Perioperative outcomes of interrupted anticoagulation in patients with non-valvular atrial fibrillation undergoing non-cardiac surgery
- Affiliations
-
- 1Department of Internal Medicine, Kyungpook National University Hospital, School of Medicine, Kyungpook National University, Daegu, Korea
- KMID: 2508178
- DOI: http://doi.org/10.12701/yujm.2020.00353
Abstract
- Background
This study aimed to investigate the incidences of and risk factors for perioperative events following anticoagulant discontinuation in patients with non-valvular atrial fibrillation (NVAF) undergoing non-cardiac surgery.
Methods
A total of 216 consecutive patients who underwent cardiac consultation for suspending perioperative anticoagulants were enrolled. A perioperative event was defined as a composite of thromboembolism and major bleeding.
Results
The mean anticoagulant discontinuation duration was 5.7 (±4.2) days and was significantly longer in the warfarin group (p<0.001). Four perioperative thromboembolic (1.85%; three strokes and one systemic embolization) and three major bleeding events (1.39%) were observed. The high CHA2DS2-VASc and HAS-BLED scores and a prolonged preoperative anticoagulant discontinuation duration (4.4±2.1 vs. 2.9±1.8 days; p=0.028) were associated with perioperative events, whereas the anticoagulant type (non-vitamin K antagonist oral anticoagulants or warfarin) was not. The best cut-off levels of the HAS-BLED and CHA2DS2-VASc scores were 3.5 and 2.5, respectively, and the preoperative anticoagulant discontinuation duration for predicting perioperative events was 2.5 days. Significant differences in the perioperative event rates were observed among the four risk groups categorized according to the sum of these values: risk 0, 0%; risk 1, 0%; risk 2, 5.9%; and risk 3, 50.0% (p<0.001). Multivariate logistic regression analysis showed that the HAS-BLED score was an independent predictor for perioperative events.
Conclusion
Thromboembolic events and major bleeding are not uncommon during perioperative anticoagulant discontinuation in patients with NVAF, and interrupted anticoagulation strategies are needed to minimize these.
Figure
-
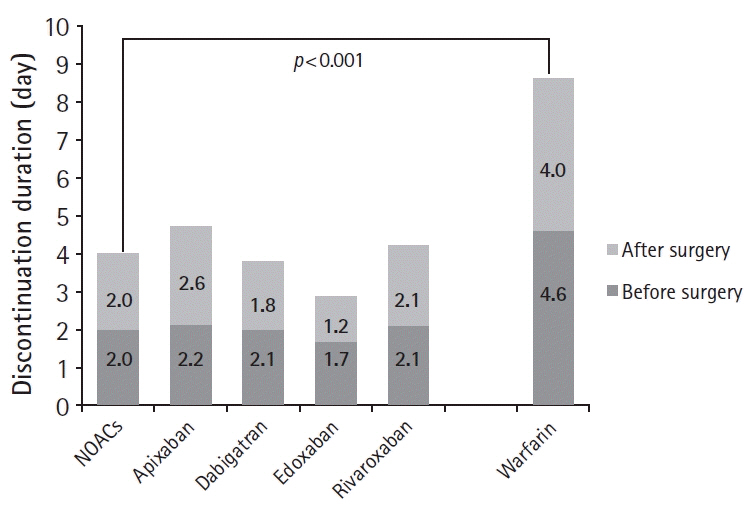
Fig. 1. Duration of perioperative anticoagulant discontinuation according to anticoagulant type (non-vitamin K antagonist oral anticoagulants [NOACs] vs. warfarin).
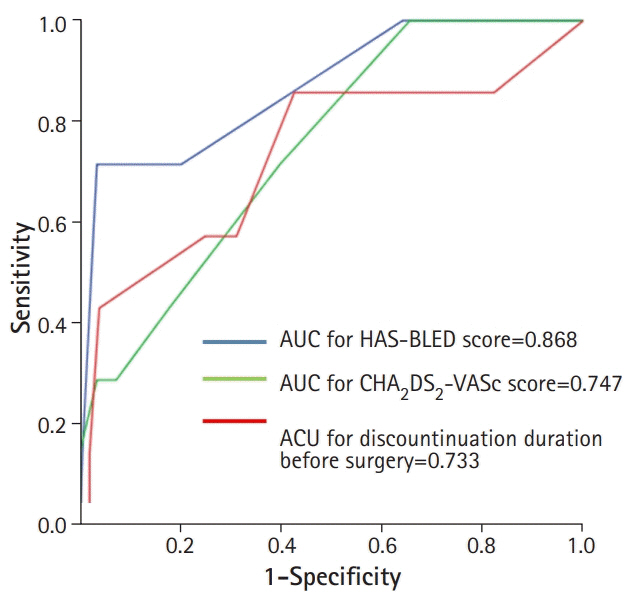
Fig. 2. Receiver operating characteristics curve analyses of the HAS-BLED and CHA2DS2VASc scores and duration of preoperative anticoagulant discontinuation for predicting perioperative events. AUC, area under the curve.
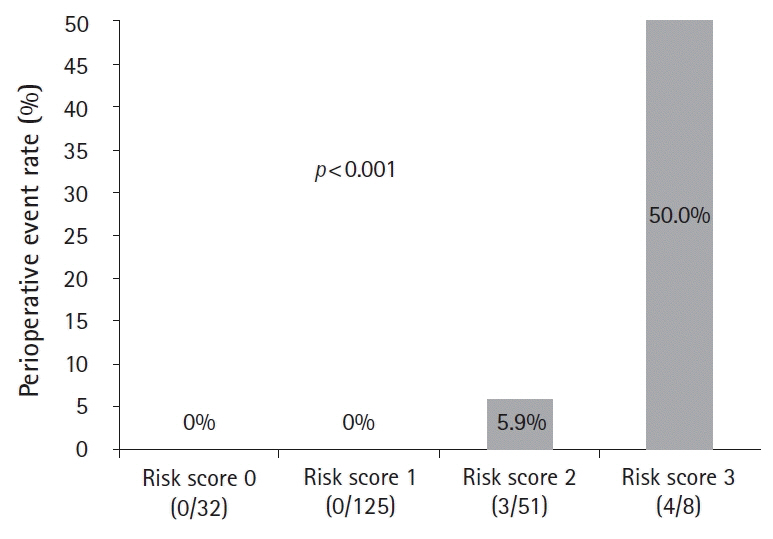
Fig. 3. Perioperative event rate categorized according to the cut-off levels of the HAS-BLED and CHA2DS2-VASc scores and duration of preoperative anticoagulant discontinuation. Significant differences in perioperative event rates are observed among the risk 0 (0%), 1 (0%), 2 (5.9%), and 3 (50.0%) groups (p<0.001). HAS-BLED score >3.5: 1, CHA2DS2-VASc >2.5: 1, discontinuation duration before surgery >2.5 days: 1.
Reference
-
References
1. Lip GY, Lim HS. Atrial fibrillation and stroke prevention. Lancet Neurol. 2007; 6:981–93.
Article2. Wolf PA, Mitchell JB, Baker CS, Kannel WB, D'Agostino RB. Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. 1998; 158:229–34.
Article3. Hughes M, Lip GY; Guideline Development Group; National Clinical Guideline for Management of Atrial Fibrillation in Primary and Secondary Care; National Institute for Health and Clinical Excellence. Stroke and thromboembolism in atrial fibrillation: a systematic review of stroke risk factors, risk stratification schema and cost effectiveness data. Thromb Haemost. 2008; 99:295–304.
Article4. Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001; 285:2370–5.
Article5. Hylek EM, Go AS, Chang Y, Jensvold NG, Henault LE, Selby JV, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med. 2003; 349:1019–26.
Article6. Rivera-Caravaca JM, Roldán V, Esteve-Pastor MA, Valdés M, Vicente V, Lip GY, et al. Cessation of oral anticoagulation is an important risk factor for stroke and mortality in atrial fibrillation patients. Thromb Haemost. 2017; 117:1448–54.
Article7. Heidbuchel H, Verhamme P, Alings M, Antz M, Diener HC, Hacke W, et al. Updated European Heart Rhythm Association practical guide on the use of non-vitamin-K antagonist anticoagulants in patients with non-valvular atrial fibrillation: executive summary. Eur Heart J. 2017; 38:2137–49.
Article8. Wysokinski WE, McBane RD, Daniels PR, Litin SC, Hodge DO, Dowling NF, et al. Periprocedural anticoagulation management of patients with nonvalvular atrial fibrillation. Mayo Clin Proc. 2008; 83:639–45.
Article9. Doherty JU, Gluckman TJ, Hucker WJ, Januzzi JL Jr, Ortel TL, Saxonhouse SJ, et al. 2017 ACC expert consensus decision pathway for periprocedural management of anticoagulation in patients with nonvalvular atrial fibrillation: a report of the American College of Cardiology Clinical Expert Consensus Document Task Force. J Am Coll Cardiol. 2017; 69:871–98.10. Larsen TB, Skjøth F, Nielsen PB, Kjældgaard JN, Lip GY. Comparative effectiveness and safety of non-vitamin K antagonist oral anticoagulants and warfarin in patients with atrial fibrillation: propensity weighted nationwide cohort study. BMJ. 2016; 353:i3189.
Article11. Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. 2018; 39:1330–93.
Article12. Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014; 383:955–62.
Article13. Birman-Deych E, Radford MJ, Nilasena DS, Gage BF. Use and effectiveness of warfarin in Medicare beneficiaries with atrial fibrillation. Stroke. 2006; 37:1070–4.
Article14. Wallentin L, Yusuf S, Ezekowitz MD, Alings M, Flather M, Franzosi MG, et al. Efficacy and safety of dabigatran compared with warfarin at different levels of international normalised ratio control for stroke prevention in atrial fibrillation: an analysis of the RE-LY trial. Lancet. 2010; 376:975–83.
Article15. Lopes RD, Alexander JH, Al-Khatib SM, Ansell J, Diaz R, Easton JD, et al. Apixaban for reduction in stroke and other ThromboemboLic events in atrial fibrillation (ARISTOTLE) trial: design and rationale. Am Heart J. 2010; 159:331–9.
Article16. Connolly SJ, Ezekowitz MD, Yusuf S, Reilly PA, Wallentin L; Randomized Evaluation of Long-Term Anticoagulation Therapy Investigators. Newly identified events in the RE-LY trial. N Engl J Med. 2010; 363:1875–6.
Article17. Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013; 369:2093–104.
Article18. Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011; 365:981–92.19. Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011; 365:883–91.
Article20. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009; 361:1139–51.
Article21. Levy JH. Discontinuation and management of direct-acting anticoagulants for emergency procedures. Am J Med. 2016; 129(11 Suppl):S47–53.
Article22. Kornej J, Potpara T, Lip GY. Anticoagulation management in nonvalvular atrial fibrillation: current and future directions. Pol Arch Med Wewn. 2013; 123:623–34.
Article23. Kearon C, Hirsh J. Management of anticoagulation before and after elective surgery. N Engl J Med. 1997; 336:1506–11.
Article24. Garcia DA, Regan S, Henault LE, Upadhyay A, Baker J, Othman M, et al. Risk of thromboembolism with short-term interruption of warfarin therapy. Arch Intern Med. 2008; 168:63–9.
Article25. Raval AN, Cigarroa JE, Chung MK, Diaz-Sandoval LJ, Diercks D, Piccini JP, et al. Management of patients on non-vitamin K antagonist oral anticoagulants in the acute care and periprocedural setting: a scientific statement from the American Heart Association. Circulation. 2017; 135:e604–33.
Article26. Douketis JD, Spyropoulos AC, Duncan J, Carrier M, Le Gal G, Tafur AJ, et al. Perioperative management of patients with atrial fibrillation receiving a direct oral anticoagulant. JAMA Intern Med. 2019; 179:1469–78.
Article27. Siegal D, Yudin J, Kaatz S, Douketis JD, Lim W, Spyropoulos AC, et al. Periprocedural heparin bridging in patients receiving vitamin K antagonists: systematic review and meta-analysis of bleeding and thromboembolic rates. Circulation. 2012; 126:1630–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Anticoagulation in Atrial Fibrillation
- Cardioembolic Stroke in Atrial Fibrillation-Rationale for Preventive Closure of the Left Atrial Appendage
- How and When to Screen for Atrial Fibrillation after Stroke: Insights from Insertable Cardiac Monitoring Devices
- Clinical Characteristics and Management in Elderly Patients with Atrial Fibrillation
- Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation
