Modified Suturing Techniques in Carotid Endarterectomy for Reducing the Cerebral Ischemic Time
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Hospital, Chonnam National University Medical School, Gwangju, Korea
- KMID: 2508615
- DOI: http://doi.org/10.3340/jkns.2020.0058
Abstract
Objective
: Carotid endarterectomy (CEA) is an effective surgical procedure for treating symptomatic or asymptomatic patients with carotid stenosis. Many neurosurgeons use a shunt to reduce perioperative ischemic complications. However, the use of shunting is still controversial, and the shunt procedure can cause several complications. In our institution, we used two types of modified arteriotomy suture techniques instead of using a shunt.
Methods
: In technique 1, to prevent ischemic complications, we sutured a third of the arteriotomy site from both ends after removing the plaque. Afterward, the unsutured middle third was isolated from the arterial lumen by placing a curved Satinsky clamp. And then, we opened all the clamped carotid arteries before finishing the suture. In technique 2, we sutured the arteriotomy site at the common carotid artery (CCA). We then placed a curved Satinsky clamp crossing from the sutured site to the carotid bifurcation, isolating the unsutured site at the internal carotid artery (ICA). After placing the Satinsky clamp, the CCA and external carotid artery (ECA) were opened to allow blood flow from CCA to ECA. By opening the ECA, ECA collateral flow via ECA-ICA anastomoses could help to reduce cerebral ischemia.
Results
: The modified suture methods can reduce the cerebral ischemia directly (technique 1) or via using collaterals (technique 2). The modified arteriotomy suture techniques are simple, safe, and applicable to almost all cases of CEA.
Conclusion
: Two modified arteriotomy suture techniques could reduce perioperative ischemic complications by reducing the cerebral ischemic time.
Figure
-
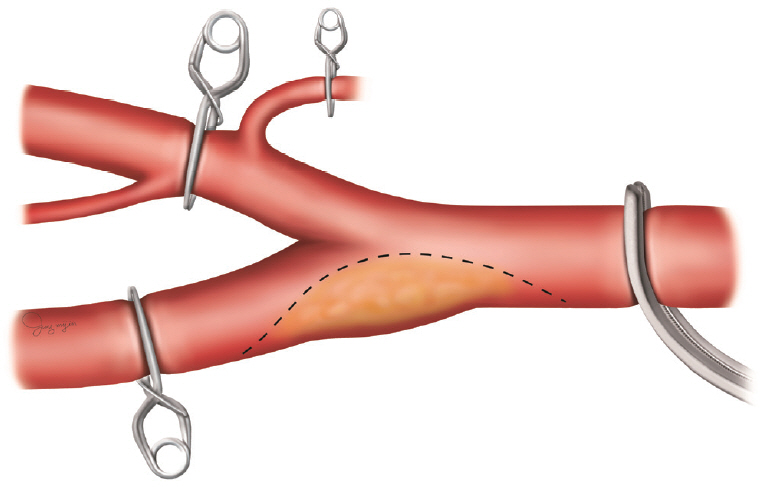
Fig. 1. In conventional carotid endarterectomy, the ICA, CCA, and ECA are clamped in that order. From incision on the carotid artery to closure of the arteriotomy, the entire process of endarterectomy is performed in the condition that the ICA, CCA, and ECA are clamped. After finishing the complete closure of the arteriotomy site, the ICA, ECA, and CCA are unclamped. ICA : internal carotid artery, CCA : common carotid artery, ECA : external carotid artery.

Fig. 2. A and B : Cerebral angiography revealed NASCET 55% stenosis in the left distal CCA including the ICA origin site. The lesion was accompanied by luminal irregularity (A : anteroposterior view, B : lateral view). C : The atheroma was an unstable plaque with ulceration. D : Applying a Satinsky clamp to isolated unsutured site from the carotid artery lumen. E : After applying a Satinsky clamp, the ECA, ICA, and CCA were opened before finishing the closure of the arteriotomy site. NASCET : The North American Symptomatic Carotid Endarterectomy Trial, CCA : common carotid artery, ICA : internal carotid artery, ECA : external carotid artery.

Fig. 3. A : Computed tomography angiography revealed severe stenosis of the left proximal cervical ICA (NASCET 80%) with calcification. B : Magnetic resonance angiography also demonstrated severe proximal ICA stenosis with ulceration. C : Intraoperative finding of unstable atheroma with ulceration. D : Applying a Satinsky clamp to isolate the unsutured site at the ICA from the CCA lumen. E : After applying a Satinsky clamp, the ECA and CCA were opened before finishing the complete suture of the arteriotomy site. ICA : internal carotid artery, NASCET : The North American Symptomatic Carotid Endarterectomy Trial, CCA : common carotid artery, ECA : external carotid artery.

Fig. 4. Suture technique 1. The key point of this method is opening the clamps early at the CCA, ICA, and ECA before finishing the complete closure of the arteriotomy, by placing a curved Satinsky clamp at the unsutured site. Black arrows indicate direct blood flow from CCA to ICA. To enable a smooth blood flow, the Satinsky clamp should be placed at the CCA. This method is more applicable in cases that the arteriotomy extends to the CCA. CCA : common carotid artery, ICA : internal carotid artery, ECA : external carotid artery.

Fig. 5. Suture technique 2. This method is using collateral blood flow via multiple anastomoses between the ICA and ECA. First, the arteriotomy at the CCA is sutured. After that, the unsutured site at the ICA is isolated using a curved Satinsky clamp. Afterward, the CCA and ECA are opened to enable blood flow from the CCA to the ECA. Black arrow indicates blood flow from CCA to ECA and dotted black arrow means collateral flow via ECA-ICA anastomoses. This method is easy to apply in cases where the plaque is located at the ICA side and the arteriotomy is not extended to the CCA. ICA : internal carotid artery, ECA : external carotid artery, CCA : common carotid artery.
Reference
-
References
1. Aburahma AF, Mousa AY, Stone PA. Shunting during carotid endarterectomy. J Vasc Surg. 54:1502–1510. 2011.
Article2. Barnett HJ, Taylor DW, Eliasziw M, Fox AJ, Ferguson GG, Haynes RB, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 339:1415–1425. 1998.
Article3. Boontje AH. Carotid endarterectomy without a temporary indwelling shunt: results and analysis of back pressure measurements. Cardiovasc Surg. 2:549–554. 1994.4. Hans SS, Catanescu I. Selective shunting for carotid endarterectomy in patients with recent stroke. J Vasc Surg. 61:915–919. 2015.
Article5. Jacobowitz GR, Rockman CB, Lamparello PJ, Adelman MA, Schanzer A, Woo D, et al. Causes of perioperative stroke after carotid endarterectomy: special considerations in symptomatic patients. Ann Vasc Surg. 15:19–24. 2001.
Article6. Lawrence PF, Alves JC, Jicha D, Bhirangi K, Dobrin PB. Incidence, timing, and causes of cerebral ischemia during carotid endarterectomy with regional anesthesia. J Vasc Surg. 27:329–334. discussion 335-337. 1998.
Article7. Liebeskind DS. Collateral circulation. Stroke. 34:2279–2284. 2003.
Article8. North American Symptomatic Carotid Endarterectomy Trial Collaborators, Barnett HJM, Taylor DW, Haynes RB, Sackett DL, Peerless SJ, et al. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 325:445–453. 1991.
Article9. Rerkasem K, Rothwell PM. Routine or selective carotid artery shunting for carotid endarterectomy (and different methods of monitoring in selective shunting). Cochrane Database Syst Rev. (4):CD000190. 2009.
Article10. Riles TS, Imparato AM, Jacobowitz GR, Lamparello PJ, Giangola G, Adelman MA, et al. The cause of perioperative stroke after carotid endarterectomy. J Vasc Surg. 19:206–214. discussion 215-216. 1994.
Article11. Samson RH, Showalter DP, Yunis JP. Routine carotid endarterectomy without a shunt, even in the presence of a contralateral occlusion. Cardiovasc Surg. 6:475–484. 1998.
Article12. Thompson JE. Complications of carotid endarterectomy and their prevention. World J Surg. 3:155–165. 1979.
Article13. van Laar PJ, van der Grond J, Bremmer JP, Klijn CJ, Hendrikse J. Assessment of the contribution of the external carotid artery to brain perfusion in patients with internal carotid artery occlusion. Stroke. 39:3003–3008. 2008.
Article14. Woodworth GF, McGirt MJ, Than KD, Huang J, Perler BA, Tamargo RJ. Selective versus routine intraoperative shunting during carotid endarterectomy: a multivariate outcome analysis. Neurosurgery. 61:1170–1176. discussion 1176-1177. 2007.15. Wu TY, Anderson NE, Barber PA. Neurological complications of carotid revascularisation. J Neurol Neurosurg Psychiatry. 83:543–550. 2012.
Article16. Young B, Moore WS, Robertson JT, Toole JF, Ernst CB, Cohen SN, et al. An analysis of perioperative surgical mortality and morbidity in the asymptomatic carotid atherosclerosis study. ACAS Investigators. Asymptomatic Carotid Atherosclerosis Study. Stroke. 27:2216–2224. 1996.
Article17. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 351:1379–1387. 1998.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carotid Endarterectomy: Techniques and Perioperative Management
- Cerebral Oxygen Saturation Monitoring during Carotid Endarterectomy: A case report
- Current Indications of Surgery and Endovascular Treatment in Ischemic Stroke
- Hyperacute hyperperfusion intracerebral hemorrhage complicating carotid endarterectomy: A case report
- Hypoxic-Ischemic Encephalopathy Following Carotid Endarterectomy
