The application of “bone window technique” using piezoelectric saws and a CAD/CAM-guided surgical stent in endodontic microsurgery on a mandibular molar case
- Affiliations
-
- 1Microscope Center, Department of Conservative Dentistry and Oral Science Research Center, Yonsei University College of Dentistry, Seoul, Korea
- 2Department of Electrical & Electronic Engineering, Yonsei University College of Engineering, Seoul, Korea
- KMID: 2512018
- DOI: http://doi.org/10.5395/rde.2020.45.e27
Abstract
- Apical surgery for a mandibular molar is still challenging for many reasons. This report describes the applications of computer-guided cortical ‘bone-window technique’ using piezoelectric saws that prevented any nerve damage in performing endodontic microsurgery of a mandibular molar. A 49-year-old woman presented with gumboil on tooth #36 (previously endodontically treated tooth) and was diagnosed with chronic apical abscess. Periapical lesions were confirmed using cone-beam computed tomography (CBCT). Endodontic microsurgery for the mesial and distal roots of tooth #36 was planned. Following the transfer of data of the CBCT images and the scanned cast to an implant surgical planning program, data from both devices were merged. A surgical stent was designed, on the superimposed three-dimensional model, to guide the preparation of a cortical window on the buccal side of tooth #36. Endodontic microsurgery was performed with a printed surgical template. Minimal osteotomy was required and preservation of the buccal cortical plate rendered this endodontic surgery less traumatic. No postoperative complications such as mental nerve damage were reported. Window technique guided by a computer-aided design/computer-aided manufacture based surgical template can be considerably useful in endodontic microsurgery in complicated cases.
Keyword
Figure
-
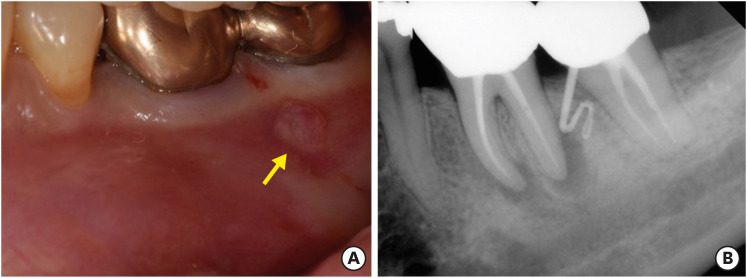
Figure 1 (A) The clinical image of tooth #36 with the sinus tract on buccal gingiva (yellow arrow). (B) The initial periapical radiograph of tooth #36 showing periapical lesions and gutta percha tracing revealing the origin of the sinus tract was the distal root of tooth #36.
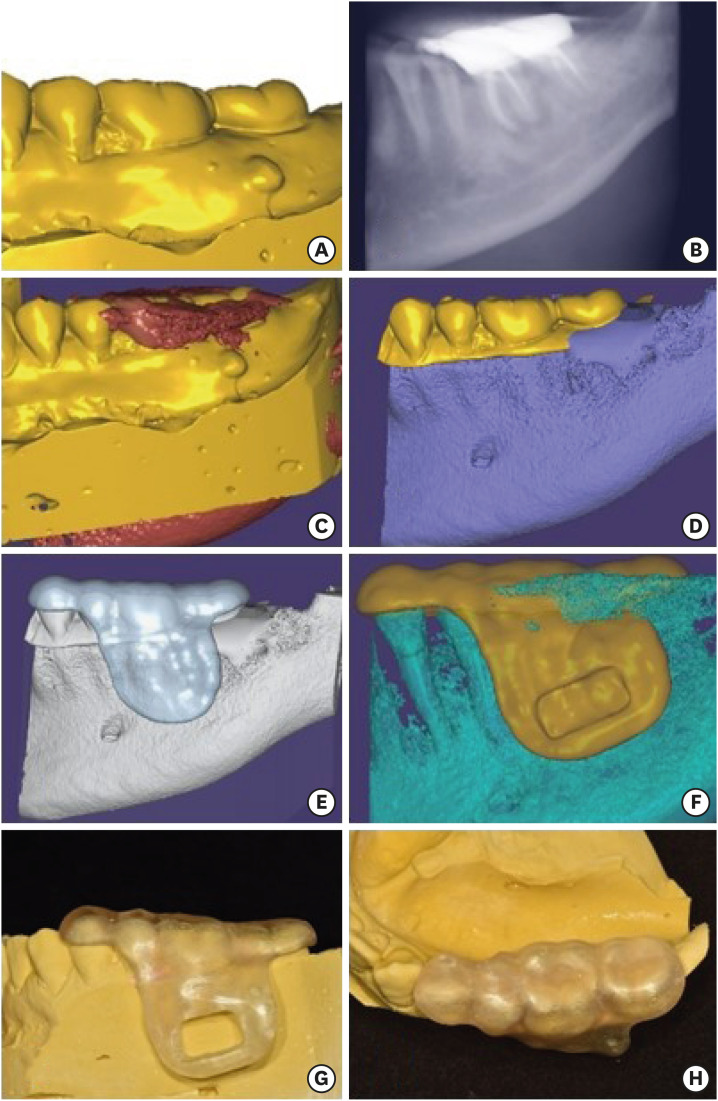
Figure 2 (A) Scanning data of the cast. (B) Cone-beam computed tomography (CBCT) image of the tooth uploaded to the surgical planning software. (C) Superimposition of the scanned cast and the CBCT image. (D) The coronal portion of the scanned cast above the level of the marginal gingiva and the gingival portion of the CBCT data were selected and merged. (E) The initial design of the surgical template without window. (F) The final design of the surgical template with window. (G, H) The buccal and the occlusal view of the 3D printed surgical template for endodontic surgery on tooth #36.
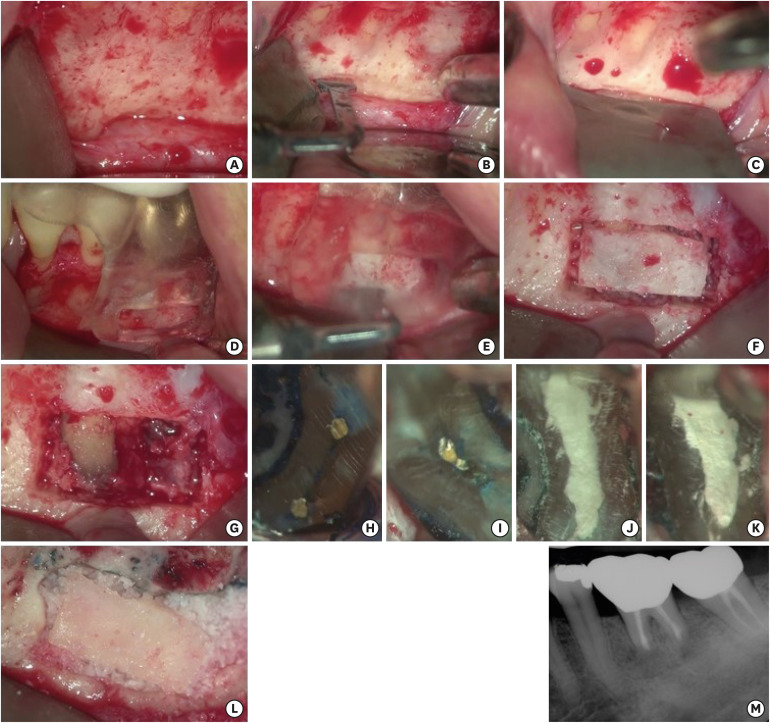
Figure 3 (A) After flap reflection, metal foramen and mental nerve was identified. (B) A groove was made using the piezoelectric saw on the coronal side of the mental foramen to protect it. (C) A KP1 retractor was placed on the groove. (D) The surgical template was positioned on tooth #36. (E) Guided osteotomy for preparation of the cortical window was performed using piezoelectric saws. (F) Bone preparation for the cortical window. (G) Uncovered area of the lesion and the apices of the roots. (H) The resected root surface inspected under high magnification. An isthmus was observed on the mesial root. (I) The resected root surface inspected under high magnification. An isthmus was observed on the distal root. (J, K) Root-end filling with Retro MTA on the mesial root and the distal root were confirmed under high magnification. (L) Allogenic bone was grafted and cortical bone was repositioned. (M) The postoperative periapical radiograph.
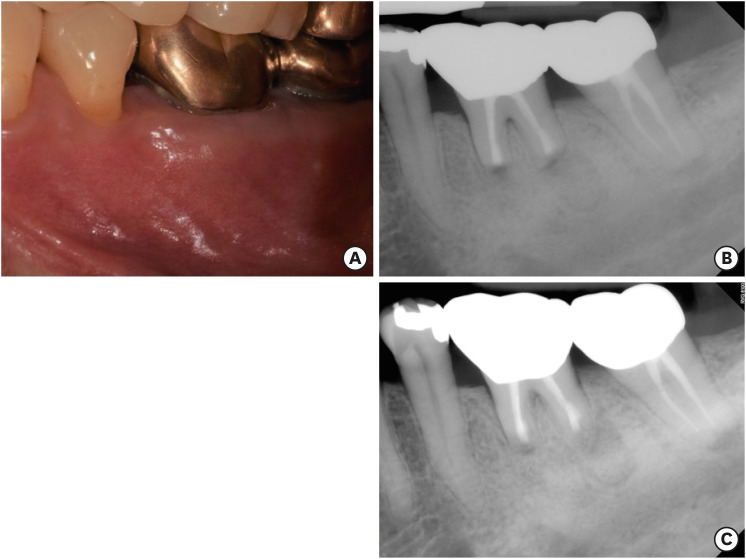
Figure 4 (A) The 6 months follow-up clinical image. (B) The 6 months follow-up periapical radiograph. (C) The 12 months follow-up periapical radiograph.
Reference
-
1. Kang M, Jung HI, Song M, Kim SY, Kim HC, Kim E. Outcome of nonsurgical retreatment and endodontic microsurgery: a meta-analysis. Clin Oral Investig. 2015; 19:569–582.
Article2. Gorni FG, Gagliani MM. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod. 2004; 30:1–4. PMID: 14760899.
Article3. Setzer FC, Shah SB, Kohli MR, Karabucak B, Kim S. Outcome of endodontic surgery: a meta-analysis of the literature--part 1: comparison of traditional root-end surgery and endodontic microsurgery. J Endod. 2010; 36:1757–1765. PMID: 20951283.
Article4. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006; 32:601–623. PMID: 16793466.
Article5. Song M, Kim SG, Lee SJ, Kim B, Kim E. Prognostic factors of clinical outcomes in endodontic microsurgery: a prospective study. J Endod. 2013; 39:1491–1497. PMID: 24238435.
Article6. Zhou W, Zheng Q, Tan X, Song D, Zhang L, Huang D. Comparison of mineral trioxide aggregate and iRoot BP Plus Root Repair Material as root-end filling materials in endodontic microsurgery: a prospective randomized controlled study. J Endod. 2017; 43:1–6. PMID: 27986096.
Article7. Kim S, Jung H, Kim S, Shin SJ, Kim E. The influence of an isthmus on the outcomes of surgically treated molars: a retrospective study. J Endod. 2016; 42:1029–1034. PMID: 27238415.
Article8. von Arx T, Hänni S, Jensen SS. Correlation of bone defect dimensions with healing outcome one year after apical surgery. J Endod. 2007; 33:1044–1048. PMID: 17931929.9. Sisk AL, Hammer WB, Shelton DW, Joy ED Jr. Complications following removal of impacted third molars: the role of the experience of the surgeon. J Oral Maxillofac Surg. 1986; 44:855–859. PMID: 3464711.
Article10. Pinsky HM, Champleboux G, Sarment DP. Periapical surgery using CAD/CAM guidance: preclinical results. J Endod. 2007; 33:148–151. PMID: 17258633.
Article11. Strbac GD, Schnappauf A, Giannis K, Moritz A, Ulm C. Guided modern endodontic surgery: a novel approach for guided osteotomy and root resection. J Endod. 2017; 43:496–501. PMID: 28139285.
Article12. Song M, Kim SG, Shin SJ, Kim HC, Kim E. The influence of bone tissue deficiency on the outcome of endodontic microsurgery: a prospective study. J Endod. 2013; 39:1341–1345. PMID: 24139252.
Article13. Gutmann JL, Harrison JW. Posterior endodontic surgery: anatomical considerations and clinical techniques. Int Endod J. 1985; 18:8–34. PMID: 3858237.
Article14. Capuzzi P, Montebugnoli L, Vaccaro MA. Extraction of impacted third molars. A longitudinal prospective study on factors that affect postoperative recovery. Oral Surg Oral Med Oral Pathol. 1994; 77:341–343. PMID: 8015796.15. Mora MA, Chenin DL, Arce RM. Software tools and surgical guides in dental-implant-guided surgery. Dent Clin North Am. 2014; 58:597–626. PMID: 24993925.
Article16. Floratos S, Kim S. Modern endodontic microsurgery concepts: a clinical update. Dent Clin North Am. 2017; 61:81–91. PMID: 27912820.17. Blumenthal NM. A clinical comparison of collagen membranes with e-PTFE membranes in the treatment of human mandibular buccal class II furcation defects. J Periodontol. 1993; 64:925–933. PMID: 8277399.
Article18. Seibert JS. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ Dent. 1983; 4:437–453. PMID: 6578906.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Apicoectomy of maxillary anterior teeth through a piezoelectric bony-window osteotomy: two case reports introducing a new technique to preserve cortical bone
- Leukocyte platelet-rich fibrin in endodontic microsurgery: a report of 2 cases
- A case of digital maxillary complete denture and mandibular implant overdenture fabricated by CAD-CAM technique
- A CAD/CAM-based strategy for concurrent endodontic and restorative treatment
- Fabrication of maxillary complete denture and mandibular implant retained overdenture using CAD-CAM system and Monolithic disc: a case report
