Ann Hepatobiliary Pancreat Surg.
2020 Aug;24(3):362-365. 10.14701/ahbps.2020.24.3.362.
Toothpick in the porta: Recurrent liver abscesses secondary to transgastric migration of a toothpick with successful surgical exploration retrieval
- Affiliations
-
- 1Case Western Reserve University, University Hospitals Cleveland Medical Center, Cleveland, OH, USA
- KMID: 2505352
- DOI: http://doi.org/10.14701/ahbps.2020.24.3.362
Abstract
- We present a rare case of a 72-year-old man with recurrent hepatic abscesses secondary to transgastric migration of a toothpick into the liver parenchyma and left portal venous branch. Prior to identification of the foreign body, the patient received multiple courses of antibiotics and underwent image-guided catheter placement without resolution of infection. Given his refractory abdominal pain, fevers, and chills, a repeat abdominal CT was obtained and demonstrated a radio-opaque object extending through the prepyloric gastric submucosa into the liver parenchyma and left portal vein. EGD confirmed a pre-pyloric fistula tract with purulent discharge. The patient subsequently underwent exploratory laparotomy, cholecystectomy, porta hepatis exploration, removal of foreign body, and ligation of porto-enteric fistula tract. A wooden toothpick was removed in its entirety. Interval CT demonstrated resolution of hepatic abscesses and no evidence of persistent porto-enteric fistula. This exceptional case demonstrates the value of multidisciplinary care, hypervigilance for patients with refractory pyogenic liver abscesses of unknown origin, and the importance of careful preoperative planning.
Keyword
Figure
-
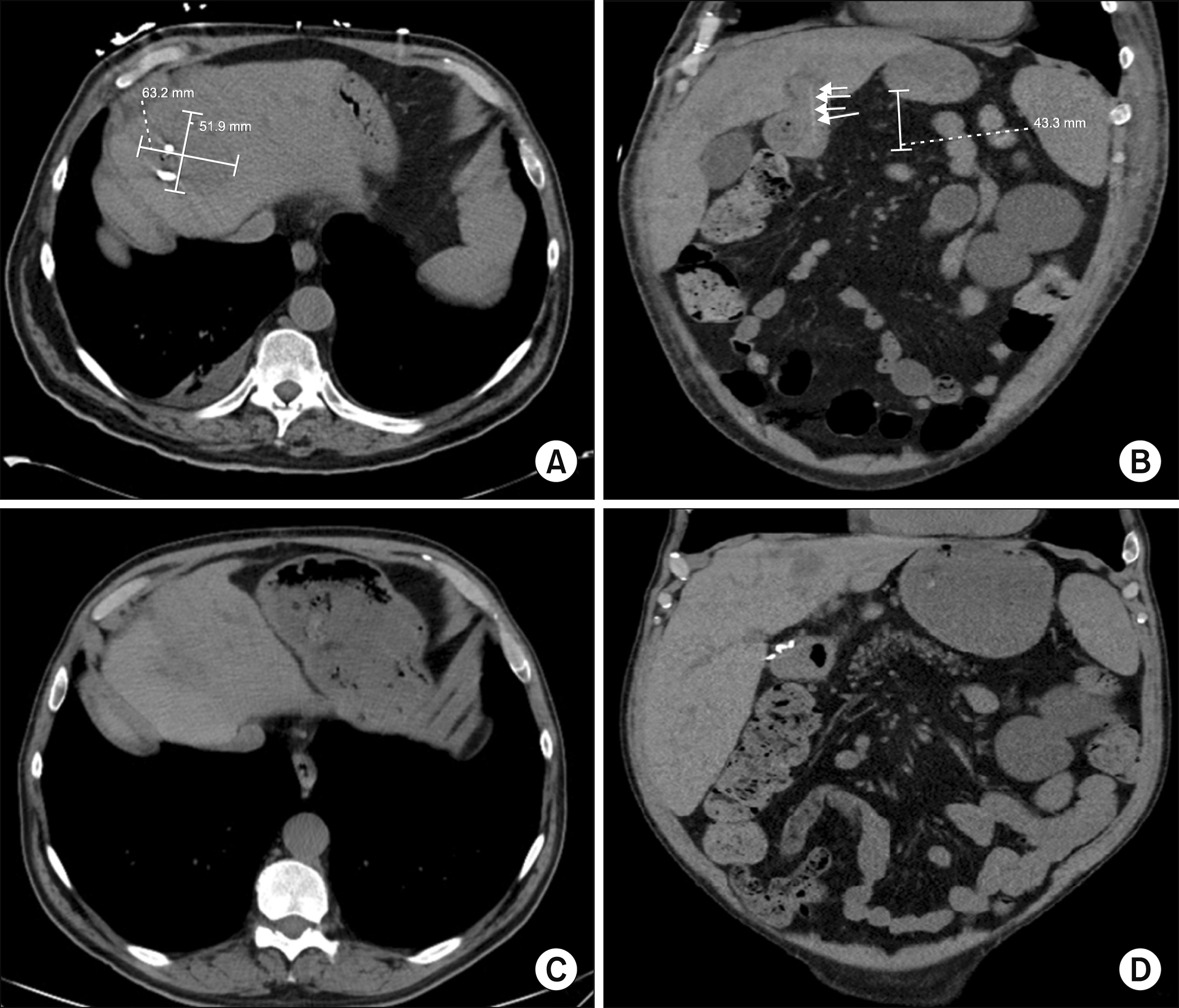
Fig. 1 CT demonstrated persistent liver abscess with IR drain in appropriate position (A). Coronal images (B) demonstrated linear, radio-opaque object extending from gastric wall to liver parenchyma and left portal venous branch. Post-operative imaging demonstrated resolution of hepatic abscess (C) and no evidence of persistent portoenteric fistula (D).
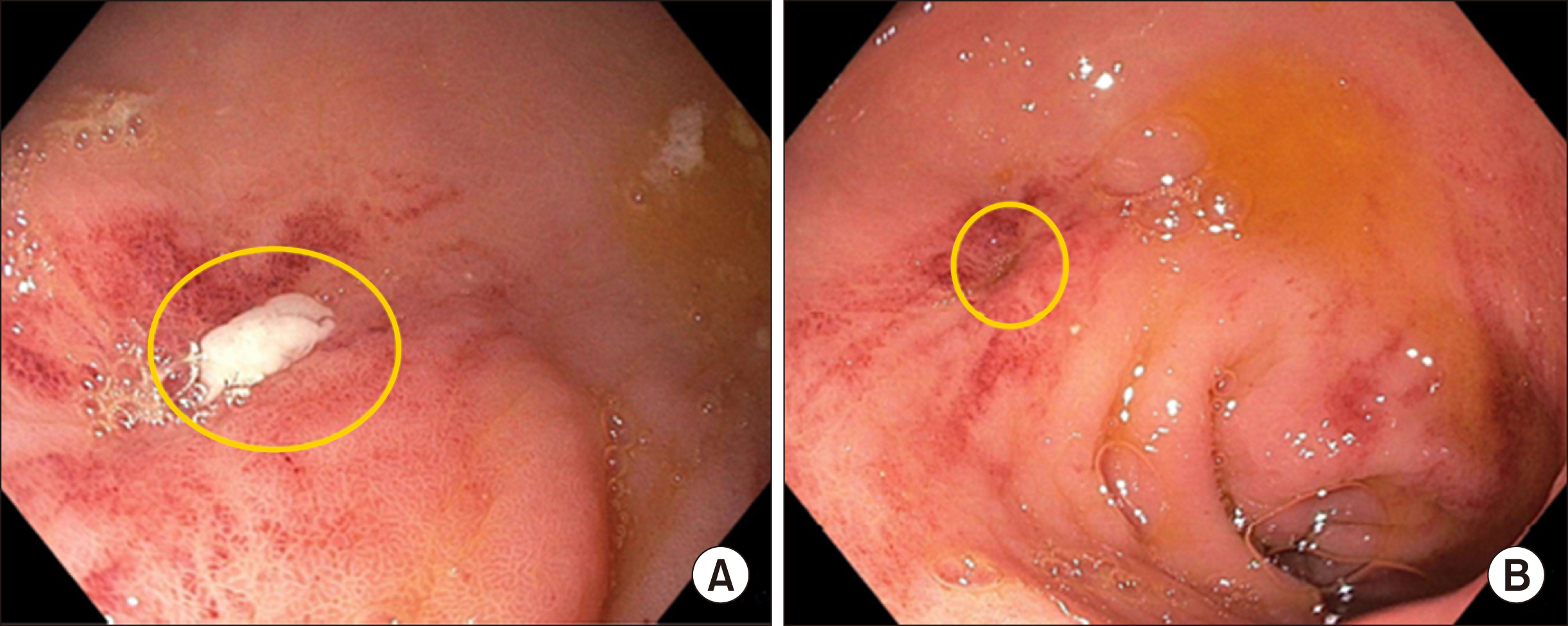
Fig. 2 Endoscopy revealed purulent output (A) from pinpoint fistulous tract (B) in pre-pyloric gastric mucosa.
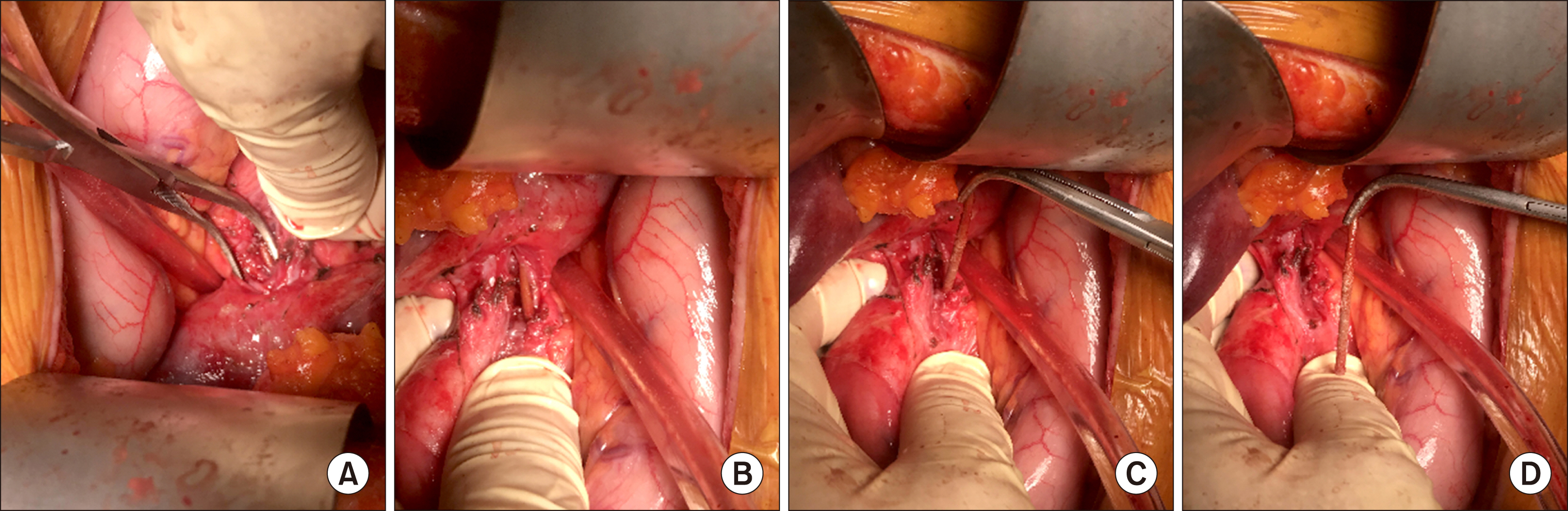
Fig. 3 Intra-operative imaging demonstrating careful dissection of porta hepatis (A) which revealed foreign body (B). A toothpick was carefully isolated (C) and retrieved (D) from the fistula tract without significant hemorrhage.
Reference
-
1. Altemeier WA, Culbertson WR, Fullen WD, Shook CD. 1973; Intra-abdominal abscesses. Am J Surg. 125:70–79. DOI: 10.1016/0002-9610(73)90010-X. PMID: 4566907.
Article2. Kaplan GG, Gregson DB, Laupland KB. 2004; Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin Gastroenterol Hepatol. 2:1032–1038. DOI: 10.1016/S1542-3565(04)00459-8. PMID: 15551257.
Article3. Huang CJ, Pitt HA, Lipsett PA, Osterman FA Jr, Lillemoe KD, Cameron JL, et al. 1996; Pyogenic hepatic abscess. Changing trends over 42 years. Ann Surg. 223:600–607. discussion 607–609. DOI: 10.1097/00000658-199605000-00016. PMCID: PMC1235191. PMID: 8651751.4. Bekki T, Fujikuni N, Tanabe K, Amano H, Noriyuki T, Nakahara M. 2019; Liver abscess caused by fish bone perforation of stomach wall treated by laparoscopic surgery: a case report. Surg Case Rep. 5:79. DOI: 10.1186/s40792-019-0639-0. PMID: 31093821. PMCID: PMC6520427.
Article5. Santos SA, Alberto SC, Cruz E, Pires E, Figueira T, Coimbra E, et al. 2007; Hepatic abscess induced by foreign body: case report and literature review. World J Gastroenterol. 13:1466–1470. DOI: 10.3748/wjg.v13.i9.1466. PMID: 17457985. PMCID: PMC4146938.
Article6. Leggieri N, Marques-Vidal P, Cerwenka H, Denys A, Dorta G, Moutardier V, et al. 2010; Migrated foreign body liver abscess: illustrative case report, systematic review, and proposed diagnostic algorithm. Medicine (Baltimore). 89:85–95. DOI: 10.1097/MD.0b013e3181d41c38. PMID: 20517180.7. Horii K, Yamazaki O, Matsuyama M, Higaki I, Kawai S, Sakaue Y. 1999; Successful treatment of a hepatic abscess that formed secondary to fish bone penetration by percutaneous transhepatic removal of the foreign body: report of a case. Surg Today. 29:922–926. DOI: 10.1007/BF02482788. PMID: 10489138.
Article8. de la Vega M, Rivero JC, Ruíz L, Suárez S. 2001; A fish bone in the liver. Lancet. 358:982. DOI: 10.1016/S0140-6736(01)06106-2. PMID: 11583753.9. Santos-Rosa OM, Lunardelli HS, Ribeiro-Junior MA. 2016; Pyogenic liver abscess: diagnostic and therapeutic management. Arq Bras Cir Dig. 29:194–197. DOI: 10.1590/0102-6720201600030015. PMID: 27759785. PMCID: PMC5074673.
Article10. Meddings L, Myers RP, Hubbard J, Shaheen AA, Laupland KB, Dixon E, et al. 2010; A population-based study of pyogenic liver abscesses in the United States: incidence, mortality, and temporal trends. Am J Gastroenterol. 105:117–124. DOI: 10.1038/ajg.2009.614. PMID: 19888200.
Article11. Kanazawa S, Ishigaki K, Miyake T, Ishida A, Tabuchi A, Tanemoto K, et al. 2003; A granulomatous liver abscess which developed after a toothpick penetrated the gastrointestinal tract: report of a case. Surg Today. 33:312–314. DOI: 10.1007/s005950300071. PMID: 12707832.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic Removal of a Toothpick Impacted in the Stomach Wall by Mucosal Incision
- Colon Perforation by an Ingested Toothpick
- A Case of Liver Abscess Caused by Toothpick Penetrating Gastric Wall
- A Case of Liver Abscess Associated with Duodenal Perforation by a Toothpick
- Toothpick Colon Injury Mimicking Colonic Diverticulitis
