Acute Crit Care.
2020 Nov;35(4):271-278. 10.4266/acc.2020.00479.
Postextubation respiratory events in patients admitted to the intensive care unit: a prospective pilot study using overnight respiratory polygraphy
- Affiliations
-
- 1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Seoul, Korea
- 2Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea
- 3Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea
- KMID: 2510546
- DOI: http://doi.org/10.4266/acc.2020.00479
Abstract
- Background
Before the main trial in which respiratory polygraphy will be used to evaluate postextubation sleep apnea in critically ill patients, we performed a prospective pilot study to ensure that any issues with the conduct of the trial would be identified.
Methods
In the present study, 13 adult patients who had received mechanical ventilation for ≥24 hours were prospectively recruited. Among the patients, 10 successfully completed respiratory polygraphy on the first or second night after extubation. Data regarding the types and doses of corticosteroids, analgesics, sedatives, and muscle relaxants as well as the methods of oxygen delivery were recorded.
Results
During the night of respiratory polygraphy, all 10 patients received supplemental oxygen (low-flow oxygen, n=5; high-flow oxygen, n=5), and seven patients received intravenous corticosteroids. Three of the 10 patients had a respiratory event index (REI) ≥5/hr. All respiratory events were obstructive episodes. None of the patients receiving high-flow oxygen therapy had an REI ≥5/hr. Two of the seven patients who received corticosteroids and one of the other three patients who did not receive this medication had an REI ≥5/hr. Although low- or high-flow oxygen therapy was provided, all patients had episodes of oxygen saturation (SpO2) <90%. Two of the three patients with an REI ≥5/hr underwent in-laboratory polysomnography. The patients’ Apnea-Hypopnea Index and REI obtained via polysomnography and respiratory polygraphy, respectively, were similar.
Conclusions
In a future trial to evaluate postextubation sleep apnea in critically ill patients, pre-stratification based on the use of corticosteroids and high-flow oxygen therapy should be considered.
Figure
-
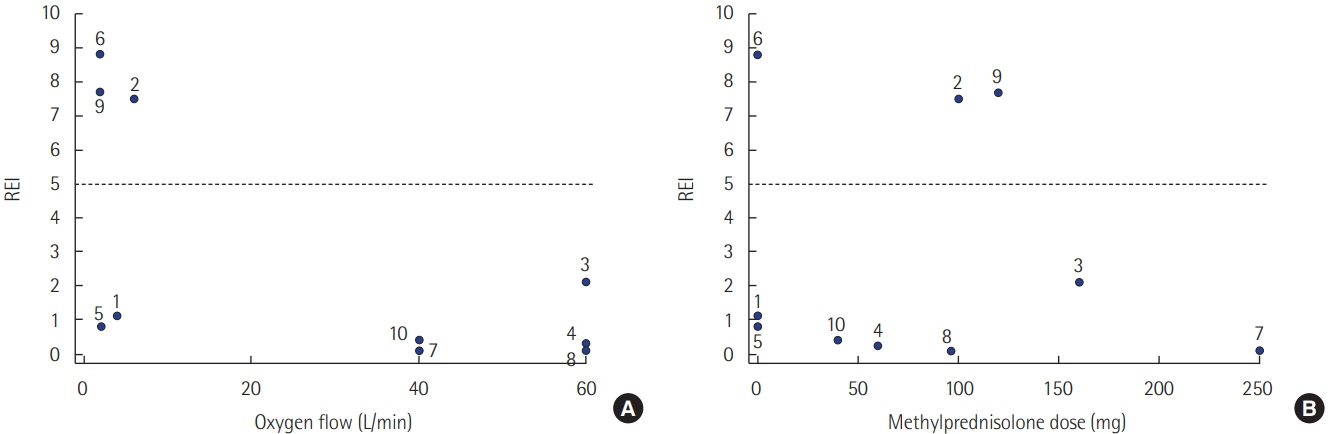
Figure 1. Scatter plots of the postextubation respiratory event index (REI) and (A) the flow rate of oxygen during the night of respiratory polygraphy, and (B) the equivalent dose of methylprednisolone administered 48 hours prior to extubation.
Reference
-
1. Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017; 34:70–81.
Article2. Kryger MH, Roth T, Dement WC. Principles and practice of sleep medicine. Philadelphia: Elsevier;2016.3. Leger D, Bayon V, Laaban JP, Philip P. Impact of sleep apnea on economics. Sleep Med Rev. 2012; 16:455–62.
Article4. Young T, Finn L, Peppard PE, Szklo-Coxe M, Austin D, Nieto FJ, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008; 31:1071–8.5. Jean RE, Gibson CD, Jean RA, Ochieng P. Obstructive sleep apnea and acute respiratory failure: an analysis of mortality risk in patients with pneumonia requiring invasive mechanical ventilation. J Crit Care. 2015; 30:778–83.
Article6. Bolona E, Hahn PY, Afessa B. Intensive care unit and hospital mortality in patients with obstructive sleep apnea. J Crit Care. 2015; 30:178–80.
Article7. Thille AW, Córdoba-Izquierdo A, Maitre B, Boyer L, Brochard L, Drouot X. High prevalence of sleep apnea syndrome in patients admitted to ICU for acute hypercapnic respiratory failure: a preliminary study. Intensive Care Med. 2018; 44:267–9.
Article8. Timm FP, Zaremba S, Grabitz SD, Farhan HN, Zaremba S, Siliski E, et al. Effects of opioids given to facilitate mechanical ventilation on sleep apnea after extubation in the intensive care unit. Sleep. 2018; 41.
Article9. Bergeron C, Kimoff J, Hamid Q. Obstructive sleep apnea syndrome and inflammation. J Allergy Clin Immunol. 2005; 116:1393–6.
Article10. Vicente E, Marin JM, Carrizo SJ, Osuna CS, González R, Marin-Oto M, et al. Upper airway and systemic inflammation in obstructive sleep apnoea. Eur Respir J. 2016; 48:1108–17.
Article11. Ogna A, Forni Ogna V, Mihalache A, Pruijm M, Halabi G, Phan O, et al. Obstructive sleep apnea severity and overnight body fluid shift before and after hemodialysis. Clin J Am Soc Nephrol. 2015; 10:1002–10.
Article12. Montandon G, Qin W, Liu H, Ren J, Greer JJ, Horner RL. Pre-Botzinger complex neurokinin-1 receptor-expressing neurons mediate opioid-induced respiratory depression. J Neurosci. 2011; 31:1292–301.
Article13. Jordan AS, McSharry DG, Malhotra A. Adult obstructive sleep apnoea. Lancet. 2014; 383:736–47.
Article14. Berry RB, Brooks R, Gamaldo C, Harding SM, Lloyd RM, Quan SF, et al. AASM scoring manual updates for 2017 (version 2.4). J Clin Sleep Med. 2017; 13:665–6.
Article15. Chishti A, Batchelor AM, Bullock RE, Fulton B, Gascoigne AD, Baudouin SV. Sleep-related breathing disorders following discharge from intensive care. Intensive Care Med. 2000; 26:426–33.
Article16. Chung F, Liao P, Elsaid H, Shapiro CM, Kang W. Factors associated with postoperative exacerbation of sleep-disordered breathing. Anesthesiology. 2014; 120:299–311.
Article17. Tan HL, Gozal D, Ramirez HM, Bandla HP, Kheirandish-Gozal L. Overnight polysomnography versus respiratory polygraphy in the diagnosis of pediatric obstructive sleep apnea. Sleep. 2014; 37:255–60.
Article18. Bianchi MT, Goparaju B. Potential underestimation of sleep apnea severity by at-home kits: rescoring in-laboratory polysomnography without sleep staging. J Clin Sleep Med. 2017; 13:551–5.
Article19. Kuriyama A, Umakoshi N, Sun R. Prophylactic corticosteroids for prevention of postextubation stridor and reintubation in adults: a systematic review and meta-analysis. Chest. 2017; 151:1002–10.20. Prajapat B, Sandhya AS, Chaudhry D, Esquinas AM. Opioids in intensive care unit (ICU): causal agent for sleep apnea, unmasking the undiagnosed sleep apnea or both in the ICU. Sleep. 2018; 41:zsy081.
Article21. McGinley B, Halbower A, Schwartz AR, Smith PL, Patil SP, Schneider H. Effect of a high-flow open nasal cannula system on obstructive sleep apnea in children. Pediatrics. 2009; 124:179–88.
Article22. McGinley BM, Patil SP, Kirkness JP, Smith PL, Schwartz AR, Schneider H. A nasal cannula can be used to treat obstructive sleep apnea. Am J Respir Crit Care Med. 2007; 176:194–200.
Article23. Joseph L, Goldberg S, Shitrit M, Picard E. High-flow nasal cannula therapy for obstructive sleep apnea in children. J Clin Sleep Med. 2015; 11:1007–10.
Article24. Hawkins S, Huston S, Campbell K, Halbower A. High-flow, heated, humidified air via nasal cannula treats CPAP-intolerant children with obstructive sleep apnea. J Clin Sleep Med. 2017; 13:981–9.
Article25. Amaddeo A, Khirani S, Frapin A, Teng T, Griffon L, Fauroux B. High-flow nasal cannula for children not compliant with continuous positive airway pressure. Sleep Med. 2019; 63:24–8.
Article26. Nishimura M. High-flow nasal cannula oxygen therapy in adults. J Intensive Care. 2015; 3:15.
Article27. Pisani MA, Friese RS, Gehlbach BK, Schwab RJ, Weinhouse GL, Jones SF. Sleep in the intensive care unit. Am J Respir Crit Care Med. 2015; 191:731–8.
Article28. Corral J, Sánchez-Quiroga MÁ, Carmona-Bernal C, Sánchez-Armengol Á, de la Torre AS, Durán-Cantolla J, et al. Conventional polysomnography is not necessary for the management of most patients with suspected obstructive sleep apnea: noninferiority, randomized controlled trial. Am J Respir Crit Care Med. 2017; 196:1181–90.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Early Use of High Flow Nasal Cannula in Postextubation Period: Can It Reduce Reintubation Rate?
- Characteristics Influencing the Occurrence of Respiratory Medical Device-related Pressure Ulcers in the Pediatric Intensive Care Unit
- Can the intensivists predict the outcomes of critically ill patients on the appropriateness of intensive care unit admission for limited intensive care unit resources ?
- Actigraphy-Based Assessment of Sleep Parameters in Intensive Care Unit Patients Receiving Respiratory Support Therapy
- Respiratory Failure Induced by Severe Hypothyroidism in a Korean Woman
