Whipple disease mimicking inflammatory bowel disease
- Affiliations
-
- 1Department of Pediatrics, Gunma University Graduate School of Medicine, Maebashi, Japan
- 2Department of Endoscopy, University of the Ryukyus, Nishihara, Japan
- 3Clinical Department of Pathology, Gunma University Hospital, Maebashi, Japan
- 4Cell Biology Program, Inflammatory Bowel Disease Centre, The Hospital for Sick Children, Toronto, ON, Canada
- KMID: 2512108
- DOI: http://doi.org/10.5217/ir.2019.09177
Abstract
- Whipple disease is a systemic chronic infection caused by Tropheryma whipplei. Although chronic diarrhea is a common gastrointestinal symptom, diagnosis is often difficult because there are no specific endoscopic findings, and the pathogen is not detectable by stool culture. We present a female patient with Whipple disease who developed chronic bloody diarrhea and growth retardation at the age of 4 years. Colonoscopy showed a mildly edematous terminal ileum and marked erythema without vascular patterns throughout the sigmoid colon and rectum. Subsequently, a primary diagnosis of ulcerative colitis was made. Histopathological analysis of the terminal ileum showed the presence of foamy macrophages filled with periodic acidSchiff-positive particles. Polymerase chain reaction using DNA from a terminal ileum biopsy sample amplified a fragment of 16S rRNA from T. whipplei. Antibiotic treatment relieved the patient’s symptoms. There was no evidence of immunodeficiency in the present case. Since Whipple disease worsens after anti-tumor necrosis factor inhibitor therapy, considering this infection in the differential diagnosis may be important in patients with inflammatory bowel disease, especially before initiation of immunotherapy.
Keyword
Figure
-
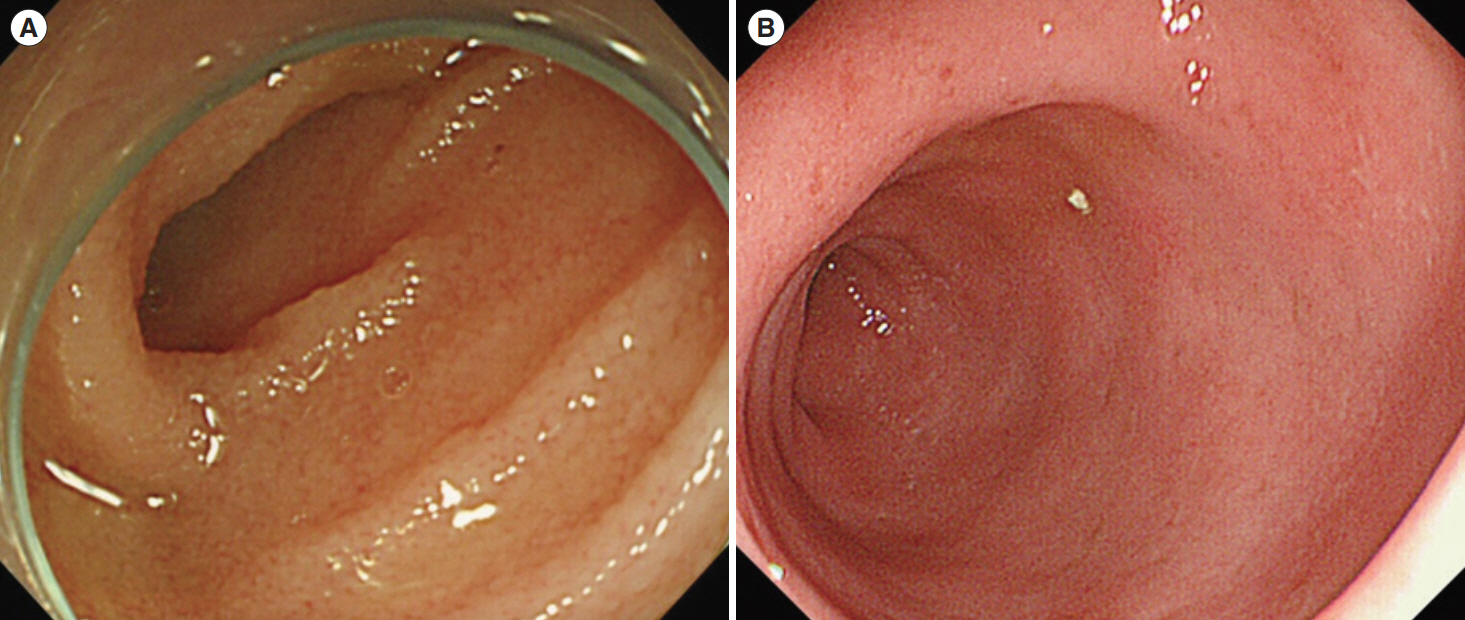
Fig. 1. Endoscopic image of the terminal ileum (A) and sigmoid colon (B) of the patient at the time of admission. The ileum showed mild edema. Colonoscopy showed friability, erythema, absence of vascular patterns, and erosions.
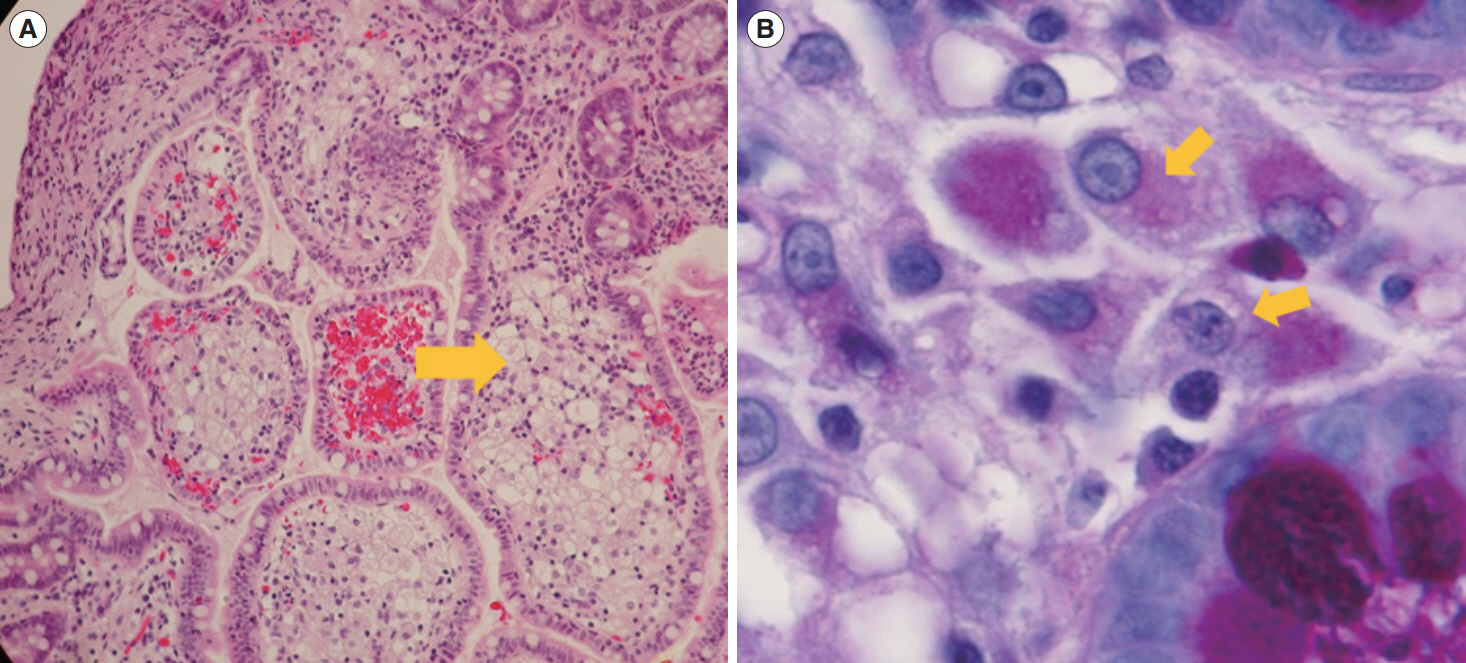
Fig. 2. Histological image of the biopsy specimens from the duodenum and terminal ileum revealed foamy macrophages with intracellular granules. Histological image of the terminal ileum with foamy macrophages. (A) Foamy macrophages are evident in the sample with H&E staining (arrow, ×100). (B) Periodic acid-Schiff positive macrophages are seen in the lamina propria (arrows, ×400).
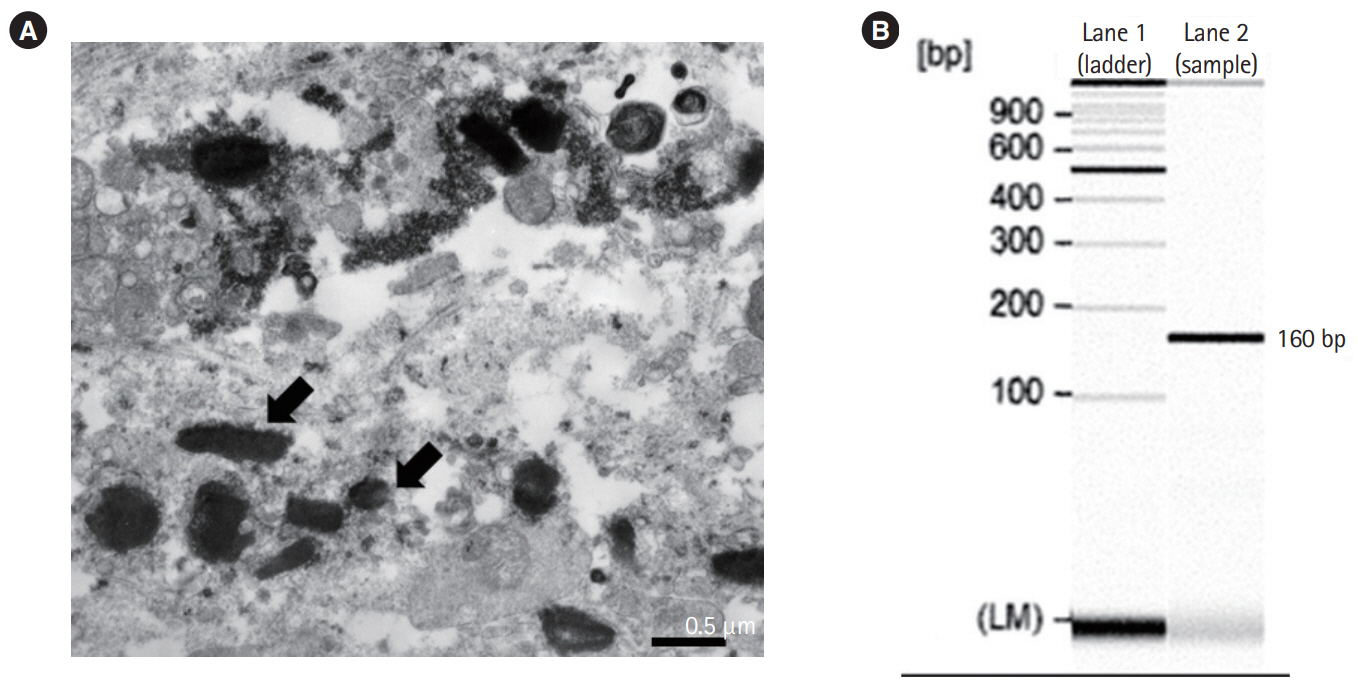
Fig. 3. Electron microscopic findings of the biopsy sample and polymerase chain reaction (PCR) detection of Tropheryma whipplei from the terminal ileum. (A) Numerous rod-shaped bacilli are observed (arrows). (B) The lane shows a PCR product of 160 base pairs specific to the T. whipplei 16S ribosomal RNA.
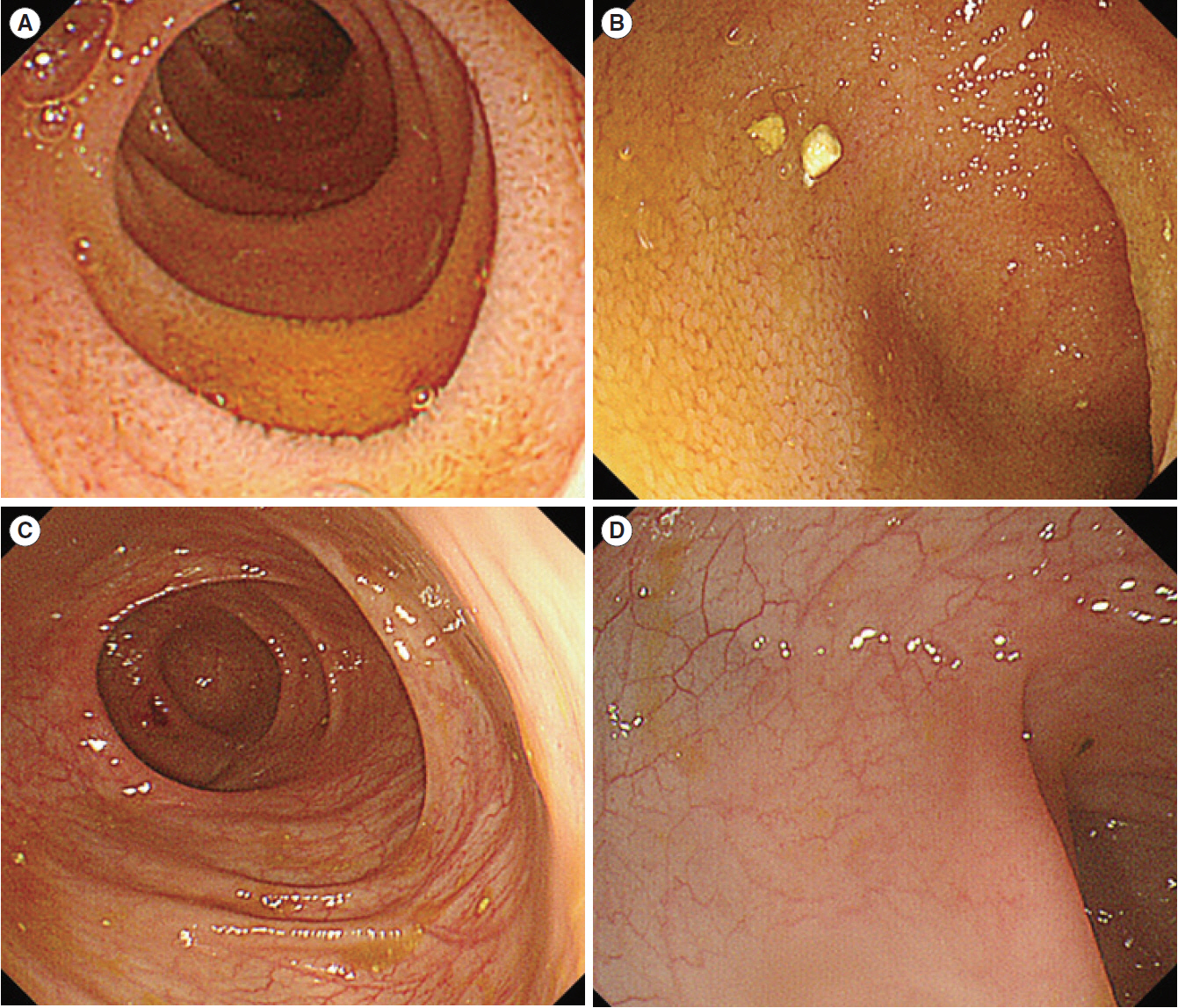
Fig. 4. Endoscopic findings after 12 months of treatment for Whipple disease. Duodenal edema is improved (A), as well as ileal (B) and colonic (C, D) pathological findings.
Reference
-
1. Benchimol EI, Fortinsky KJ, Gozdyra P, Van den Heuvel M, Van Limbergen J, Griffiths AM. Epidemiology of pediatric inflammatory bowel disease: a systematic review of international trends. Inflamm Bowel Dis. 2011; 17:423–439.
Article2. IBD Working Group of the European Society for Paediatric Gastroenterology; Hepatology and Nutrition. Inflammatory bowel disease in children and adolescents: recommendations for diagnosis: the Porto criteria. J Pediatr Gastroenterol Nutr. 2005; 41:1–7.3. Yardley JH, Hendrix TR. Combined electron and light microscopy in Whipple’s disease: demonstration of “bacillary bodies” in the intestine. Bull Johns Hopkins Hosp. 1961; 109:80–98.4. Yajima N, Wada R, Kimura S, et al. Whipple disease diagnosed with PCR using formalin-fixed paraffin-embedded specimens of the intestinal mucosa. Intern Med. 2013; 52:219–222.
Article5. Yogi T, Hokama A, Kinjo F, et al. Whipple’s disease: the first Japanese case diagnosed by electron microscopy and polymerase chain reaction. Intern Med. 2004; 43:566–570.
Article6. Relman DA, Schmidt TM, MacDermott RP, Falkow S. Identification of the uncultured bacillus of Whipple’s disease. N Engl J Med. 1992; 327:293–301.
Article7. Ramzan NN, Loftus E Jr, Burgart LJ, et al. Diagnosis and monitoring of Whipple disease by polymerase chain reaction. Ann Intern Med. 1997; 126:520–527.
Article8. Fenollar F, Puéchal X, Raoult D. Whipple’s disease. N Engl J Med. 2007; 356:55–66.
Article9. Marth T, Moos V, Müller C, Biagi F, Schneider T. Tropheryma whipplei infection and Whipple’s disease. Lancet Infect Dis. 2016; 16:e13–e22.10. Fleming JL, Wiesner RH, Shorter RG. Whipple’s disease: clinical, biochemical, and histopathologic features and assessment of treatment in 29 patients. Mayo Clin Proc. 1988; 63:539–551.
Article11. Patel SJ, Huard RC, Keller C, Foca M. Possible case of CNS Whipple’s disease in an adolescent with AIDS. J Int Assoc Physicians AIDS Care (Chic). 2008; 7:69–73.
Article12. Tan TQ, Vogel H, Tharp BR, Carrol CL, Kaplan SL. Presumed central nervous system Whipple’s disease in a child: case report. Clin Infect Dis. 1995; 20:883–889.
Article13. Duprez TP, Grandin CB, Bonnier C, et al. Whipple disease confined to the central nervous system in childhood. AJNR Am J Neuroradiol. 1996; 17:1589–1591.14. Fenollar F, Minodier P, Boutin A, et al. Tropheryma whipplei associated with diarrhoea in young children. Clin Microbiol Infect. 2016; 22:869–874.15. Günther U, Moos V, Offenmüller G, et al. Gastrointestinal diagnosis of classical Whipple disease: clinical, endoscopic, and histopathologic features in 191 patients. Medicine (Baltimore). 2015; 94:e714.16. Masselot F, Boulos A, Maurin M, Rolain JM, Raoult D. Molecular evaluation of antibiotic susceptibility: Tropheryma whipplei paradigm. Antimicrob Agents Chemother. 2003; 47:1658–1664.
Article17. Marth T. Systematic review: Whipple’s disease (Tropheryma whipplei infection) and its unmasking by tumour necrosis factor inhibitors. Aliment Pharmacol Ther. 2015; 41:709–724.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Abdominal Pain over 6 Months
- The Pharmacotherapy of Inflammatory Bowel Disease in Child and Adolescence
- Inflammatory Bowel Disease in Pediatric Age
- Can vitamin D supplementation help control inflammation in inflammatory bowel disease beyond its classical role in bone health?
- The old versus the new: which do you keep in postoperative Crohn's disease?
