Extended liver resection including hypertrophy concept with portal venous embolisation for giant haemangioma. Too much surgery?
- Strohmaier A
 1,2
1,2 - Wagner KC1,2
- Reese T1,2
- Fard-Aghaie M1,2
- Makridis G1,2
- Rittberg Yv1,2
- Horling K3
- Oldhafer KJ1,2
- Affiliations
-
- 1Division of Hepatobiliary and Pancreatic Surgery, Department of Surgery, Asklepios Hospital Barmbek,Hamburg, Germany
- 2Semmelweis University of Medicine, Asklepios Campus Hamburg, Germany
- 3MVZ Hanse Histologikum GmbH, Hamburg, Germany
- KMID: 2505351
- DOI: http://doi.org/10.14701/ahbps.2020.24.3.357
Abstract
- Haemangiomas of the liver are benign tumours, which are often diagnosed randomly. With an increase in size haemangiomas could become symptomatic. In this case therapeutic options, surgical or interventional, have to be weighted to a conservative approach. We present a case of a 36-year old woman with a symptomatic giant haemangioma of the right liver lobe. Because of the size of the tumor and the small future liver remnant we decided to perform a major liver resection after hypertrophy induction with a preoperative portal vein embolization; an option mainly used for major hepatectomies in malignant tumors of the liver. But however, this case shows, that using a hypertrophy concept also for benign liver tumours is the safer approach, if an extended resection is necessary and the future liver remnant is critical.
Figure
-

Fig. 1 Clinical findings. (A) Photograph from the right patient side. Distended abdomen due to enlarged liver. (B) Marking of the palpabel liver.

Fig. 2 Portal Vein Embolisation of all right hepatic portal veins. (A) Angiography of the portal vein with a five French- Pigtail-Catheter. The catheter is placed in the main portal vein. (B) Portal vein embolization with Glubran of the right anterior and posterior branch.
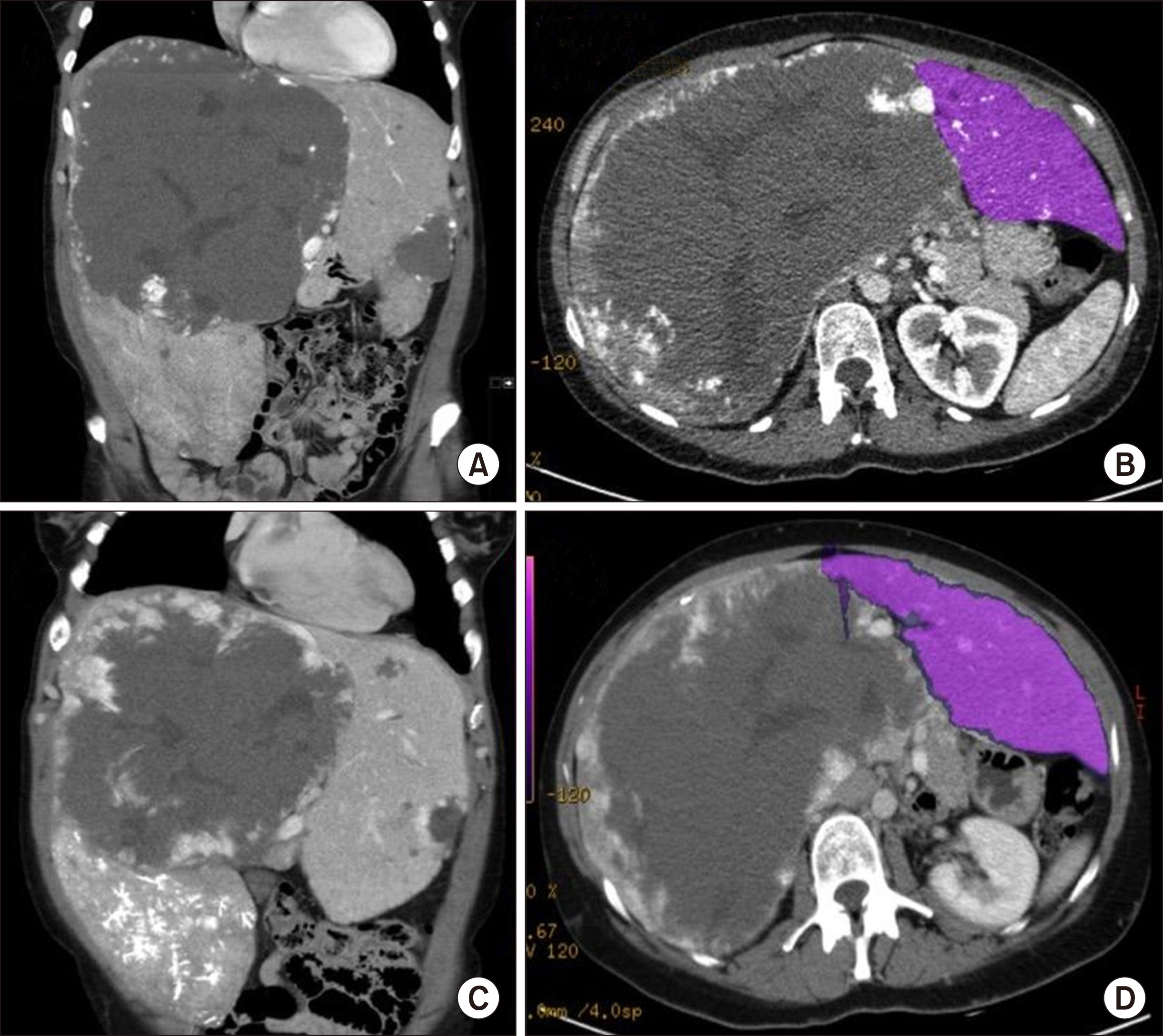
Fig. 3 CT-Scans. (A) Giant haemangioma in the right lobe of the liver and smaller haemangioma in segment III. (B) Volumetric CT scan of the left liver lobe. (C) CT Scan 2 weeks after PVE showing an enlarged left liver lobe. (D) Volumetric CT scan of the left liver lobe after PVE.
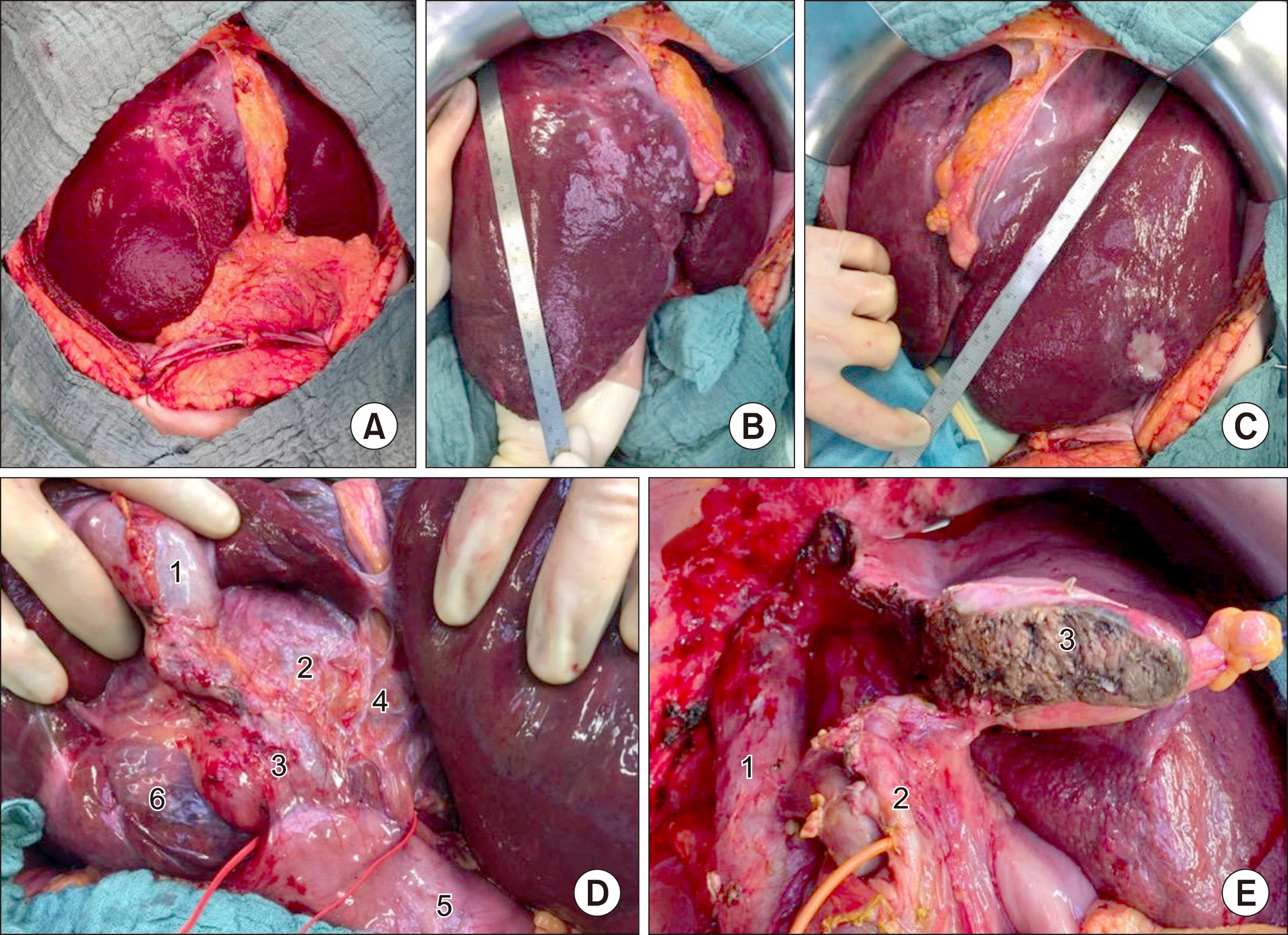
Fig. 4 Intraoperative situs. (A) Open abdomen; (B) Left liver lobe with haemangioma, measuring 29.5 cm; (C) Hypertrophied left liver lobe, measuring 23 cm; (D) Ligamentum hepatoduodenale: Gallbladder (1); Ductus hepaticus communis (2); Ductus choledochus (3); Left hepatic arteries (4); Duodenum (5); Segment I haemangioma (6); (E) Situs after extended right resection: Inferior vena cava (1); Left bile duct with inserted T-drain (2); Resection area (3).

Fig. 5 Pathological findings. (A) Specimen of the extended right resection (liver segment IV-VIII and I); (B) Cross section with characteristic structure of haemangioma with small streak of regular liver parenchyma on the left margin.
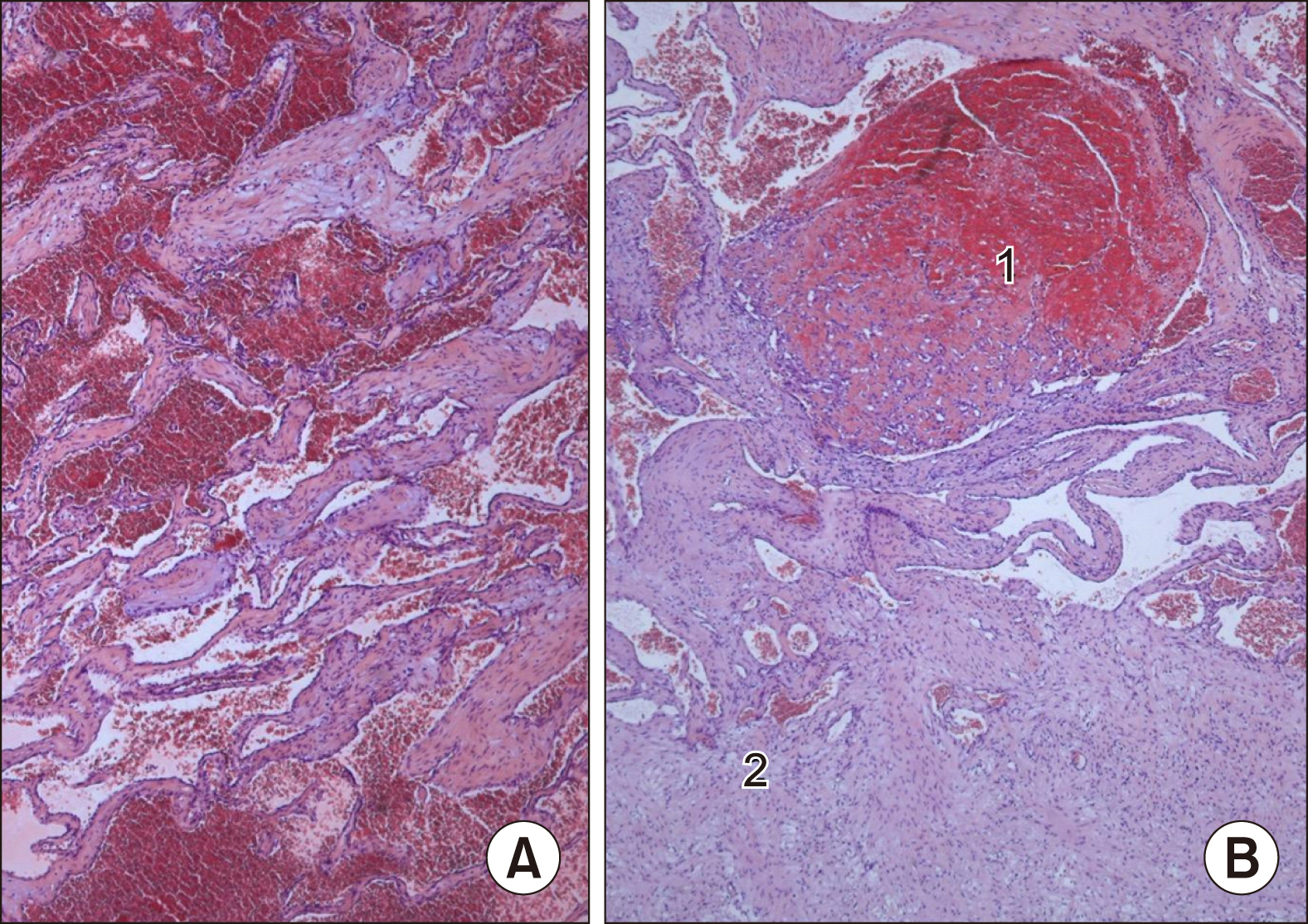
Fig. 6 (A) HE-stained sections showed the classic morphology of a cavernous haemangioma with widely dilated vascular channels lined by flattened inconspicuous endothelial cells and fibrous walls, (B) focal organized thrombi (1) and partial sclerotic areas (2) could be recognised.
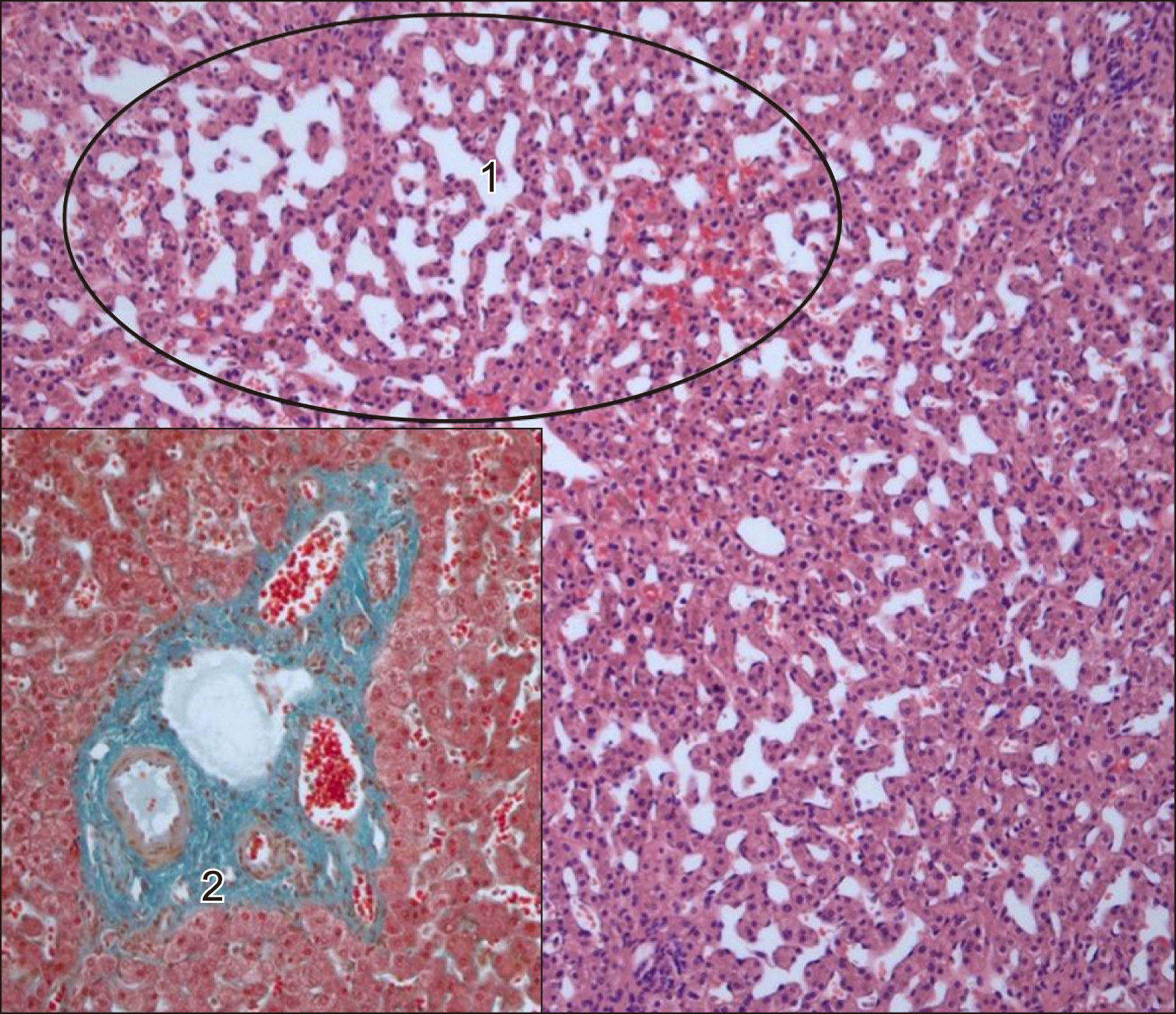
Fig. 7 Adjacent liver parenchyma with peliosis hepatis like sinusoidal dilatation (1) and mild fibrosis of the portal tracts in Elastica van Gieson stain (2).
Reference
-
1. Farges O, Daradkeh S, Bismuth H. 1995; Cavernous hemangiomas of the liver: are there any indications for resection? World J Surg. 19:19–24. DOI: 10.1007/BF00316974. PMID: 7740805.
Article2. Fodor M, Primavesi F, Braunwarth E, Cardini B, Resch T, Bale R, et al. 2018; Indications for liver surgery in benign tumours. Eur Surg. 50:125–131. DOI: 10.1007/s10353-018-0536-y. PMID: 29875801. PMCID: PMC5968066.
Article3. Furumaya A, van Rosmalen BV, Takkenberg RB, van Delden OM, Dejong CHC, Verheij J, et al. 2019; Transarterial (chemo-)embolization and lipiodolization for hepatic haemangioma. Cardiovasc Intervent Radiol. 42:800–811. DOI: 10.1007/s00270-019-02169-x. PMID: 30783780. PMCID: PMC6503075.
Article4. Adhikari DR, Thakur V, Telavane PP, Kulkarni R, Singh R, Joshi RM. 2015; Hypergiant hepatic hemangiomas: case series. Indian J Surg. 77(Suppl 1):40–42. DOI: 10.1007/s12262-014-1104-8. PMID: 25972639. PMCID: PMC4425751.
Article5. Firouznia K, Ghanaati H, Alavian SM, Nassiri Toosi M, Ebrahimi Daryani N, Jalali AH, et al. 2014; Management of liver hemangioma using trans-catheter arterial embolization. Hepat Mon. 14:e25788. DOI: 10.5812/hepatmon.25788. PMID: 25737731. PMCID: PMC4329237.
Article6. Gao J, Ke S, Ding XM, Zhou YM, Qian XJ, Sun WB. 2013; Radiofrequency ablation for large hepatic hemangiomas: initial experience and lessons. Surgery. 153:78–85. DOI: 10.1016/j.surg.2012.06.004. PMID: 22853860.
Article7. Ziemlewicz TJ, Wells SA, Lubner MA, Musat AI, Hinshaw JL, Cohn AR, et al. 2014; Microwave ablation of giant hepatic cavernous hemangiomas. Cardiovasc Intervent Radiol. 37:1299–1305. DOI: 10.1007/s00270-014-0934-x. PMID: 25023180.
Article8. Duxbury MS, Garden OJ. 2010; Giant haemangioma of the liver: observation or resection? Dig Surg. 27:7–11. DOI: 10.1159/000268108. PMID: 20357445.
Article9. Glantzounis GK, Tokidis E, Basourakos SP, Ntzani EE, Lianos GD, Pentheroudakis G. 2017; The role of portal vein embolization in the surgical management of primary hepatobiliary cancers. A systematic review. Eur J Surg Oncol. 43:32–41. DOI: 10.1016/j.ejso.2016.05.026. PMID: 27283892.
Article10. Ketchum WA, Lin-Hurtubise KM, Ochmanek E, Ishihara K, Rice RD. 2019; Management of symptomatic hepatic "mega" hemangioma. Hawaii J Med Public Health. 78:128–131. PMID: 30972235. PMCID: PMC6452022.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Liver Regeneration following Extended Liver Resection combined with Pancreatoduodenectomy
- Blood Loss in Surgery for Aggressive Vertebral Haemangioma with and without Embolisation
- Robotic-assisted right hepatectomy via anterior approach for intrahepatic cholangiocarcinoma
- Portal vein embolization prior to hepatectomy: Techniques, outcomes and novel therapeutic approaches
- Computed Tomography Findings of Thrombosis and Aneurysm of the Portal Venous System
