
Korean Circ J. 2020;51(2):154-156. doi: 10.4070/kcj.2020.0488.
Reference
-
1. Han HC, Ha FJ, Sanders P, et al. Atrioesophageal fistula: clinical presentation, procedural characteristics, diagnostic investigations, and treatment outcomes. Circ Arrhythm Electrophysiol. 2017; 10:e005579. PMID: 29109075.2. Kim YG, Shim J, Kim DH, et al. Characteristics of atrial fibrillation patients suffering atrioesophageal fistula after radiofrequency catheter ablation. J Cardiovasc Electrophysiol. 2018; 29:1343–1351. PMID: 29927012.
Article3. Martinek M, Bencsik G, Aichinger J, et al. Esophageal damage during radiofrequency ablation of atrial fibrillation: impact of energy settings, lesion sets, and esophageal visualization. J Cardiovasc Electrophysiol. 2009; 20:726–733. PMID: 19207781.
Article4. Leite LR, Santos SN, Maia H, et al. Luminal esophageal temperature monitoring with a deflectable esophageal temperature probe and intracardiac echocardiography may reduce esophageal injury during atrial fibrillation ablation procedures: results of a pilot study. Circ Arrhythm Electrophysiol. 2011; 4:149–156. PMID: 21325208.5. Kumar S, Romero J, Stevenson WG, et al. Impact of lowering irrigation flow rate on atrial lesion formation in thin atrial tissue: preliminary observations from experimental and clinical studies. JACC Clin Electrophysiol. 2017; 3:1114–1125. PMID: 29759494.6. Bunch TJ, Day JD. Novel ablative approach for atrial fibrillation to decrease risk of esophageal injury. Heart Rhythm. 2008; 5:624–627. PMID: 18325845.
Article7. Bhaskaran A, Chik W, Pouliopoulos J, et al. Five seconds of 50–60 W radio frequency atrial ablations were transmural and safe: an in vitro mechanistic assessment and force-controlled in vivo validation. Europace. 2017; 19:874–880. PMID: 27207815.8. Nilsson B, Chen X, Pehrson S, Svendsen JH. The effectiveness of a high output/short duration radiofrequency current application technique in segmental pulmonary vein isolation for atrial fibrillation. Europace. 2006; 8:962–965. PMID: 17043070.
Article9. Winkle RA, Mohanty S, Patrawala RA, et al. Low complication rates using high power (45–50 W) for short duration for atrial fibrillation ablations. Heart Rhythm. 2019; 16:165–169. PMID: 30712645.
Article10. Bunch TJ, May HT, Bair TL, et al. Long-term outcomes after low power, slower movement versus high power, faster movement irrigated-tip catheter ablation for atrial fibrillation. Heart Rhythm. 2020; 17:184–189. PMID: 31398477.
Article11. Lee JH, Nam GB, Go TH, et al. Alternative strategies to improve success rate of mitral isthmus block. Medicine (Baltimore). 2018; 97:e13060. PMID: 30508886.
Article12. Jaïs P, Hocini M, Hsu LF, et al. Technique and results of linear ablation at the mitral isthmus. Circulation. 2004; 110:2996–3002. PMID: 15520313.
Article13. Hocini M, Jaïs P, Sanders P, et al. Techniques, evaluation, and consequences of linear block at the left atrial roof in paroxysmal atrial fibrillation: a prospective randomized study. Circulation. 2005; 112:3688–3696. PMID: 16344401.14. Yarlagadda B, Deneke T, Turagam M, et al. Temporal relationships between esophageal injury type and progression in patients undergoing atrial fibrillation catheter ablation. Heart Rhythm. 2019; 16:204–212. PMID: 30273767.
Article15. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017; 14:e275–444. PMID: 28506916.16. Leshem E, Zilberman I, Tschabrunn CM, et al. High-power and short-duration ablation for pulmonary vein isolation: biophysical characterization. JACC Clin Electrophysiol. 2018; 4:467–479. PMID: 30067486.17. Winkle RA, Mead RH, Engel G, Patrawala RA. Atrial fibrillation ablation: “perpetual motion” of open irrigated tip catheters at 50 W is safe and improves outcomes. Pacing Clin Electrophysiol. 2011; 34:531–539. PMID: 21208229.
Article18. Zhang P, Zhang YY, Ye Q, et al. Characteristics of atrial fibrillation patients suffering esophageal injury caused by ablation for atrial fibrillation. Sci Rep. 2020; 10:2751. PMID: 32066780.
Article19. Kawaji T, Shizuta S, Morimoto T, et al. Very long-term clinical outcomes after radiofrequency catheter ablation for atrial fibrillation: a large single-center experience. Int J Cardiol. 2017; 249:204–213. PMID: 28964553.
Article20. Marrouche NF, Guenther J, Segerson NM, et al. Randomized comparison between open irrigation technology and intracardiac-echo-guided energy delivery for pulmonary vein antrum isolation: procedural parameters, outcomes, and the effect on esophageal injury. J Cardiovasc Electrophysiol. 2007; 18:583–588. PMID: 17490437.
Article21. Chen S, Schmidt B, Bordignon S, et al. Ablation index-guided 50 W ablation for pulmonary vein isolation in patients with atrial fibrillation: procedural data, lesion analysis, and initial results from the FAFA AI High Power Study. J Cardiovasc Electrophysiol. 2019; 30:2724–2731. PMID: 31588620.
Article22. Castrejón-Castrejón S, Martínez Cossiani M, Ortega Molina M, et al. Feasibility and safety of pulmonary vein isolation by high-power short-duration radiofrequency application: short-term results of the POWER-FAST PILOT study. J Interv Card Electrophysiol. 2020; 57:57–65. PMID: 31713704.
Article23. Halm U, Gaspar T, Zachäus M, et al. Thermal esophageal lesions after radiofrequency catheter ablation of left atrial arrhythmias. Am J Gastroenterol. 2010; 105:551–556. PMID: 19888201.
Article24. Halbfass P, Berkovitz A, Pavlov B, et al. Incidence of acute thermal esophageal injury after atrial fibrillation ablation guided by prespecified ablation index. J Cardiovasc Electrophysiol. 2019; 30:2256–2261. PMID: 31559655.
Article25. Knopp H, Halm U, Lamberts R, et al. Incidental and ablation-induced findings during upper gastrointestinal endoscopy in patients after ablation of atrial fibrillation: a retrospective study of 425 patients. Heart Rhythm. 2014; 11:574–578. PMID: 24418167.
Article26. Jhuo SJ, Lo LW, Chang SL, et al. Periesophageal vagal plexus injury is a favorable outcome predictor after catheter ablation of atrial fibrillation. Heart Rhythm. 2016; 13:1786–1793. PMID: 27236026.
Article27. Irastorza RM, d'Avila A, Berjano E. Thermal latency adds to lesion depth after application of high-power short-duration radiofrequency energy: results of a computer-modeling study. J Cardiovasc Electrophysiol. 2018; 29:322–327. PMID: 28988468.
Article28. Black-Maier E, Pokorney SD, Barnett AS, et al. Risk of atrioesophageal fistula formation with contact force-sensing catheters. Heart Rhythm. 2017; 14:1328–1333. PMID: 28416466.
Article29. Schoene K, Arya A, Grashoff F, et al. Oesophageal probe evaluation in radiofrequency ablation of atrial fibrillation (OPERA): results from a prospective randomized trial. Europace. 2020; 22:1487–1494. PMID: 32820324.
Article30. Chen S, Schmidt B, Seegeer A, et al. Catheter ablation of atrial fibrillation using ablation index-guided high power (50 W) for pulmonary vein isolation: with or without esophageal temperature probe? Heart Rhythm. 2020; [Epub ahead of print].
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Chronic Radiodermatitis following Radiofrequency Catheter Ablation for Atrial Fibrillation
- Radiofrequency Catheter Ablation of Persistent Atrial Fibrillation with Myotonic Dystrophy and Achalasia-like Esophageal Dilatation
- Successful Management of Atrio-Esophageal Fistula after Cardiac Radiofrequency Catheter Ablation
- Catheter ablation for treatment of tachyarrhythmia
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
