J Pathol Transl Med.
2020 Nov;54(6):504-507. 10.4132/jptm.2020.09.18.
A case of monoclonal gammopathy of renal significance presenting as atypical amyloidosis with IgA lambda paraproteinemia
- Affiliations
-
- 1Department of Anatomical Pathology, SA Pathology, Adelaide, Australia
- 2Central and Northern Adelaide Renal Transplantation Services, Royal Adelaide Hospital, Adelaide, Australia
- KMID: 2509504
- DOI: http://doi.org/10.4132/jptm.2020.09.18
Abstract
- Monoclonal gammopathy of renal significance is defined as any B cell or plasma cell clonal lymphoproliferation which neither causes tumor complications nor meets any current hematological criteria for specific therapy, with one or more kidney lesions related to the produced monoclonal immunoglobulin, such as amyloidosis. A 50-year-old male presented with heavy proteinuria and blood tests showing IgA and Lambda paraproteinemia. Light microscopy showed mesangial eosinophilic ground substance extending into the capillary loops, and positive staining within the glomeruli and vessel walls for amyloid P immunohistochemistry was also noted. Immunofluorescence showed positive staining for IgA and Lambda in the mesangia and capillary loops. Electron microscopy exhibited organized fibrils measuring 4–5 nm in diameter in the mesangia, glomerular basement membranes and vessel walls. We interpreted the overall findings as atypical renal amyloidosis with IgA and Lambda deposition on immunofluorescence. Further amyloid typing using laser microdissection-liquid chromatography and mass spectrometry will be useful.
Keyword
Figure
-
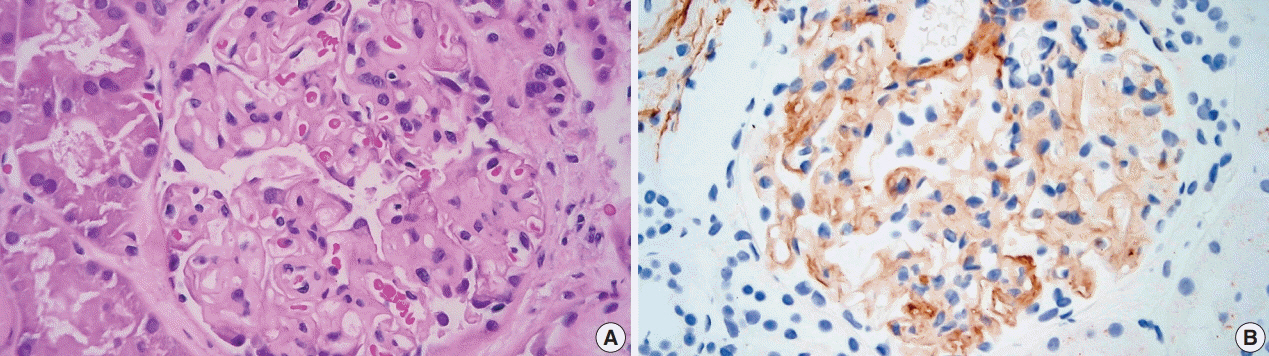
Fig. 1. Hematoxylin and eosin stain and Amyloid P immunohistochemistry. (A) The glomerulus shows mesangial eosinophilic ground substance which extends into the capillary loops. (B) Positive staining is seen within the glomerulus with amyloid P immunohistochemistry.
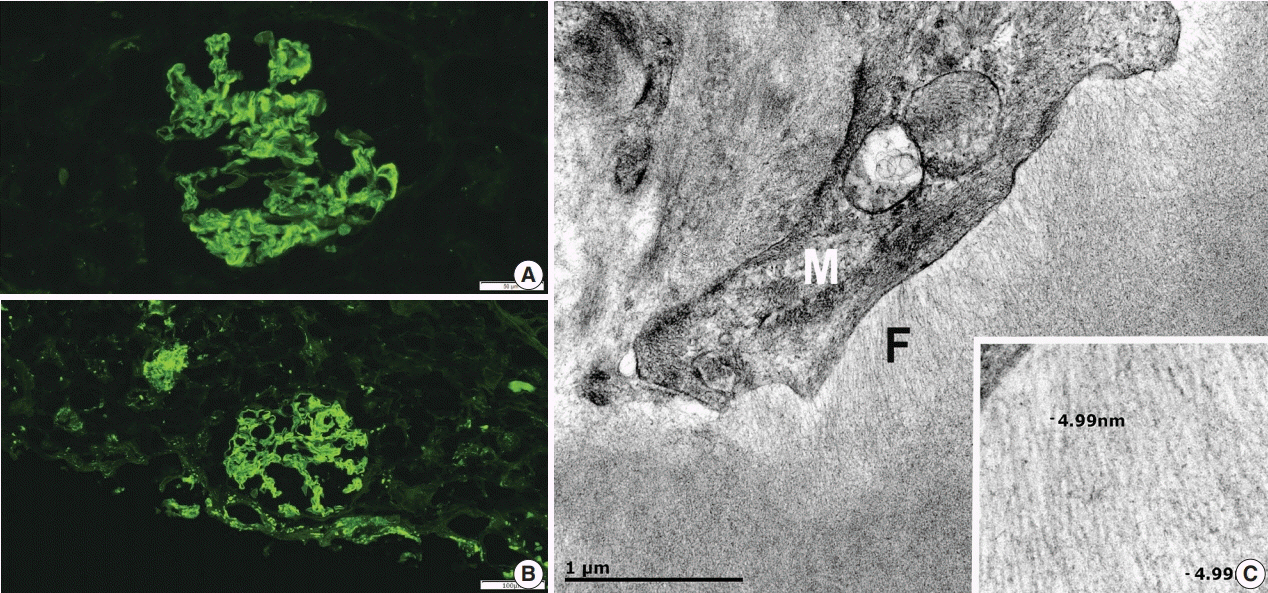
Fig. 2. Immunofluorescence and electron microscopy. (A) Positive mesangial and capillary loop staining with IgA on immunofluorescence. (B) Positive mesangial and capillary loops staining with Lambda on immunofluorescence. (C) The fine fibrillary material (F) is present adjacent to the mesangial cell (M) (×40,000). The inset shows amyloid-like fibrils measuring approximately 5 nm in diameter (×120,000).
Reference
-
References
1. Westermark P, Benson MD, Buxbaum JN, et al. A primer of amyloid nomenclature. Amyloid. 2007; 14:179–83.
Article2. Holanda DG, Acharya VK, Dogan A, Racusen LC, Atta MG. Atypical presentation of atypical amyloid. Nephrol Dial Transplant. 2011; 26:373–6.
Article3. Leung N, Bridoux F, Batuman V, et al. The evaluation of monoclonal gammopathy of renal significance: a consensus report of the International Kidney and Monoclonal Gammopathy Research Group. Nat Rev Nephrol. 2019; 15:45–59.
Article4. Leung N, Drosou ME, Nasr SH. Dysproteinemias and glomerular disease. Clin J Am Soc Nephrol. 2018; 13:128–39.
Article5. Suhr OB, Lundgren E, Westermark P. One mutation, two distinct disease variants: unravelling the impact of transthyretin amyloid fibril composition. J Intern Med. 2017; 281:337–47.
Article6. Manabe S, Iwasaki C, Hatano M, et al. AL amyloidosis with nonamyloid forming monoclonal immunoglobulin deposition: a case mimicking AHL amyloidosis. BMC Nephrol. 2018; 19:337.
Article7. Nasr SH, Said SM, Valeri AM, et al. The diagnosis and characteristics of renal heavy-chain and heavy/light-chain amyloidosis and their comparison with renal light-chain amyloidosis. Kidney Int. 2013; 83:463–70.
Article8. Nasr SH, Valeri AM, Cornell LD, et al. Renal monoclonal immunoglobulin deposition disease: a report of 64 patients from a single institution. Clin J Am Soc Nephrol. 2012; 7:231–9.
Article9. Vrana JA, Gamez JD, Madden BJ, Theis JD, Bergen HR 3rd, Dogan A. Classification of amyloidosis by laser microdissection and mass spectrometry-based proteomic analysis in clinical biopsy specimens. Blood. 2009; 114:4957–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Polyneuropathy Associated with IgA Paraproteinemia and Amyloidosis: A Case Report and Literature Review
- Concurrence of Fibrillary Glomerulonephritis and AL Amyloidosis Associated with Monoclonal Gammopathy
- Seven Cases of Monoclonal Gammopathies Involving Kidney
- Coexistence of AA and AL Cardiac Amyloidosis in a Patient with Ankylosing Spondylitis Accompanying Monoclonal Gammopathy of Undetermined Significance
- A Patient with IgA Monoclonal Gammopathy Presenting as Myelomatous Pleural Effusion with Axillary Node Involvement
