Effect of Fascia Penetration in Lateral Femoral Cutaneous Nerve Conduction
- Affiliations
-
- 1Department of Rehabilitation Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
- KMID: 2510813
- DOI: http://doi.org/10.5535/arm.20022
Abstract
Objective
To evaluate the effect of fascia penetration and develop a new technique for lateral femoral cutaneous nerve (LFCN) conduction studies based on the fascia penetration point (PP) identified using ultrasound.
Methods
The fascia PP of the LFCN was localized in 20 healthy subjects, and sensory nerve action potentials (SNAPs) were obtained at four different stimulation points—2 cm proximal to the PP (2PPP), PP, 2 cm distal to the PP (2DPP), and 4 cm distal to the PP (4DPP). We compared the stimulation technique based on the fascia penetration point (STBFP) with the conventional technique.
Results
The SNAP amplitude of the LFCN was significantly higher when stimulation was performed at the PP and 2DPP than at other stimulation points. Using the STBFP, SNAP responses were elicited in 38 of 40 legs, whereas they were elicited in 32 of 40 legs using the conventional technique (p=0.041). STBFP had a comparable SNAP amplitude and slightly delayed negative peak latency compared to the conventional technique. In terms of the time required, the time spent on STBFP showed a more consistent distribution than the time spent on the conventional technique (two-sample Kolmogorov–Smirnov test, p<0.05).
Conclusion
SNAP of the LFCN significantly changed near the fascia PP, and stimulation at PP and at 2DPP provided high amplitudes. STBFP can help increase the response rate and ensure stable and consistent procedure time of the LFCN conduction study.
Keyword
Figure
-
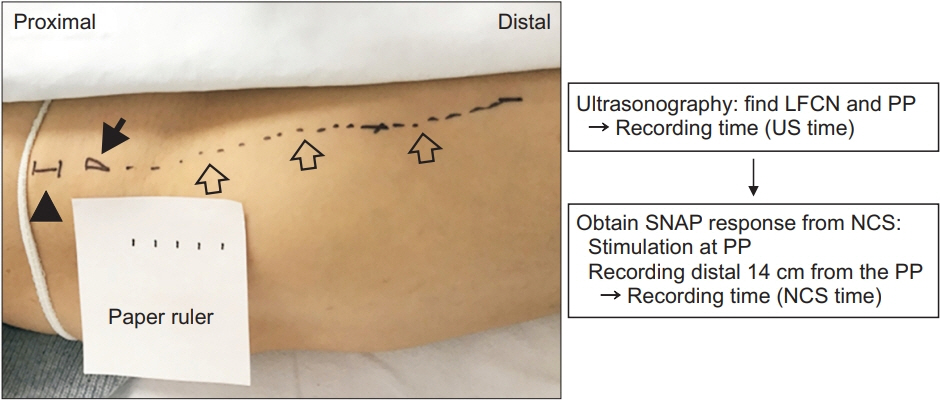
Fig. 1. The study protocol of the stimulation technique based on the fascia penetration point. ① Find LFCN using sonography and mark the fascia PP (filled arrow), the nerve course (unfilled arrow) and ASIS (black arrowhead) on the surface of right thigh as shown in left image. ② Evaluate the time spent on US. ③ Stimulate the fascia PP and obtain SNAP at recording site distal 14 cm from the stimulation point. ④ Evaluate the time spent on NCS and VAS. The white paper ruler (scale drawn on white paper at 1 cm intervals) is placed alongside the nerve course marking. Left side of the image is proximal. LFCN, lateral femoral cutaneous nerve; PP, penetration point; ASIS, anterior superior iliac spine; US, ultrasonography; SNAP, sensory nerve action potential; NCS, nerve conduction study; VAS, visual analogue scale.
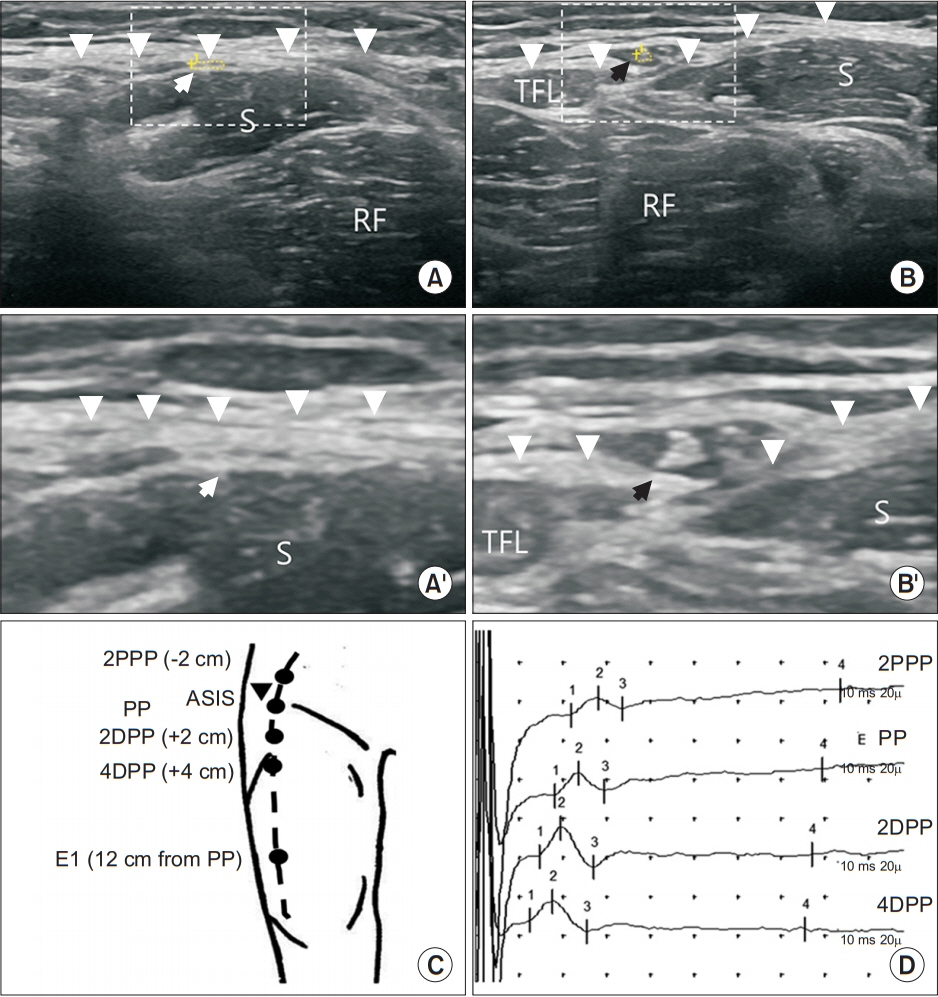
Fig. 2. Sonography and sensory nerve conduction study of the lateral femoral cutaneous nerve. (A) Lateral femoral cutaneous nerve (dotted circle with white arrow) beneath the fascia lata (arrowheads). (B) Lateral femoral cutaneous nerve (dotted circle with black arrow) just after penetrating the fascia. (A’) Enlarged image of the part indicated by a dotted rectangle in panel A. (B’) Enlarged image of the part indicated by a dotted rectangle in panel B. (C) Stimulation point based on the PP in the lateral femoral cutaneous nerve conduction study. (D) Sensory nerve action potentials at different stimulation points. RF, rectus femoris muscle; TFL, tensor fascia lata muscle; S, sartorius muscle; 2PPP, 2 cm proximal to the penetration point; PP, the penetration point ; 2DPP, 2 cm distal to the penetration point ; 4DPP, 4 cm distal to the penetration point; ASIS, anterior superior iliac spine.

Fig. 3. Comparison of time spent on conventional technique and STBFP. Histogram shows spending time of two techniques, conventional technique (red) and STBFP (blue). The distribution of two histograms are significantly different according to the two-sample KolmogorovSmirnov test (D=0.342, p-value=0.0173). STBFP, stimulation based on fascia penetration.
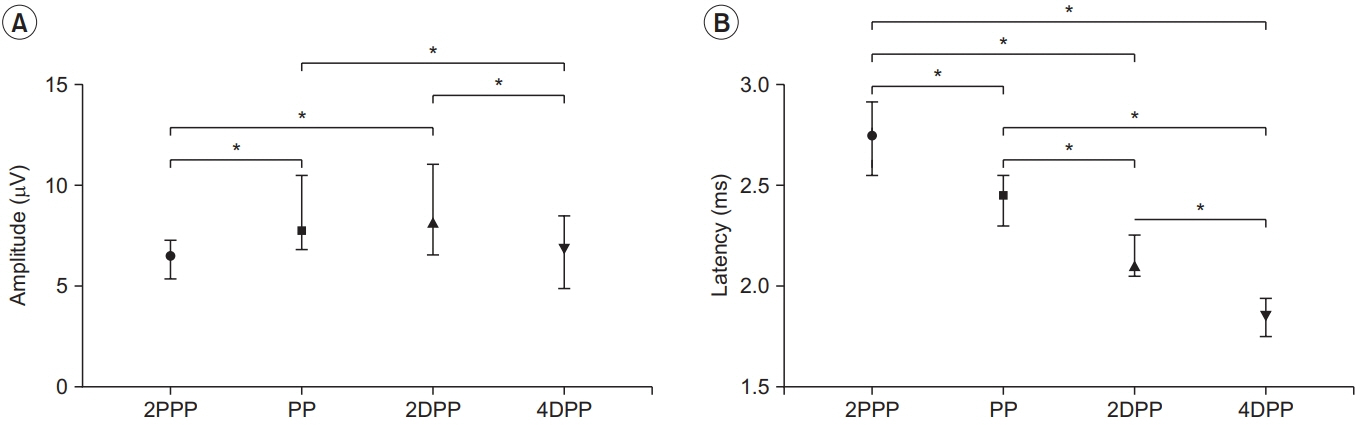
Fig. 4. Comparison of parameters between four different stimulation points based on the PP in the lateral femoral cutaneous nerve conduction study. (A) SNAP amplitude and (B) SNAP negative peak latency at each stimulation point as median and interquartile range. *p<0.0083 comparison by post-hoc analysis (Mann-Whitney U test with Bonferroni correction), significant differences between groups. SNAP, sensory nerve action potential; 2PPP, 2 cm proximal to the penetration point; PP, penetration point; 2DPP, 2 cm distal to the penetration point; 4DPP, 4 cm distal to the penetration point.
Reference
-
1. Tomaszewski KA, Popieluszko P, Henry BM, Roy J, Sanna B, Kijek MR, et al. The surgical anatomy of the lateral femoral cutaneous nerve in the inguinal region: a meta-analysis. Hernia. 2016; 20:649–57.
Article2. Anloague PA, Huijbregts P. Anatomical variations of the lumbar plexus: a descriptive anatomy study with proposed clinical implications. J Man Manip Ther. 2009; 17:e107–14.
Article3. Ghent WR. Meralgia paraesthetica. Can Med Assoc J. 1959; 81:631–3.4. Butler ET, Johnson EW, Kaye ZA. Normal conduction velocity in the lateral femoral cutaneous nerve. Arch Phys Med Rehabil. 1974; 55:31–2.5. Spevak MK, Prevec TS. A noninvasive method of neurography in meralgia paraesthetica. Muscle Nerve. 1995; 18:601–5.
Article6. Boon AJ, Bailey PW, Smith J, Sorenson EJ, Harper CM, Hurdle MF. Utility of ultrasound-guided surface electrode placement in lateral femoral cutaneous nerve conduction studies. Muscle Nerve. 2011; 44:525–30.
Article7. Park BJ, Joeng ES, Choi JK, Kang S, Yoon JS, Yang SN. Ultrasound-guided lateral femoral cutaneous nerve conduction study. Ann Rehabil Med. 2015; 39:47–51.
Article8. Deimel GW, Hurst RW, Sorenson EJ, Boon AJ. Utility of ultrasound-guided near-nerve needle recording for lateral femoral cutaneous sensory nerve conduction study: does it increase reliability compared with surface recording? Muscle Nerve. 2013; 47:274–6.
Article9. Park GY, Im S, Lee JI, Lim SH, Ko YJ, Chung ME, et al. Effect of superficial peroneal nerve fascial penetration site on nerve conduction studies. Muscle Nerve. 2010; 41:227–33.
Article10. Park HJ, Yoon JS, Rhee WI, Kim JW, Yang SN, Won SJ. Effect of fascia penetration on sensory nerve conduction in the superficial radial nerve. J Clin Neurophysiol. 2018; 35:263–6.
Article11. Hanna A. The lateral femoral cutaneous nerve canal. J Neurosurg. 2017; 126:972–8.
Article12. Sarala PK, Nishihara T, Oh SJ. Meralgia paresthetica: electrophysiologic study. Arch Phys Med Rehabil. 1979; 60:30–1.13. Jefferson D, Eames RA. Subclinical entrapment of the lateral femoral cutaneous nerve: an autopsy study. Muscle Nerve. 1979; 2:145–54.
Article14. Shin YB, Park JH, Kwon DR, Park BK. Variability in conduction of the lateral femoral cutaneous nerve. Muscle Nerve. 2006; 33:645–9.
Article15. Ray B, D’Souza AS, Kumar B, Marx C, Ghosh B, Gupta NK, et al. Variations in the course and microanatomical study of the lateral femoral cutaneous nerve and its clinical importance. Clin Anat. 2010; 23:978–84.
Article16. Dias Filho LC, Valenca MM, Guimaraes Filho FA, Medeiros RC, Silva RA, Morais MG, et al. Lateral femoral cutaneous neuralgia: an anatomical insight. Clin Anat. 2003; 16:309–16.
Article17. Majkrzak A, Johnston J, Kacey D, Zeller J. Variability of the lateral femoral cutaneous nerve: an anatomic basis for planning safe surgical approaches. Clin Anat. 2010; 23:304–11.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Schwannoma on the Lateral Side of the Proximal Thigh
- Lateral Femoral Cutaneous Nerve Conduction Study
- The ascending branch of the lateral circumflex femoral artery penetrating the posterior division of the femoral nerve
- Superficial Peroneal Nerve Conduction Study
- Management of Meralgia Paresthetica by Lateral Femoral Cutaneous Nerve Block: Case reports
