Current National and International Guidelines for the Management of Male Hypogonadism: Helping Clinicians to Navigate Variation in Diagnostic Criteria and Treatment Recommendations
- Affiliations
-
- 1Department of Endocrinology, Newcastle Upon Tyne Hospitals NHS Foundation Trust, UK
- 2Translational & Clinical Research Institute, Newcastle University, Newcastle-upon-Tyne, UK
- KMID: 2508001
- DOI: http://doi.org/10.3803/EnM.2020.760
Abstract
- Male hypogonadism—rebadged by some as testosterone deficiency syndrome—is a clinical and biochemical diagnosis of increasing worldwide interest. Organic male hypogonadism—usually permanent—is well-established, but aging men may also exhibit lower serum testosterone levels; principally due to burden of extra-gonadal comorbidities such as obesity, diabetes and metabolic syndrome, but with an underlying intact hypothalamo-pituitary-testicular (HPT) axis capable of springing back into operation once comorbidities are addressed. Despite encouraging observational data and plausible theoretical underpinning, evidence for efficacy and safety of testosterone in this “aging” group of men is lacking; addressing comorbid illnesses remains the key priority instead. Nevertheless, in recent years, accumulation of misleading information online has triggered a global tsunami of testosterone prescriptions. Despite this, many men with organic hypogonadism remain undiagnosed or untreated; many more face a diagnostic odyssey before achieving care by the appropriate specialist. As testosterone therapy is not without risk several clinical practice guidelines have been published specialist societies to guide physicians on best practice. However, these are heterogeneous in key areas, reflecting divergent approaches to the same evidence basis. Herein, we navigate the major clinical practice guidelines on male hypogonadism and test their respective recommendations against current best evidence.
Figure
-
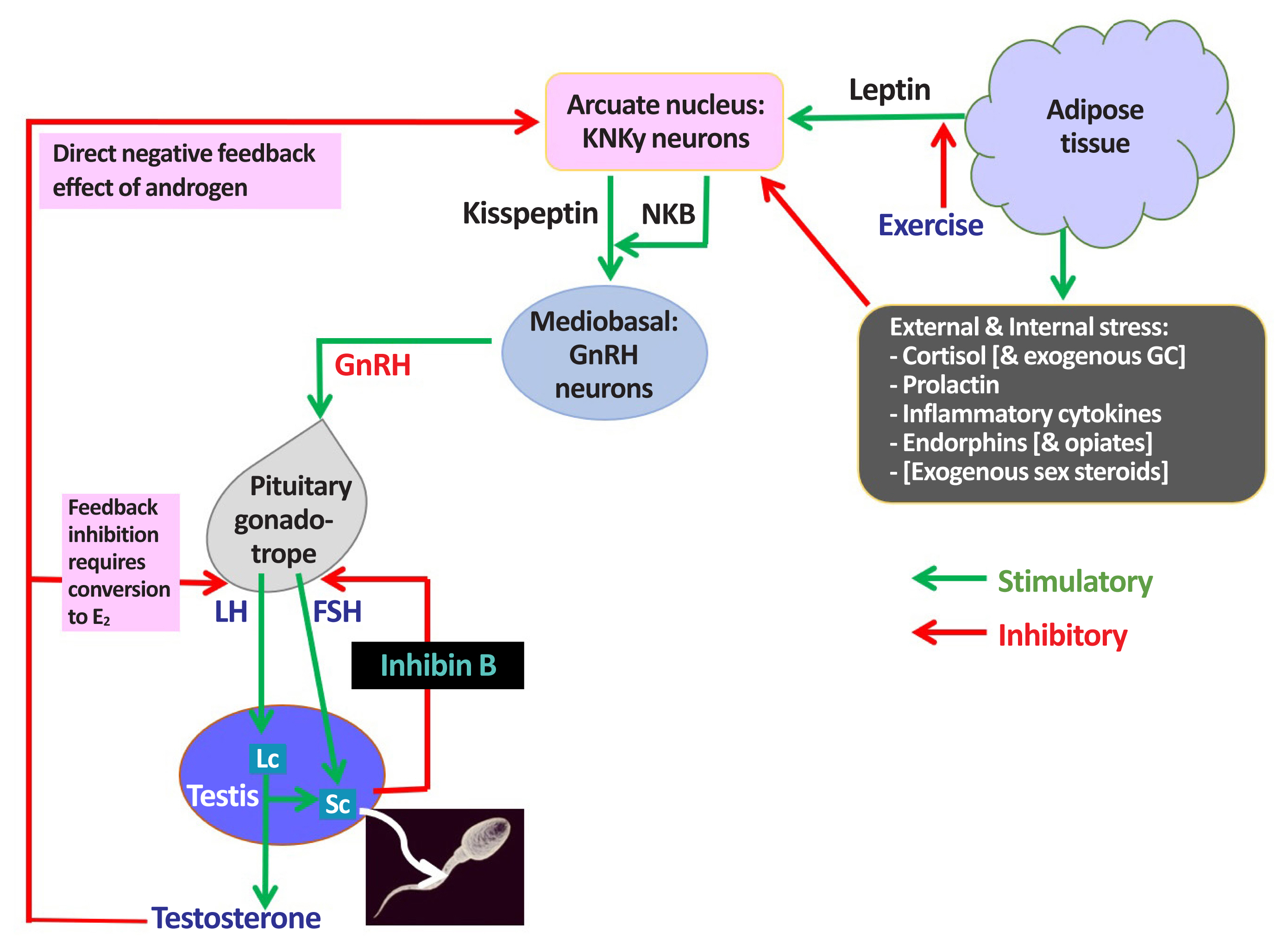
Fig. 1 Male hypothalamic-pituitary-gonadal (HPG) axis: homeostatic & environmental inputs: endocrine & paracrine actions of testosterone. KNDy, kisspeptin, neurokinin B, and dynorphin; NKB, neurokinin B; GC, glucocorticosteroid; GnRH, gonadotropin-releasing hormone; E2, oestradiol; FSH, follicle-stimulating hormone; LH, luteinizing hormone; Lc, Leydig cell; Sc, Sertoli cell.
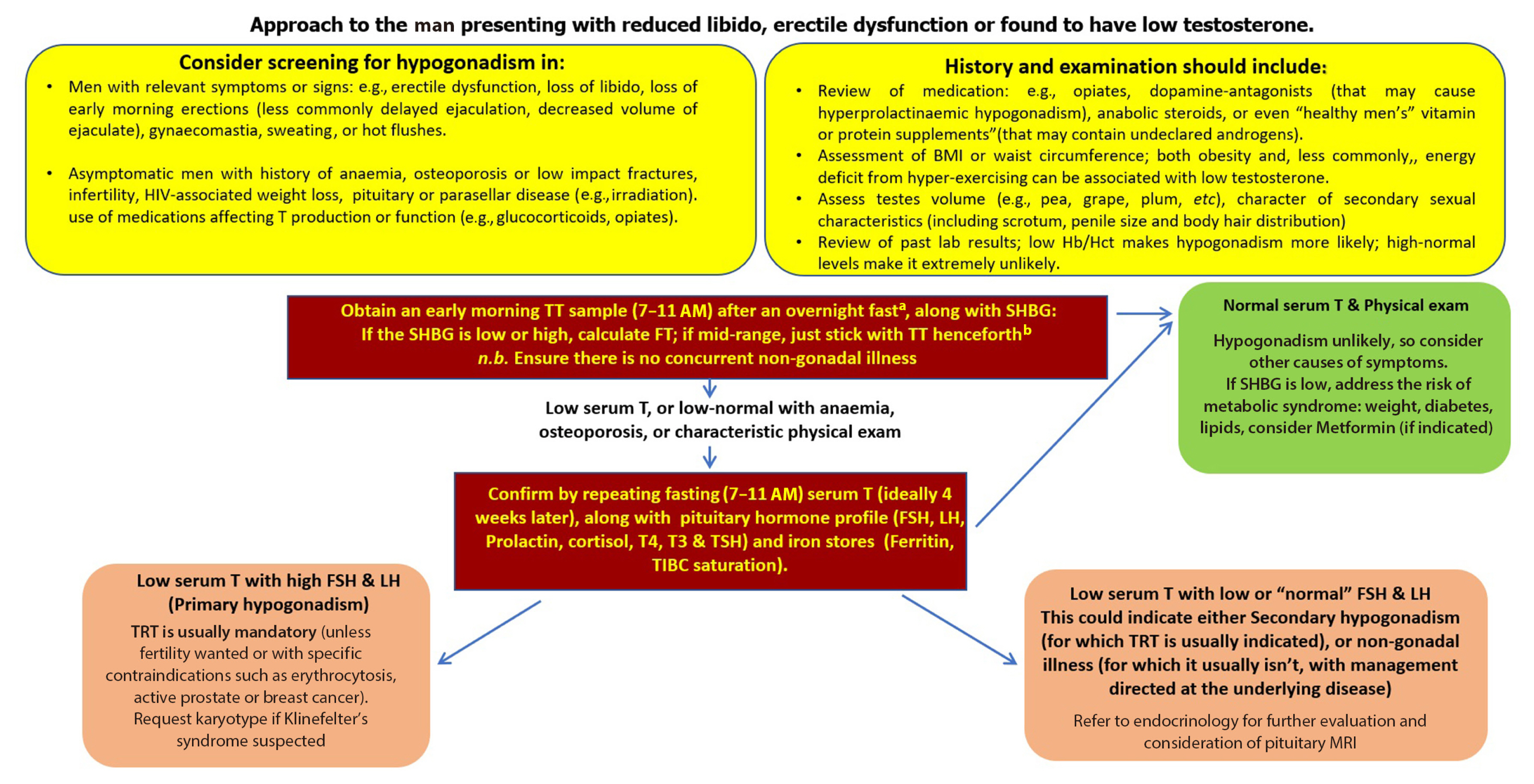
Fig. 2 An approach to low testosterone levels in primary care. HIV, human immunodeficiency virus; BMI, body mass index; Hb/Hct, hemoglobin/hematocrit; TT, total testosterone; SHBG, sex hormone binding globulin; FSH, follicle-stimulating hormone; LH, luteinizing hormone; T4, thyroxine; T3, triiodothyronine; TSH, thyroid stimulating hormone; TIBC, total iron binding capacity; TRT, testosterone replacement therapy; MRI, magnetic resonance imaging. aConsider your local laboratory reference range as measurements can be variable from laboratory to another, in shift workers measure within 3 hours of waking; bwww.issam.ch/freetesto.htm.
Reference
-
1. Bhasin S, Brito JP, Cunningham GR, Hayes FJ, Hodis HN, Matsumoto AM, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018; 103:1715–44.
Article2. Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR; Baltimore Longitudinal Study of Aging. Longitudinal effects of aging on serum total and free testosterone levels in healthy men. Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001; 86:724–31.3. Araujo AB, Esche GR, Kupelian V, O’Donnell AB, Travison TG, Williams RE, et al. Prevalence of symptomatic androgen deficiency in men. J Clin Endocrinol Metab. 2007; 92:4241–7.
Article4. Llahana S, Follin C, Yedinak C, Grossman AB. Advanced practice in endocrinology nursing. Cham: Springer;2019. Chapter, Classification of hypothalamic-pituitary-gonadal (HPG) axis endocrine disorders. p. 853–70.5. Kelly DM, Jones TH. Testosterone and obesity. Obes Rev. 2015; 16:581–606.
Article6. Pye SR, Huhtaniemi IT, Finn JD, Lee DM, O’Neill TW, Tajar A, et al. Late-onset hypogonadism and mortality in aging men. J Clin Endocrinol Metab. 2014; 99:1357–66.
Article7. Dong JY, Zhang YH, Qin LQ. Erectile dysfunction and risk of cardiovascular disease: meta-analysis of prospective cohort studies. J Am Coll Cardiol. 2011; 58:1378–85.8. Wu FC, Tajar A, Pye SR, Silman AJ, Finn JD, O’Neill TW, et al. Hypothalamic-pituitary-testicular axis disruptions in older men are differentially linked to age and modifiable risk factors: the European Male Aging Study. J Clin Endocrinol Metab. 2008; 93:2737–45.
Article9. Turner HE, Wass JA. Gonadal function in men with chronic illness. Clin Endocrinol (Oxf). 1997; 47:379–403.
Article10. Dwyer AA, Quinton R. The metabolic syndrome in central hypogonadotrophic hypogonadism. Front Horm Res. 2018; 49:156–69.
Article11. Cheng J, Han B, Li Q, Xia F, Zhai H, Wang N, et al. Testosterone: relationships with metabolic disorders in men-an observational study from SPECT-China. Int J Endocrinol. 2017; 2017:4547658.
Article12. Sartorius G, Spasevska S, Idan A, Turner L, Forbes E, Zamojska A, et al. Serum testosterone, dihydrotestosterone and estradiol concentrations in older men self-reporting very good health: the healthy man study. Clin Endocrinol (Oxf). 2012; 77:755–63.
Article13. Society for Endocrinology. Society for endocrinology position statement on male hypogonadism and ageing [Internet]. Bristol: Society for Endocrinology;2018. [cited 2020 Aug 4]. Available from: https://www.endocrinology.org/media/2710/male-hypogonadism-and-ageing-2018.pdf .14. Bojesen A, Kristensen K, Birkebaek NH, Fedder J, Mosekilde L, Bennett P, et al. The metabolic syndrome is frequent in Klinefelter’s syndrome and is associated with abdominal obesity and hypogonadism. Diabetes Care. 2006; 29:1591–8.
Article15. Dahlqvist JR, Vissing J. Diabetes in myotonic dystrophy. Front Diabetes. 2017; 25:182–7.
Article16. Baillargeon J, Urban RJ, Ottenbacher KJ, Pierson KS, Goodwin JS. Trends in androgen prescribing in the United States, 2001 to 2011. JAMA Intern Med. 2013; 173:1465–6.
Article17. Layton JB, Li D, Meier CR, Sharpless JL, Sturmer T, Jick SS, et al. Testosterone lab testing and initiation in the United Kingdom and the United States, 2000 to 2011. J Clin Endocrinol Metab. 2014; 99:835–42.
Article18. Gan EH, Pattman S, Pearce SHS, Quinton R. A UK epidemic of testosterone prescribing, 2001–2010. Clin Endocrinol (Oxf). 2013; 79:564–70.
Article19. Handelsman DJ. Trends and regional differences in testosterone prescribing in Australia, 1991–2001. Med J Aust. 2004; 181:419–22.
Article20. Karavolos S, Reynolds M, Panagiotopoulou N, McEleny K, Scally M, Quinton R. Male central hypogonadism secondary to exogenous androgens: a review of the drugs and protocols highlighted by the online community of users for prevention and/or mitigation of adverse effects. Clin Endocrinol (Oxf). 2015; 82:624–32.
Article21. Al-Sharefi A, Wilkes S, Jayasena CN, Quinton R. How to manage low testosterone level in men: a guide for primary care. Br J Gen Pract. 2020; 70:364–5.
Article22. Calof OM, Singh AB, Lee ML, Kenny AM, Urban RJ, Tenover JL, et al. Adverse events associated with testosterone replacement in middle-aged and older men: a meta-analysis of randomized, placebo-controlled trials. J Gerontol A Biol Sci Med Sci. 2005; 60:1451–7.
Article23. Budoff MJ, Ellenberg SS, Lewis CE, Mohler ER 3rd, Wenger NK, Bhasin S, et al. Testosterone treatment and coronary artery plaque volume in older men with low testosterone. JAMA. 2017; 317:708–16.
Article24. Dean JD, McMahon CG, Guay AT, Morgentaler A, Althof SE, Becher EF, et al. The International Society for Sexual Medicine’s process of care for the assessment and management of testosterone deficiency in adult men. J Sex Med. 2015; 12:1660–86.
Article25. Hackett G, Kirby M, Edwards D, Jones TH, Wylie K, Ossei-Gerning N, et al. British Society for Sexual Medicine guidelines on adult testosterone deficiency, with statements for UK practice. J Sex Med. 2017; 14:1504–23.
Article26. Morales A, Bebb RA, Manjoo P, Assimakopoulos P, Axler J, Collier C, et al. Diagnosis and management of testosterone deficiency syndrome in men: clinical practice guideline. CMAJ. 2015; 187:1369–77.
Article27. Mulhall JP, Trost LW, Brannigan RE, Kurtz EG, Redmon JB, Chiles KA, et al. Evaluation and management of testosterone deficiency: AUA guideline. J Urol. 2018; 200:423–32.
Article28. Dohle GR, Arver S, Bettocchi C, Jones TH, Kliesch S. Male hypogonadism [Internet]. Arnhem: European Association of Urology;c2020. [cited 2020 Aug 4]. Available from: https://uroweb.org/guideline/male-hypogonadism .29. Yeap BB, Grossmann M, McLachlan RI, Handelsman DJ, Wittert GA, Conway AJ, et al. Endocrine Society of Australia position statement on male hypogonadism (part 1): assessment and indications for testosterone therapy. Med J Aust. 2016; 205:173–8.
Article30. Yeap BB, Grossmann M, McLachlan RI, Handelsman DJ, Wittert GA, Conway AJ, et al. Endocrine Society of Australia position statement on male hypogonadism (part 2): treatment and therapeutic considerations. Med J Aust. 2016; 205:228–31.
Article31. Qaseem A, Horwitch CA, Vijan S, Etxeandia-Ikobaltzeta I, Kansagara D; Clinical Guidelines Committee of the American College of Physicians. Testosterone treatment in adult men with age-related low testosterone: a clinical guideline from the American College of Physicians. Ann Intern Med. 2020; 172:126–33.
Article32. Hiort O, Holterhus PM, Horter T, Schulze W, Kremke B, Bals-Pratsch M, et al. Significance of mutations in the androgen receptor gene in males with idiopathic infertility. J Clin Endocrinol Metab. 2000; 85:2810–5.
Article33. Leonard JM, Bremner WJ, Capell PT, Paulsen CA. Male hypogonadism: Klinefelter and Reifenstein syndromes. Birth Defects Orig Artic Ser. 1975; 11:17–22.34. Ly LP, Sartorius G, Hull L, Leung A, Swerdloff RS, Wang C, et al. Accuracy of calculated free testosterone formulae in men. Clin Endocrinol (Oxf). 2010; 73:382–8.35. Paller CJ, Shiels MS, Rohrmann S, Basaria S, Rifai N, Nelson W, et al. Relationship of sex steroid hormones with bone mineral density (BMD) in a nationally representative sample of men. Clin Endocrinol (Oxf). 2009; 70:26–34.
Article36. Antonio L, Wu FC, O’Neill TW, Pye SR, Ahern TB, Laurent MR, et al. Low free testosterone is associated with hypogonadal signs and symptoms in men with normal total testosterone. J Clin Endocrinol Metab. 2016; 101:2647–57.
Article37. Woods DR, Hill NE, Neely RDG, Talks KL, Heggie A, Quinton R. Hematopoiesis shows closer correlation with calculated free testosterone in men than total testosterone. J Applied Lab Med. 2017; 4:441–4.
Article38. Cohen PG. The hypogonadal-obesity cycle: role of aromatase in modulating the testosterone-estradiol shunt: a major factor in the genesis of morbid obesity. Med Hypotheses. 1999; 52:49–51.
Article39. Practice Update ADA 2020: Testosterone plus lifestyle program reduced risk of type 2 diabetes in overweight and obese men [Internet]. Amsterdam: Elsevier;c2020. [cited 2020 Aug 4]. Available from: https://www.practiceupdate.com/content/ada-2020-testosterone-plus-lifestyle-program-reduced-risk-of-type-2-diabetes-in-overweight-and-obese-men/102636 .40. Snyder PJ, Bhasin S, Cunningham GR, Matsumoto AM, Stephens-Shields AJ, Cauley JA, et al. Lessons from the testosterone trials. Endocr Rev. 2018; 39:369–86.
Article41. Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, et al. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2010; 95:2536–59.
Article42. Dalvi M, Walker BR, Strachan MW, Zammitt NN, Gibb FW. The prevalence of structural pituitary abnormalities by MRI scanning in men presenting with isolated hypogonadotrophic hypogonadism. Clin Endocrinol (Oxf). 2016; 84:858–61.
Article43. El Osta R, Grandpre N, Monnin N, Hubert J, Koscinski I. Hypogonadotropic hypogonadism in men with hereditary hemochromatosis. Basic Clin Androl. 2017; 27:13.
Article44. Raju K, Venkataramappa SM. Primary hemochromatosis presenting as type 2 diabetes mellitus: a case report with review of literature. Int J Appl Basic Med Res. 2018; 8:57–60.
Article45. Angelopoulos NG, Goula A, Dimitriou E, Tolis G. Reversibility of hypogonadotropic hypogonadism in a patient with the juvenile form of hemochromatosis. Fertil Steril. 2005; 84:1744.
Article46. Gama R, Smith MJ, Wright J, Marks V. Hypopituitarism in primary haemochromatosis; recovery after iron depletion. Postgrad Med J. 1995; 71:297–8.
Article47. McDermott JH, Walsh CH. Hypogonadism in hereditary hemochromatosis. J Clin Endocrinol Metab. 2005; 90:2451–5.
Article48. National Cancer Institute. Hormone therapy for prostate cancer [Internet]. Bethesda: NIH;2020. [cited 2020 Aug 4]. Available from: https://www.cancer.gov/types/prostate/prostate-hormone-therapy-fact-sheet#:~:text=For%20men%20with%20intermediate%2Drisk,given%20for%2018%E2%-80%9324%20months .49. Nishikawa E, Jia S, Dharamshi C, Charron V, Lock M. Prostate cancer, gender identity, and testosterone replacement therapy in klinefelter syndrome: a case report and literature review. Cureus. 2019; 11:e4630.
Article50. Khoo TK. Adverse events associated with testosterone administration. N Engl J Med. 2010; 363:1865–6.
Article51. Warny M, Helby J, Birgens HS, Bojesen SE, Nordestgaard BG. Arterial and venous thrombosis by high platelet count and high hematocrit: 108 521 individuals from the Copenhagen General Population Study. J Thromb Haemost. 2019; 17:1898–911.
Article52. Emamian M, Hasanian SM, Tayefi M, Bijari M, Movahedian Far F, Shafiee M, et al. Association of hematocrit with blood pressure and hypertension. J Clin Lab Anal. 2017; 31:e22124.
Article53. Muensterman ET, Jaynes HA, Sowinski KM, Overholser BR, Shen C, Kovacs RJ, et al. Effect of transdermal testosterone and oral progesterone on drug-induced qt interval lengthening in older men: a randomized, double-blind, placebo-controlled crossover-design study. Circulation. 2019; 140:1127–9.
Article54. Gravholt CH, Chang S, Wallentin M, Fedder J, Moore P, Skakkebaek A. Klinefelter syndrome: integrating genetics, neuropsychology, and endocrinology. Endocr Rev. 2018; 39:389–423.
Article55. Quinton R, Tomlinson J. Male hypogonadism and ageing: rejuvenating the guidance. Endocrinologist. 2019; 131: https://www.endocrinology.org/endocrinologist/131-spring19/society-news/male-hypogonadism-and-ageing-rejuvenating-the-guidance/ .56. Anawalt BD. Diagnosis and management of anabolic androgenic steroid use. J Clin Endocrinol Metab. 2019; 104:2490–500.
Article57. Zitzmann M, Faber S, Nieschlag E. Association of specific symptoms and metabolic risks with serum testosterone in older men. J Clin Endocrinol Metab. 2006; 91:4335–43.
Article58. Kwong JCC, Krakowsky Y, Grober E. Testosterone deficiency: a review and comparison of current guidelines. J Sex Med. 2019; 16:812–20.
Article59. Wu FC, Tajar A, Beynon JM, Pye SR, Silman AJ, Finn JD, et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N Engl J Med. 2010; 363:123–35.
Article60. Travison TG, Vesper HW, Orwoll E, Wu F, Kaufman JM, Wang Y, et al. Harmonized reference ranges for circulating testosterone levels in men of four cohort studies in the United States and Europe. J Clin Endocrinol Metab. 2017; 102:1161–73.
Article61. Boehm U, Bouloux PM, Dattani MT, de Roux N, Dode C, Dunkel L, et al. Expert consensus document: European Consensus Statement on congenital hypogonadotropic hypogonadism: pathogenesis, diagnosis and treatment. Nat Rev Endocrinol. 2015; 11:547–64.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Manual of 2008 ISA, ISSAM, EAU, EAA and ASA Recommendations: Investigation, Treatment and Monitoring of Late-onset Hypogonadism in Males
- Diagnosis and Treatment of Sexual Dysfunctions in Late-Onset Hypogonadism
- Monitoring Ethambutol-Induced Optic Neuropathy in Tuberculosis Treatment: A Systematic Review of Guidelines and Recommendations
- Management of Chronic Hepatitis B with Nucleoside or Nucleotide Analogues: A Review of Current Guidelines
- 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma
