Retroduodenal resection of the extrahepatic common bile duct with in situ re-implantation of the main pancreatic duct:A report of two cases
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2505354
- DOI: http://doi.org/10.14701/ahbps.2020.24.3.373
Abstract
- Resection of the whole distal common bile duct (CBD) with in situ re-implantation of the main pancreatic duct can be a surgical option to avoid pancreaticoduodenectomy. in this study, we present two cases of cholangiocarcinomas with diffuse involvement of the extrahepatic CBD that was resected through a retroduodenal approach and re-implantation of the main pancreatic duct. The first case was a 70-year-old male patient with intraductal papillary neoplasm with invasive cholangiocarcinoma. He underwent retroduodenal resection of the whole CBD and in situ re-implantation of the main pancreatic duct. He was disease-free for 8 years, but tumor recurrence occurred at the hepaticojejunostomy site. This patient is currently undergoing chemoradiation therapy for treatment of recurrent lesions. The second case was a 71-year-old male patient with diffuse cholangiocarcinoma involving the whole extrahepatic CBD. He underwent medial sectionectomy, retroduodenal resection of the whole CBD and in situ re-implantation of the main pancreatic duct. He received postoperative chemoradiation therapy. He was disease-free for 3 years, but tumor recurrence occurred at the hepaticojejunostomy site. He passed away 4 years and 6 months after surgery. In conclusion, complete resection of the extrahepatic CBD through a retroduodenal approach with in situ re-implantation of the main pancreatic duct is feasible and less invasive than PD. Therefore, the proposed less-invasive approach can be an alternative procedure in selected patients requiring complete resection of the distal CBD.
Keyword
Figure
-
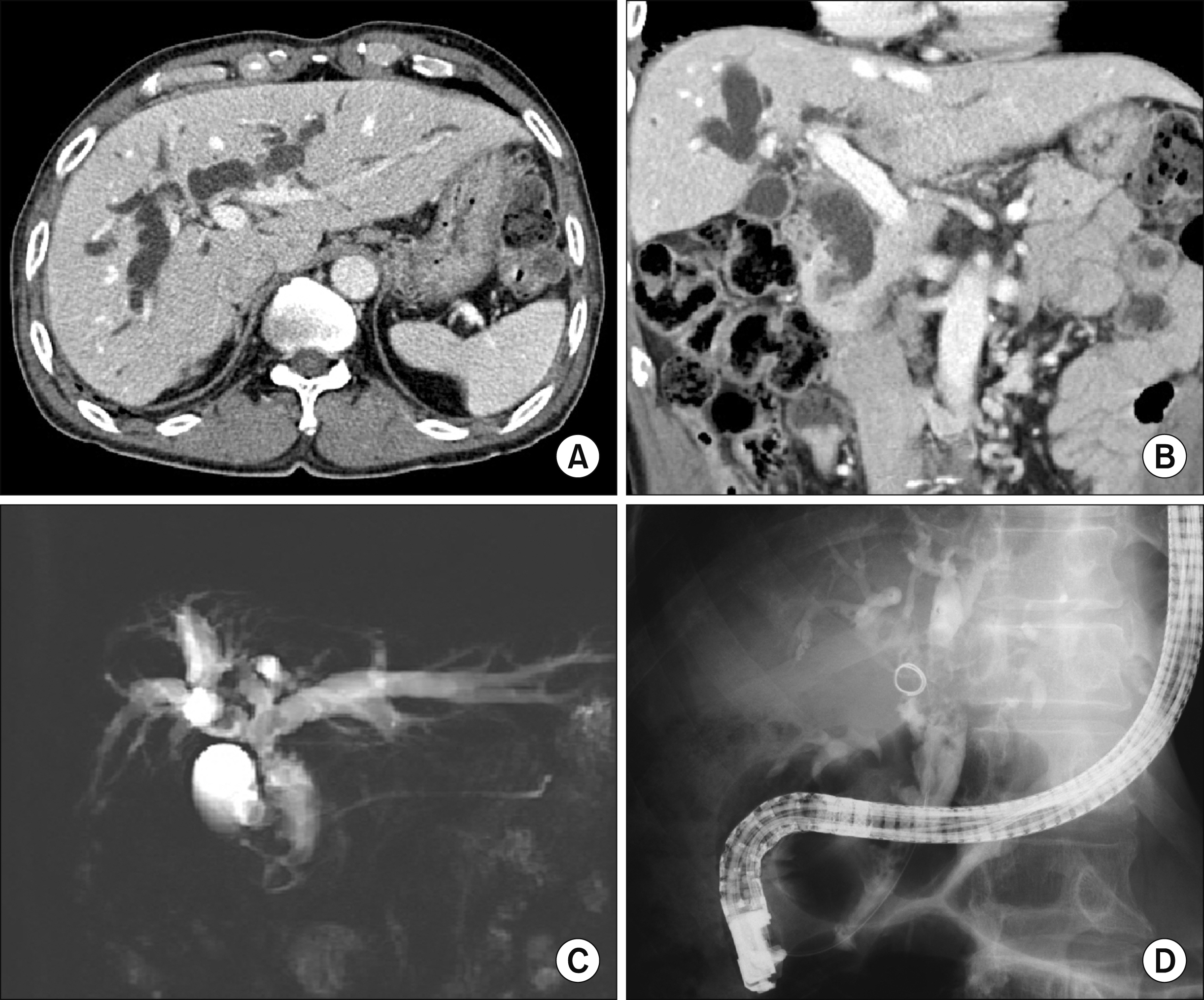
Fig. 1 Initial preoperative radiologic findings of Case 1. (A and B) Computed tomography scan shows multiple intraductal papillary masses in the extrahepatic bile duct and right intrahepatic duct with diffuse bile duct dilatation. (C) Magnetic resonance cholangiopancreatography shows intrahepatic duct stones and multiple intraductal lesions. (D) Endoscopic retrograde cholangiopancreatography with biopsy was performed.
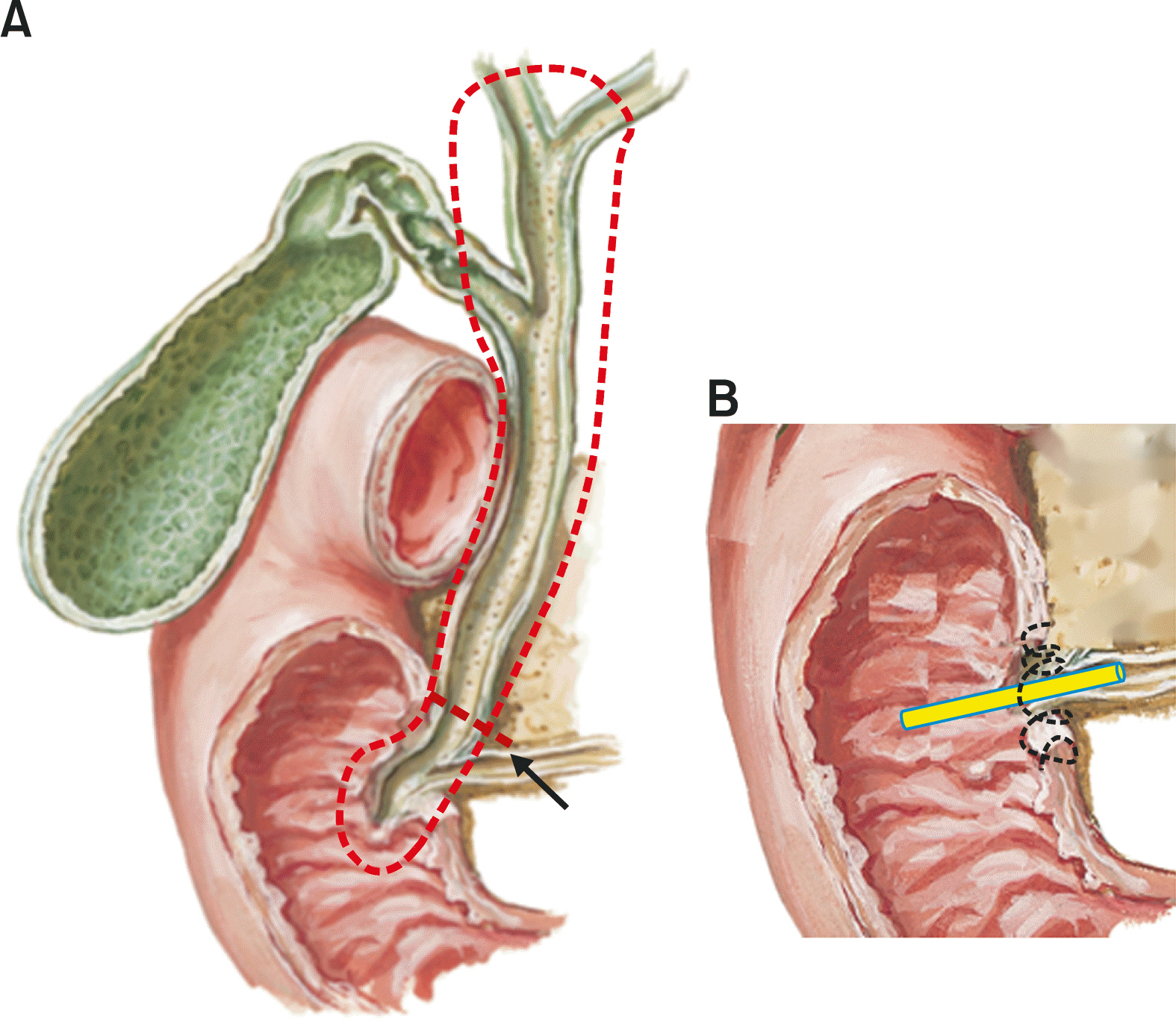
Fig. 2 Schematic illustration of the retroduodenal resection of the whole extrahepatic bile duct (A) and in situ re-implantation of the main pancreatic duct (B) in Case 1. The dotted line and arrow denote the extent of bile duct resection and initial transection line, respectively (A). The tube indicates the internal pancreatic stent (B).
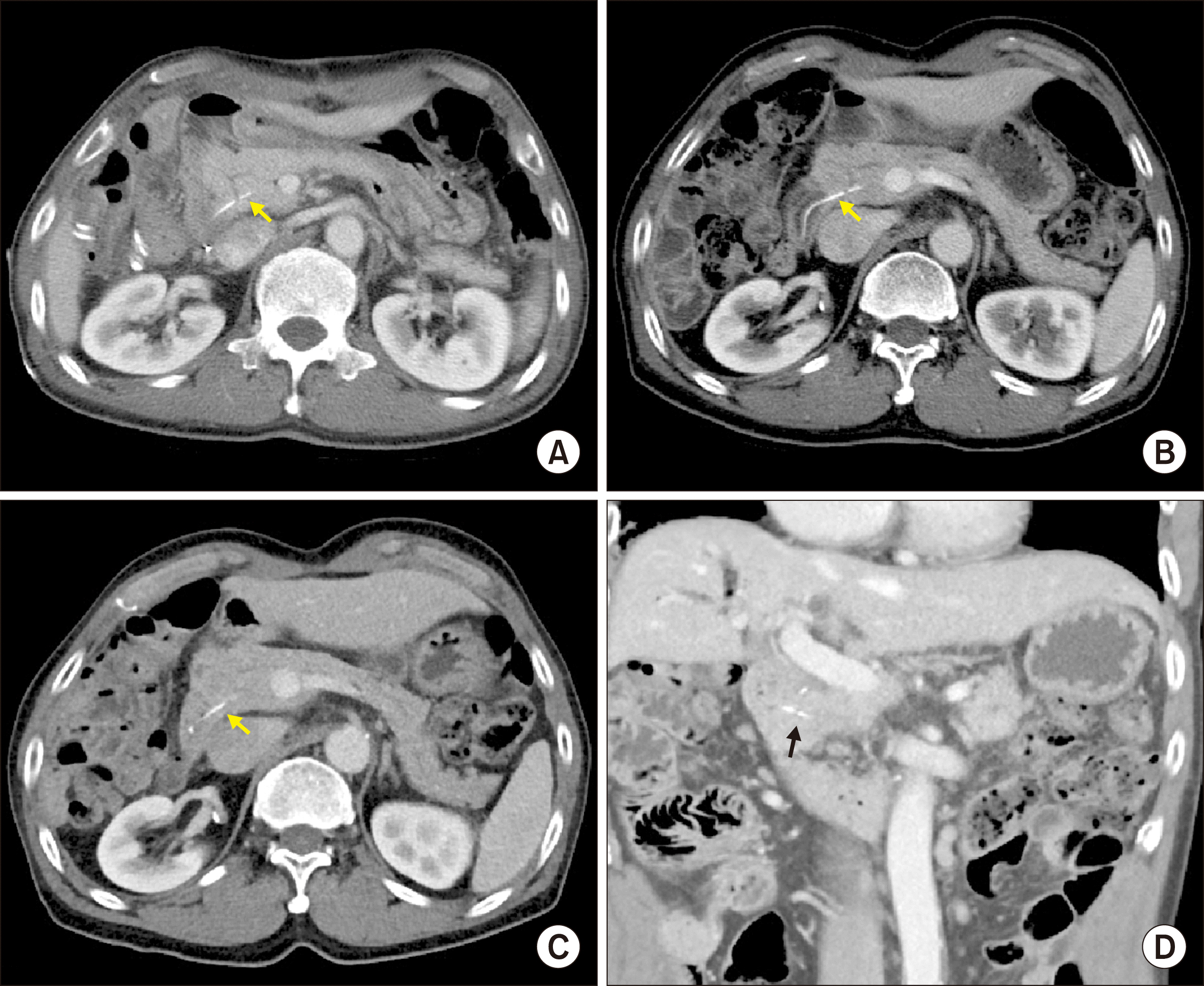
Fig. 3 Imaging study findings of Case 1 taken at 7 days (A), 1 year (B), 3 years (C) and 6 years (D) after the operation. The arrows indicate the internal pancreatic stent.

Fig. 4 Gross photographs of Case 1 specimen after bile duct resection showing intraductal papillary neoplasm with invasive cholangiocarcinoma.
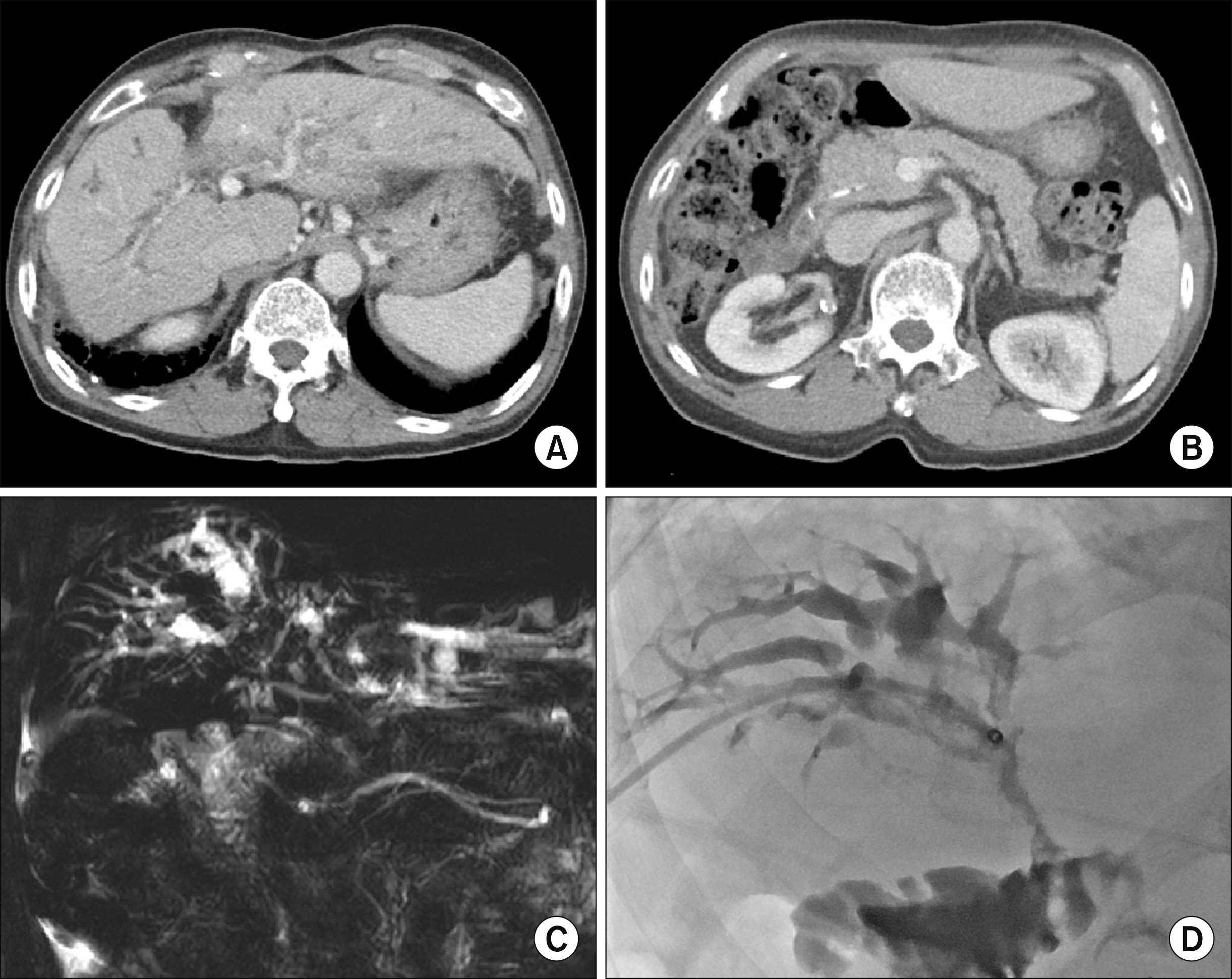
Fig. 5 Imaging study findings of Case 1 showing tumor recurrence at 8 years after the operation. A recurrent tumor is visible at the hepaticojejunostomy site (A), and the pancreatic duct implantation site is intact (B). Magnetic resonance cholangiopancreatography shows intraluminal narrowing (C), thus percutaneous transhepatic biliary drainage was performed for biliary drainage (D).
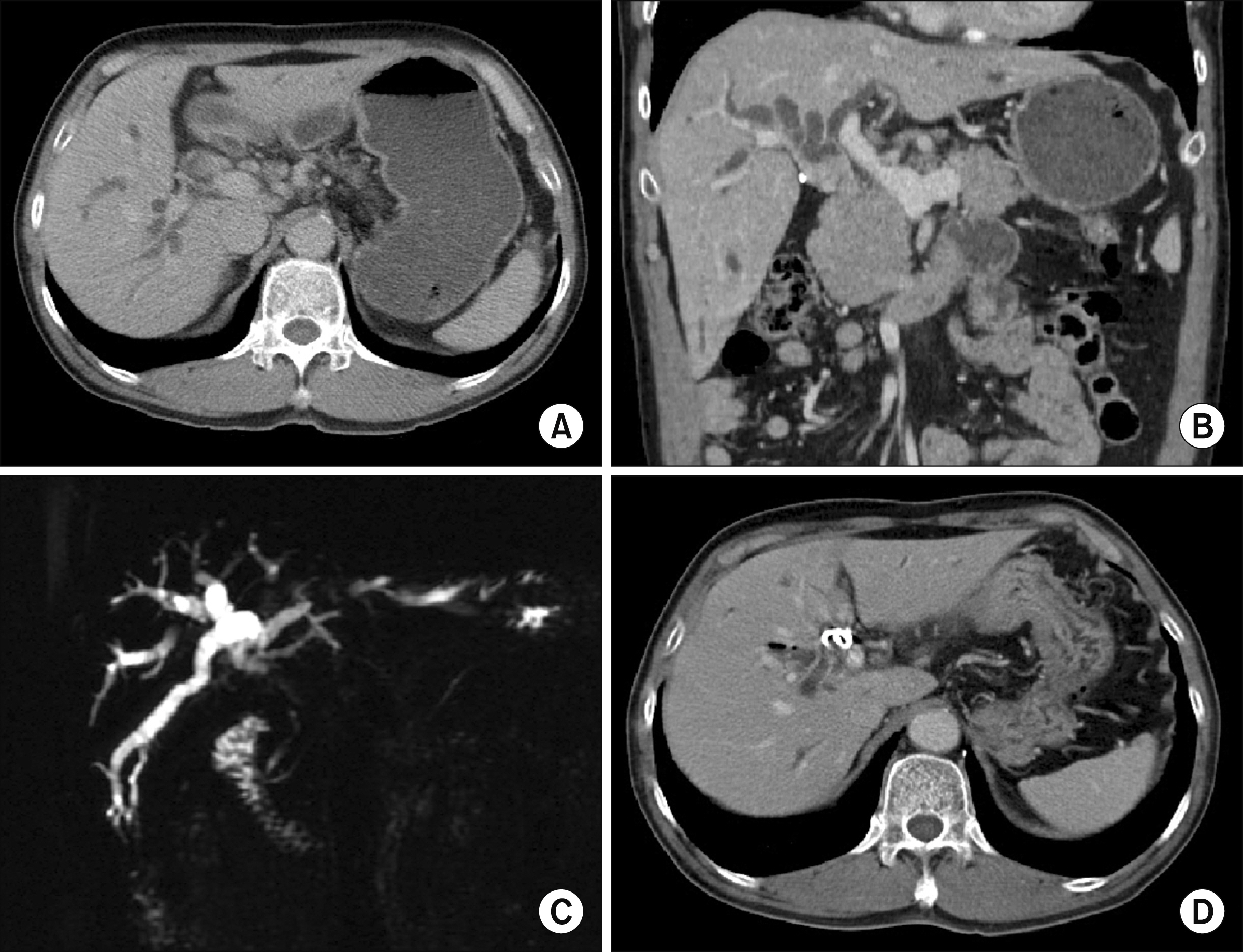
Fig. 6 Initial preoperative radiologic findings of Case 2. (A and B) Computed tomography scan shows perihilar cholangiocarcinoma of Bismuth-Corlette type I. (C) Magnetic resonance cholangiopancreatography shows mass within the bile duct. (D) Endoscopic retrograde biliary drainage is performed for biliary drainage.
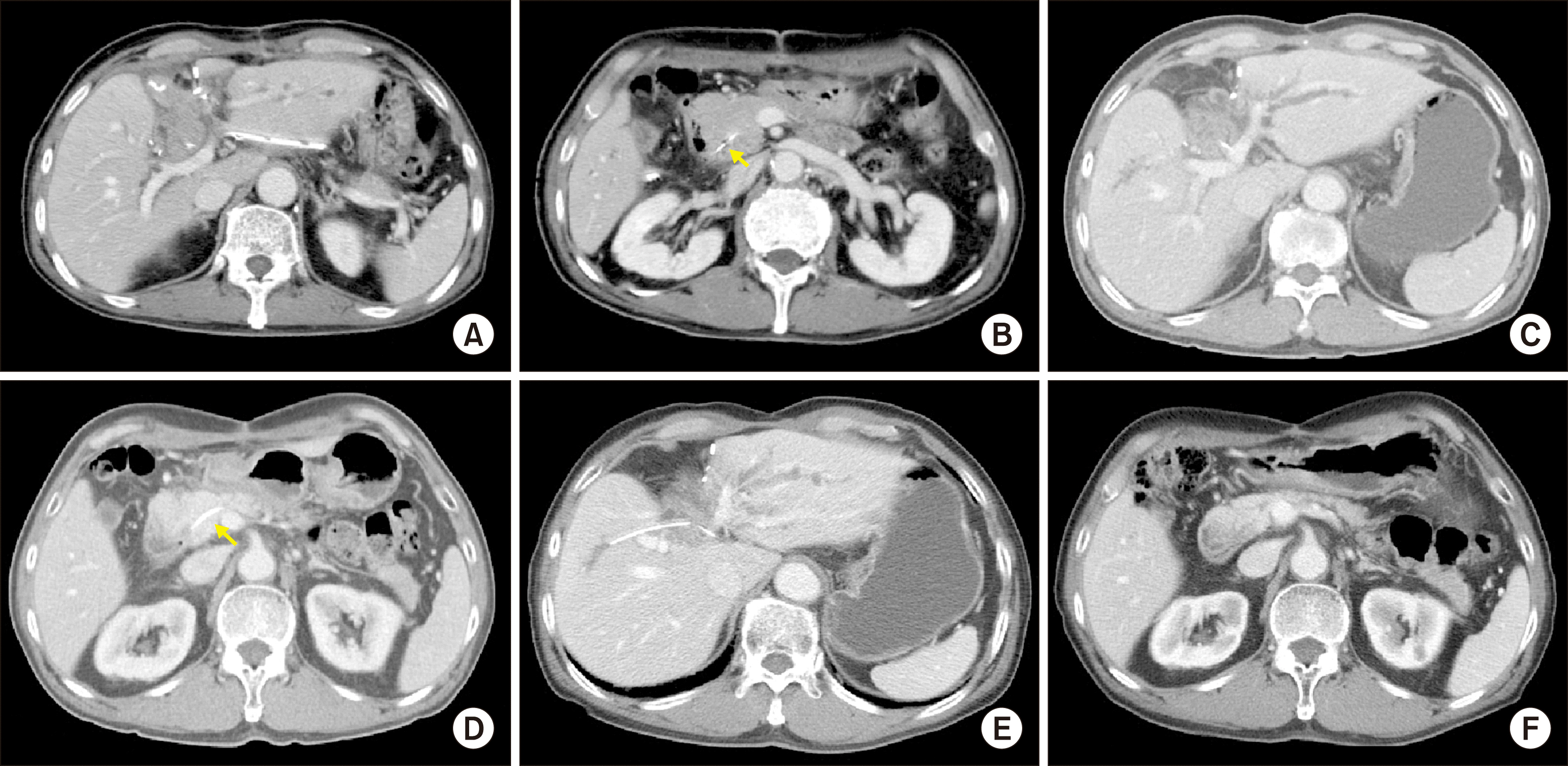
Fig. 7 Imaging study findings of Case 2 taken at 7 days (A and B), 1 month (C and D), and 2 years (E and F) after the operation. The arrows indicate the internal pancreatic stent, which was spontaneously removed before 2 years (F).
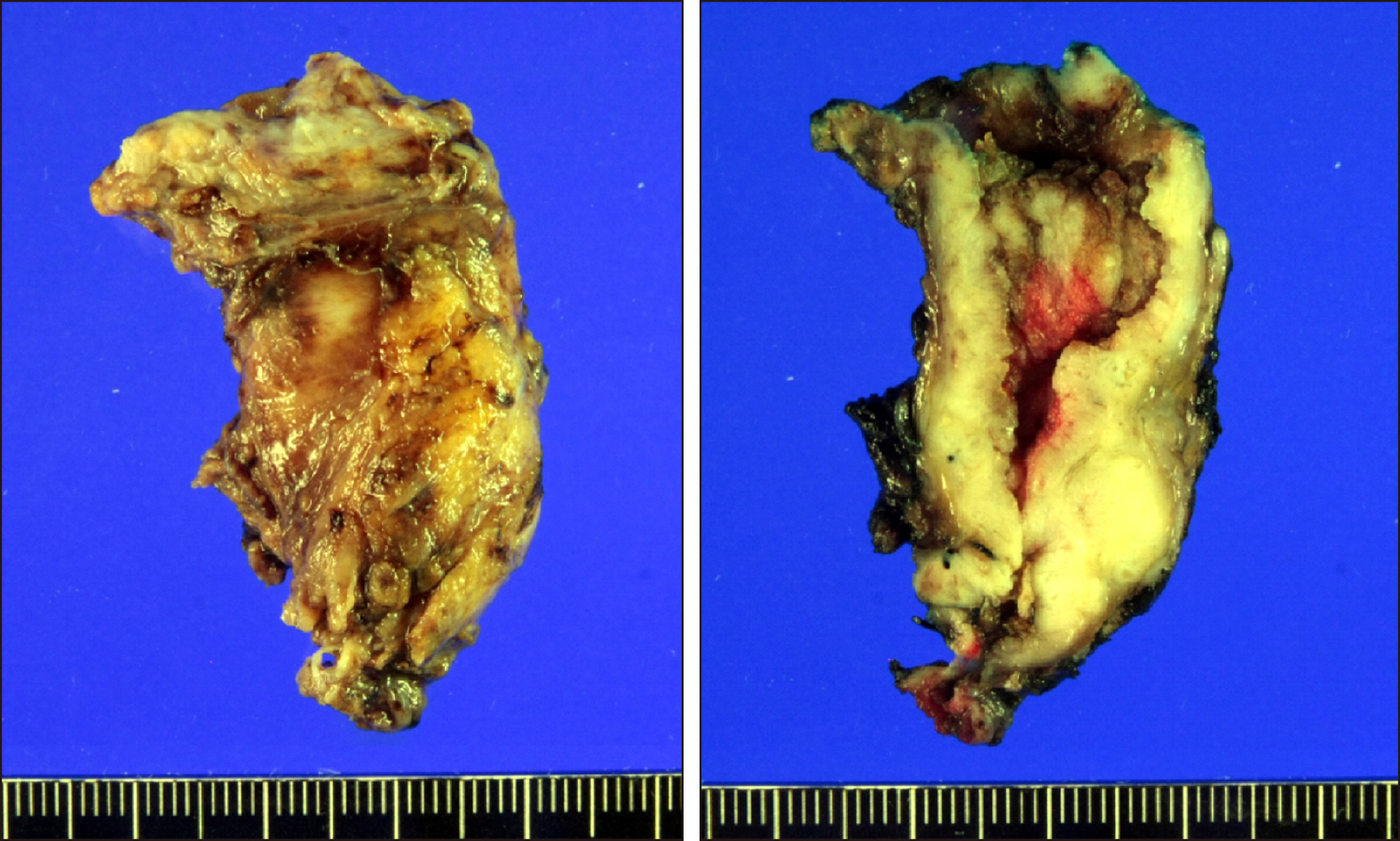
Fig. 8 Gross photographs of Case 2 specimen showing common bile duct adenocarcinoma.
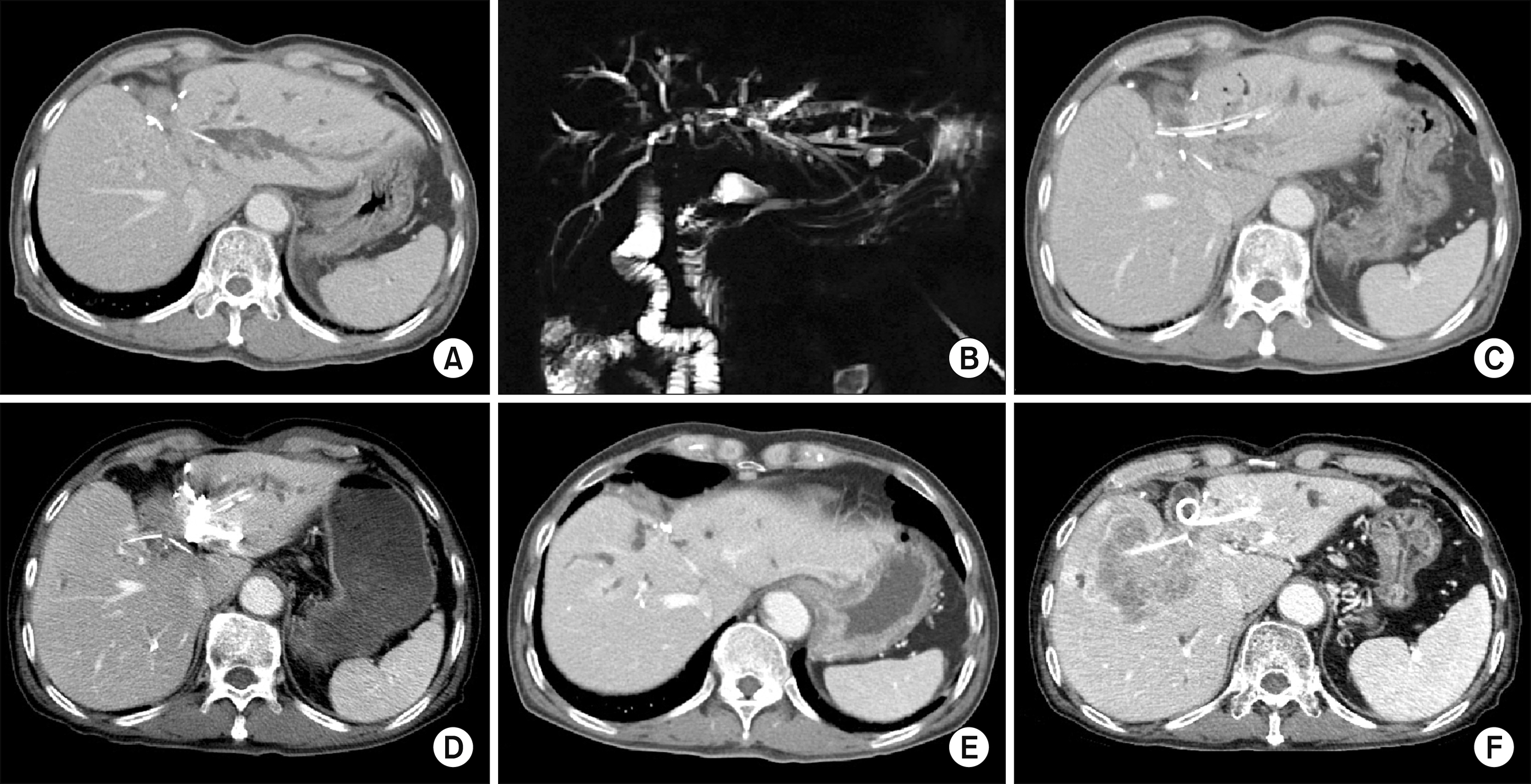
Fig. 9 Imaging study findings of Case 2 showing tumor recurrence at 3-4 years after the operation. A recurrent tumor is visible at the left hepaticojejunostomy site (A and B). Percutaneous transhepatic cholangioscopy was performed to remove the intrahepatic stones from the left lateral segment (C). Percutaneous left portal vein embolization was performed (D). Cholangiohepatitis with abscess formation developed in the right liver (E). Finally, multiple intrahepatic recurrences occurred in the liver (F).
Reference
-
1. Khan SA, Taylor-Robinson SD, Toledano MB, Beck A, Elliott P, Thomas HC. 2002; Changing international trends in mortality rates for liver, biliary and pancreatic tumours. J Hepatol. 37:806–813. DOI: 10.1016/S0168-8278(02)00297-0. PMID: 12445422.
Article2. Murakami Y, Uemura K, Sudo T, Hashimoto Y, Nakashima A, Kondo N, et al. 2011; Prognostic factors after surgical resection for intrahepatic, hilar, and distal cholangiocarcinoma. Ann Surg Oncol. 18:651–658. DOI: 10.1245/s10434-010-1325-4. PMID: 20945107.
Article3. Sakamoto Y, Kosuge T, Shimada K, Sano T, Ojima H, Yamamoto J, et al. 2005; Prognostic factors of surgical resection in middle and distal bile duct cancer: an analysis of 55 patients concerning the significance of ductal and radial margins. Surgery. 137:396–402. DOI: 10.1016/j.surg.2004.10.008. PMID: 15800484.
Article4. Hong SM, Pawlik TM, Cho H, Aggarwal B, Goggins M, Hruban RH, et al. 2009; Depth of tumor invasion better predicts prognosis than the current American Joint Committee on Cancer T classification for distal bile duct carcinoma. Surgery. 146:250–257. DOI: 10.1016/j.surg.2009.02.023. PMID: 19628081. PMCID: PMC3402913.
Article5. Rizvi S, Khan SA, Hallemeier CL, Kelley RK, Gores GJ. 2018; Cholangiocarcinoma - evolving concepts and therapeutic strategies. Nat Rev Clin Oncol. 15:95–111. DOI: 10.1038/nrclinonc.2017.157. PMID: 28994423. PMCID: PMC5819599.
Article6. Sahai P, Kumar S. 2017; External radiotherapy and brachytherapy in the management of extrahepatic and intrahepatic cholangiocarcinoma: available evidence. Br J Radiol. 90:20170061. DOI: 10.1259/bjr.20170061. PMID: 28466653. PMCID: PMC5603950.
Article7. Kiriyama M, Ebata T, Aoba T, Kaneoka Y, Arai T, Shimizu Y, et al. 2015; Prognostic impact of lymph node metastasis in distal cholangiocarcinoma. Br J Surg. 102:399–406. DOI: 10.1002/bjs.9752. PMID: 25611179.8. Kimura W, Miyata H, Gotoh M, Hirai I, Kenjo A, Kitagawa Y, et al. 2014; A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a web-based data entry system: the 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Ann Surg. 259:773–780. DOI: 10.1097/SLA.0000000000000263. PMID: 24253151.9. Addeo P, Delpero JR, Paye F, Oussoultzoglou E, Fuchshuber PR, Sauvanet A, et al. 2014; Pancreatic fistula after a pancreaticoduodenectomy for ductal adenocarcinoma and its association with morbidity: a multicentre study of the French Surgical Association. HPB (Oxford). 16:46–55. DOI: 10.1111/hpb.12063. PMID: 23461663. PMCID: PMC3892314.
Article10. Sugimoto M, Takahashi S, Gotohda N, Kato Y, Kinoshita T, Shibasaki H, et al. 2013; Schematic pancreatic configuration: a risk assessment for postoperative pancreatic fistula after pancreaticoduodenectomy. J Gastrointest Surg. 17:1744–1751. DOI: 10.1007/s11605-013-2320-4. PMID: 23975030.
Article11. Hwang S, Lee SG, Kim KH, Ahn CS, Moon DB, Ha TY, et al. 2008; Extended extrahepatic bile duct resection to avoid performing pancreatoduodenectomy in patients with mid bile duct cancer. Dig Surg. 25:74–79. DOI: 10.1159/000118025. PMID: 18292664.
Article12. Lee SJ, Hwang S, Ha TY, Kim KH, Ahn CS, Moon DB, et al. 2013; Technical knacks and outcomes of extended extrahepatic bile duct resection in patients with mid bile duct cancer. Korean J Hepatobiliary Pancreat Surg. 17:109–112. DOI: 10.14701/kjhbps.2013.17.3.109. PMID: 26155223. PMCID: PMC4304529.
Article13. Hwang S, Jung DJ, Ha TY. 2020; Application of suction-type cigarette drain in leak-prone hepatopancreatobiliary surgery. Ann Hepatobiliary Pancreat Surg. 24:305–308. DOI: 10.14701/ahbps.2020.24.3.305. PMID: 32843596.
Article14. Kolb A, Kleeff J, Frohlich B, Werner J, Friess H, Büchler MW. 2009; Resection of the intrapancreatic bile duct preserving the pancreas. J Hepatobiliary Pancreat Surg. 16:31–34. DOI: 10.1007/s00534-008-0013-2. PMID: 19089312.
Article15. Hwang S, Moon KM, Park JI, Kim MH, Lee SG. 2007; Retroduodenal resection of ampullary carcinoid tumor in a patient with cavernous transformation of the portal vein. J Gastrointest Surg. 11:1322–1327. DOI: 10.1007/s11605-007-0240-x. PMID: 17674113.
Article16. Nishida Y, Sugimoto M, Kojima M, Gotohda N, Konishi M, Takahashi S. 2017; Pancreas-preserving resection of lower biliary tract adenocarcinoma: a coring-out technique. Ann Gastroenterol Surg. 1:150–155. DOI: 10.1002/ags3.12021. PMID: 29863138. PMCID: PMC5881344.
Article17. Kim JK, Hwang HK, Park JS, Cho SI, Yoon DS, Chi HS. 2008; Left hemihepatectomy and caudate lobectomy and complete extrahepatic bile duct resection using transduodenal approach for hilar cholangiocarcinoma arsing from biliary papillomatosis. J Surg Oncol. 98:139–142. DOI: 10.1002/jso.21089. PMID: 18521837.
Article18. Hong S, Song KB, Lee YJ, Park KM, Kim SC, Hwang DW, et al. 2018; Transduodenal ampullectomy for ampullary tumors - single center experience of consecutive 26 patients. Ann Surg Treat Res. 95:22–28. DOI: 10.4174/astr.2018.95.1.22. PMID: 29963536. PMCID: PMC6024084.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent pyogenic cholangitis: The pattern of thickening of the extrahepatic bile duct on CT
- Extrahepatic Bile Duct Duplication with Intraductal Papillary Neoplasm: A Case Report
- A Case of Multiple Papillary Adenocarcinoma of the Extrahepatic Bile Duct : Findings of ERCP
- Intrahepatic Bile Duct Dilatation Caused by Pancreatic Pseudocyst: A Case Report
- Two Cases of Anomalous Termination of the Common Bile Duct and the Pancreatic Duct into the Duodenal Bulb
