Emergency exploratory laparotomy in a COVID-19 patient - A case report -
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, National Medical Center, Seoul, Korea
- KMID: 2508414
- DOI: http://doi.org/10.17085/apm.20041
Abstract
- Background
Surgeries in patients with coronavirus disease 2019 (COVID-19) put medical staff at a high risk of infection. We report the anesthetic management and infection control of a mechanically ventilated COVID-19 patient who underwent exploratory laparotomy for suspected duodenal ulcer perforation. Case: A 73-year-old man, mechanically ventilated for confirmed COVID-19, showed clinical and radiographic signs of a perforated duodenal ulcer, and he was transferred under sedation and intubation to a negative-pressure operating room. The operating and assistant staff wore personal protective equipment. High-efficiency particulate absorbing (HEPA) filters were inserted into the expiratory circuits of the anesthesia machine and portable ventilator. No participating staff contracted COVID-19, although the patient later died due to pneumonia.
Conclusions
This report can contribute to establishing clinical guidelines for the surgical management and operation room setting of COVID-19 patients.
Keyword
Figure
-

Fig. 1. Chest radiograph of the patient. (A) Chest radiograph of the patient showing ill-defined, hazy, and streaky density in both the lungs. (B) Chest radiograph showing subphrenic free air on both sides, homogenous increased density in the right costophrenic angle, and aggravated bilateral peripheral lung consolidation. (C) Chest radiograph showing increased pneumonic consolidation in both lung fields, especially that of the right lower lobe and pleural effusion right.

Fig. 2. Medical staff in preparation for surgery. The medical staff who were going to be inside the operating room each wore a fluid-resistant gown, PAPR, gloves, boots, and an apron. Staff wore double layers of gloves and boots. The surgeon and scrub nurse wore sterile gowns and surgical gloves on top of the PPE. The surgeons in the picture wore N95 masks inside the PAPR hoods. There is no strong evidence for the added protective effects of the concurrent use of N95 masks with PAPR [4]. Laminar flows from the ceiling toward the operating field (dotted arrow). A: anesthesiologist, S: surgeon, SN: scrub nurse, CN: circulating nurse, PAPR: powered air-purifying respirator, PPE: personal protective equipment.
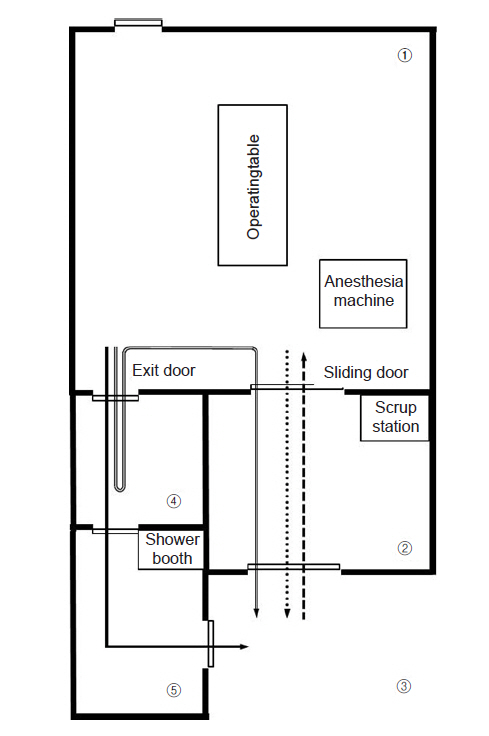
Fig. 3. Overall design of the negative-pressure operating room. Negative pressure is maintained only in (1) and (2), and when the doors of these rooms are opened, the negative pressure is temporarily lost. Square dotted arrow: pathway for entry of medical staff and patients; round dotted arrow: pathway for the patient’s exit, solid arrow: pathway for the exit of medical staff who do not participate in the patient transfer, overlaid arrow: pathway for medical staff who participate in the patient transfer after changing PPE that was worn during surgery. (1) main operating room, (2) anteroom, (3) waiting room, (4) doffing area, (5) buffer area. PPE: personal protective equipment.
Reference
-
1. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020; 323:1239–42.2. COVID-19 National Emergency Response Center; Epidemiology and Case Management Team; Korea Centers for Disease Control and Prevention. Early epidemiological and clinical characteristics of 28 cases of coronavirus disease in South Korea. Osong Public Health Res Perspect. 2020; 11:8–14.3. Wax RS, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anaesth. 2020; 67:568–76.4. Wong J, Goh QY, Tan Z, Lie SA, Tay YC, Ng SY, et al. Preparing for a COVID-19 pandemic: a review of operating room outbreak response measures in a large tertiary hospital in Singapore. Can J Anaesth. 2020; 67:732–45.5. Tompkins BM, Kerchberger JP. Special article: personal protective equipment for care of pandemic influenza patients: a training workshop for the powered air purifying respirator. Anesth Analg. 2010; 111:933–45.6. Søreide K, Thorsen K, Harrison EM, Bingener J, Møller MH, Ohene-Yeboah M, et al. Perforated peptic ulcer. Lancet. 2015; 386:1288–98.7. Ghekiere O, Lesnik A, Hoa D, Laffargue G, Uriot C, Taourel P. Value of computed tomography in the diagnosis of the cause of nontraumatic gastrointestinal tract perforation. J Comput Assist Tomogr. 2007; 31:169–76.8. Kim JY, Song JY, Yoon YK, Choi SH, Song YG, Kim SR, et al. Middle East respiratory syndrome infection control and prevention guideline for healthcare facilities. Infect Chemother. 2015; 47:278–302.9. Sehulster L, Chinn RY; CDC; HICPAC. Guidelines for environmental infection control in health-care facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR Recomm Rep. 2003; 52:1–42.10. Park J, Yoo SY, Ko JH, Lee SM, Chung YJ, Lee JH, et al. Infection prevention measures for surgical procedures during a Middle East respiratory syndrome outbreak in a tertiary care hospital in South Korea. Sci Rep. 2020; 10:325.11. Park MH, Kim HR, Choi DH, Sung JH, Kim JH. Emergency cesarean section in an epidemic of the Middle East respiratory syndrome: a case report. Korean J Anesthesiol. 2016; 69:287–91.12. Xia H, Zhao S, Wu Z, Luo H, Zhou C, Chen X. Emergency caesarean delivery in a patient with confirmed COVID-19 under spinal anaesthesia. Br J Anaesth. 2020; 124:e216–8.13. Chen R, Zhang Y, Huang L, Cheng BH, Xia ZY, Meng QT. Safety and efficacy of different anesthetic regimens for parturients with COVID-19 undergoing cesarean delivery: a case series of 17 patients. Can J Anaesth. 2020; 67:655–63.14. Liew MF, Siow WT, Yau YW, See KC. Safe patient transport for COVID-19. Crit Care. 2020; 24:94.15. van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020; 382:1564–7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Intestinal Ischemia in a Patient with COVID-19 Infection
- The impact of the COVID-19 pandemic on in-hospital mortality in patients admitted through the emergency department
- Intracranial Hypertension after COVID-19 Infection
- The Impact of COVID-19 on Dysphagia in a Steroid-Responsive Dermatomyositis Patient: A Case Report
- A Case Report of Tracheoesophageal Fistula Found during General Anesthesia for Emergency Exploratory Laparotomy
