Application of Novel Intraoperative Neuromonitoring System Using an Endotracheal Tube With Pressure Sensor during Thyroid Surgery: A Porcine Model Study
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Pusan National University School of Medicine and Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea
- 2Department of Otorhinolaryngology-Head and Neck Surgery, School of Medicine, Pusan National University and Medical Research Institute, Pusan National University Hospital, Busan, Korea
- 3Department of Biomedical Engineering, Pusan National University Hospital, Busan, Korea
- KMID: 2504925
- DOI: http://doi.org/10.21053/ceo.2019.01249
Abstract
Objectives
. The loss of signal during intraoperative neuromonitoring (IONM) using electromyography (EMG) in thyroidectomy is one of the biggest problems. We have developed a novel IONM system with an endotracheal tube (ETT) with an attached pressure sensor instead of EMG to detect laryngeal twitching. The aim of the present study was to investigate the feasibility and reliability of this novel IONM system using an ETT with pressure sensor during thyroidectomy in a porcine model.
Methods
. We developed an ETT-attached pressure sensor that uses the piezoelectric effect to measure laryngeal muscle twitching. Stimulus thresholds, amplitude, and latency of laryngeal twitching evaluated using the pressure sensor were compared to those measured using transcartilage needle EMG. The measured amplitude changes by EMG and the pressure sensor during recurrent laryngeal nerve (RLN) traction injury were compared.
Results
. No significant differences in stimulus threshold intensity between EMG and the pressure sensor were observed. The EMG amplitude detected at 0.3 mA, increased with increasing stimulus intensity. When the stimulus was more than 1.0 mA, the amplitude showed a plateau. In a RLN traction injury experiment, the EMG amplitude did not recover even 20 minutes after stopping RLN traction. However, the pressure sensor showed a mostly recovery.
Conclusion
. The change in amplitude due to stimulation of the pressure sensor showed a pattern similar to EMG. Pressure sensors can be feasibly and reliably used for RLN traction injury prediction, RLN identification, and preservation through the detection of laryngeal muscle twitching. Our novel IONM system that uses an ETT with an attached pressure sensor to measure the change of surface pressure can be an alternative to EMG in the future.
Keyword
Figure
-
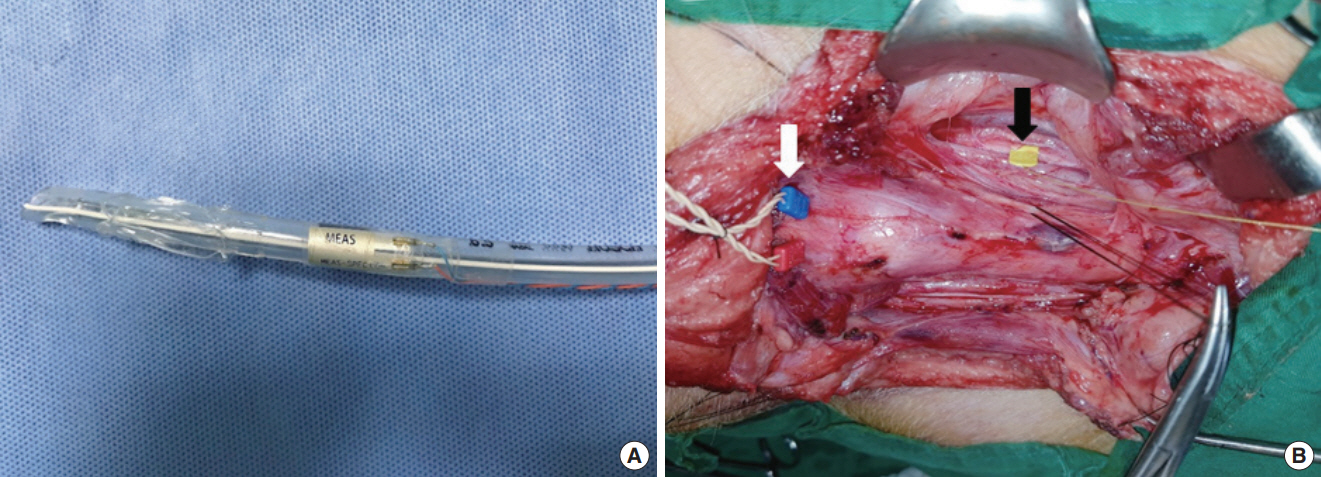
Fig. 1. (A) Novel device and surgical field. Photograph of an endotracheal tube with attached pressure sensor. (B) Photograph of the surgical field on the pig, demonstrating recurrent laryngeal nerve (RLN) traction injury. Transcartilage needle electrodes were inserted into the vocal cord level of both sides of the thyroid cartilage. The automatic periodic stimulation (APS) was placed on the vagus nerve, left under continuous intermittent intraoperative neuromonitoring, and the left RLN was pulled up using silk 3-0. White arrow, electromyography electrodes; Black arrow, APS.

Fig. 2. Electromyography (EMG) and endotracheal tube with pressure sensor recordings, showing the amplitude and latency of EMG and the pressure sensor for 1 mA stimulation using the Nerve Integrity Monitor 3.0 system in pig. Upper graph, pressure sensor signal; Lower graph, EMG signal.
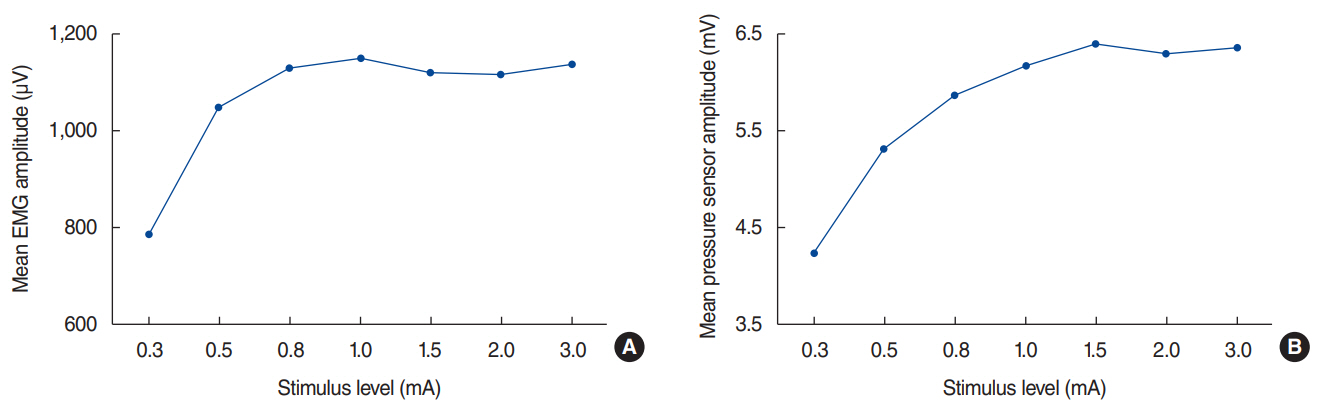
Fig. 3. Change in electromyography (EMG) and pressure sensor according to stimulus. The amplitudes of EMG (A) and the pressure sensor (B) of the vocalis muscle depending on stimulus level.
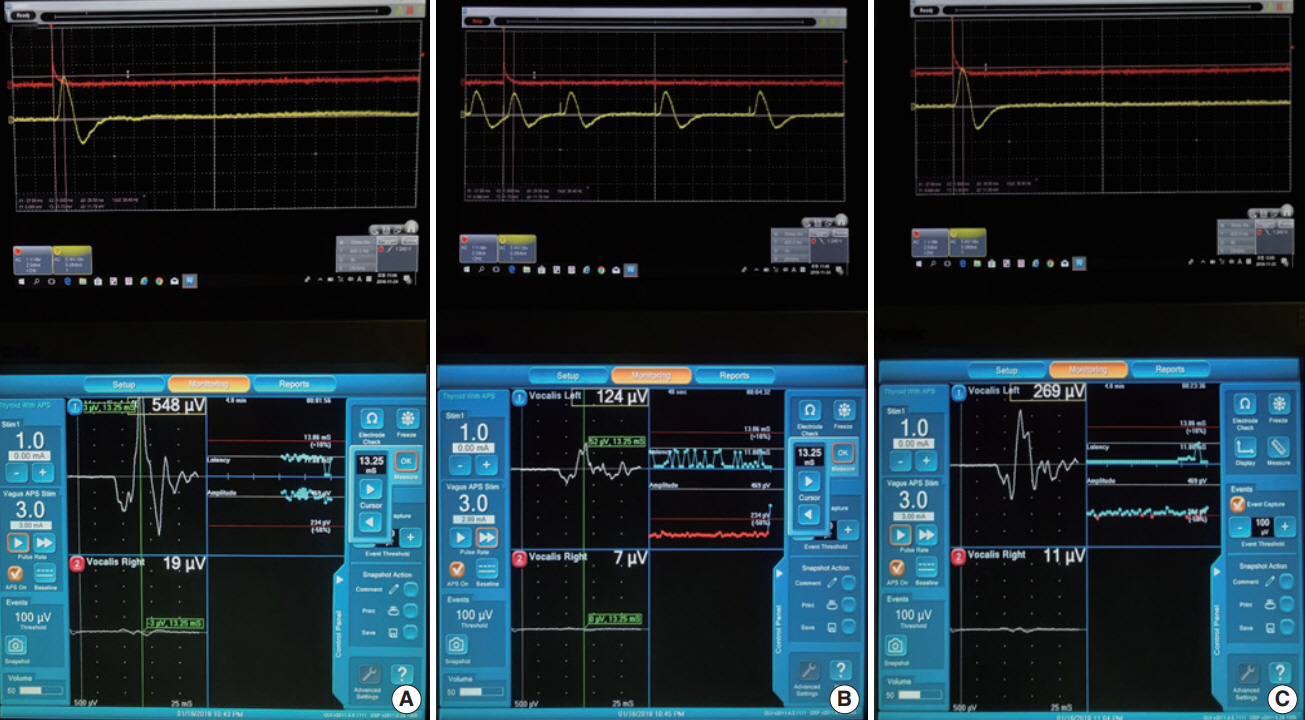
Fig. 4. Continuous amplitude changes of electromyography (EMG) and pressure sensor before recurrent laryngeal nerve (RLN) traction (A), when RLN traction stopped (B), and 20 minutes after RLN traction (C) for 3-mA stimulation using the Nerve Integrity Monitor 3.0 system in pigs. Upper graph, pressure sensor signal; Lower graph, EMG signal.
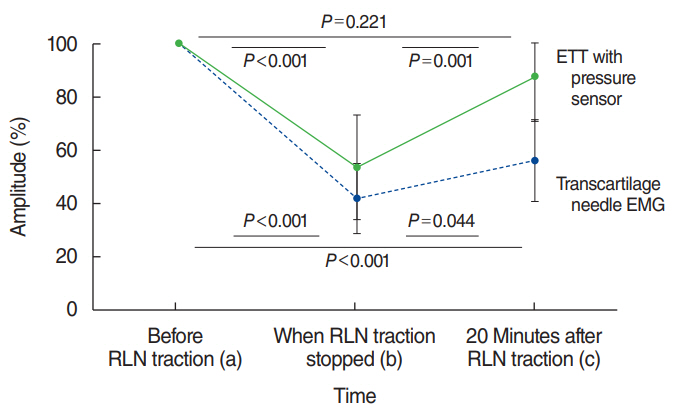
Fig. 5. Amplitude (%) patterns of electromyography (EMG, dotted line) and the pressure sensor (solid line) change depending on the time of the recurrent laryngeal nerve (RLN) traction injury: before RLN traction (a), when RLN traction stopped (b), and 20 minutes after RLN traction (c). a vs. b: P<0.001, b vs. c: P=0.001, a vs. c: P=0.221 in pressure sensor; a vs. b: P<0.001, b vs. c: P=0.044, a vs. c: P<0.001 in EMG. ETT, endotracheal tube.
Cited by 1 articles
-
Intraoperative Neuromonitoring System Using Needle and Skin Electrode during Thyroid Surgery
Sung-Chan Shin, Myeonggu Seo, Yong-Il Cheon, Byung-Joo Lee
Int J Thyroidol. 2022;15(1):17-22. doi: 10.11106/ijt.2022.15.1.17.
Reference
-
1. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016; Jan. 26(1):1–133.
Article2. Chandrasekhar SS, Randolph GW, Seidman MD, Rosenfeld RM, Angelos P, Barkmeier-Kraemer J, et al. Clinical practice guideline: improving voice outcomes after thyroid surgery. Otolaryngol Head Neck Surg. 2013; Jun. 148(6 Suppl):S1–37.3. Jeannon JP, Orabi AA, Bruch GA, Abdalsalam HA, Simo R. Diagnosis of recurrent laryngeal nerve palsy after thyroidectomy: a systematic review. Int J Clin Pract. 2009; Apr. 63(4):624–9.
Article4. Riddell V. Thyroidectomy: prevention of bilateral recurrent nerve palsy. Results of identification of the nerve over 23 consecutive years (1946-69) with a description of an additional safety measure. Br J Surg. 1970; Jan. 57(1):1–11.
Article5. Hermann M, Alk G, Roka R, Glaser K, Freissmuth M. Laryngeal recurrent nerve injury in surgery for benign thyroid diseases: effect of nerve dissection and impact of individual surgeon in more than 27,000 nerves at risk. Ann Surg. 2002; Feb. 235(2):261–8.6. Chiang FY, Wang LF, Huang YF, Lee KW, Kuo WR. Recurrent laryngeal nerve palsy after thyroidectomy with routine identification of the recurrent laryngeal nerve. Surgery. 2005; Mar. 137(3):342–7.
Article7. Randolph GW, Dralle H; International Intraoperative Monitoring Study Group, Abdullah H, Barczynski M, Bellantone R, et al. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011; Jan. 121 Suppl 1:S1–16.
Article8. Sung ES, Lee JC, Shin SC, Choi SW, Jung DW, Lee BJ. Development of a novel detachable magnetic nerve stimulator for intraoperative neuromonitoring. World J Surg. 2018; Jan. 42(1):137–42.
Article9. Sung ES, Lee JC, Kim SH, Shin SC, Jung DW, Lee BJ. Development of an attachable endoscopic nerve stimulator for intraoperative neuromonitoring during endoscopic or robotic thyroidectomy. Otolaryngol Head Neck Surg. 2018; Mar. 158(3):465–8.
Article10. Shin SC, Sung ES, Choi SW, Kim SD, Jung DW, Kim SH, et al. Feasibility and safety of nerve stimulator attachment to energy-based devices: a porcine model study. Int J Surg. 2017; Dec. 48:155–9.
Article11. Snyder SK, Hendricks JC. Intraoperative neurophysiology testing of the recurrent laryngeal nerve: plaudits and pitfalls. Surgery. 2005; Dec. 138(6):1183–91.
Article12. Beldi G, Kinsbergen T, Schlumpf R. Evaluation of intraoperative recurrent nerve monitoring in thyroid surgery. World J Surg. 2004; Jun. 28(6):589–91.
Article13. Lu IC, Chu KS, Tsai CJ, Wu CW, Kuo WR, Chen HY, et al. Optimal depth of NIM EMG endotracheal tube for intraoperative neuromonitoring of the recurrent laryngeal nerve during thyroidectomy. World J Surg. 2008; Sep. 32(9):1935–9.
Article14. Wu CW, Wang MH, Chen CC, Chen HC, Chen HY, Yu JY, et al. Loss of signal in recurrent nerve neuromonitoring: causes and management. Gland Surg. 2015; Feb. 4(1):19–26.15. Dionigi G, Bacuzzi A, Boni L, Rovera F, Dionigi R. What is the learning curve for intraoperative neuromonitoring in thyroid surgery? Int J Surg. 2008; 6 Suppl 1:S7–12.
Article16. Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A; German IONM Study Group. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg. 2008; Jul. 32(7):1358–66.
Article17. Khan A, Pearlman RC, Bianchi DA, Hauck KW. Experience with two types of electromyography monitoring electrodes during thyroid surgery. Am J Otolaryngol. 1997; Mar-Apr. 18(2):99–102.
Article18. Tschopp KP, Gottardo C. Comparison of various methods of electromyographic monitoring of the recurrent laryngeal nerve in thyroid surgery. Ann Otol Rhinol Laryngol. 2002; Sep. 111(9):811–6.
Article19. Rea JL, Khan A. Clinical evoked electromyography for recurrent laryngeal nerve preservation: use of an endotracheal tube electrode and a postcricoid surface electrode. Laryngoscope. 1998; Sep. 108(9):1418–20.
Article20. Marcus B, Edwards B, Yoo S, Byrne A, Gupta A, Kandrevas J, et al. Recurrent laryngeal nerve monitoring in thyroid and parathyroid surgery: the University of Michigan experience. Laryngoscope. 2003; Feb. 113(2):356–61.
Article21. Liddy W, Barber SR, Lin BM, Kamani D, Kyriazidis N, Lawson B, et al. Monitoring of the posterior cricoarytenoid muscle represents another option for neural monitoring during thyroid surgery: normative vagal and recurrent laryngeal nerve posterior cricoarytenoid muscle electromyographic data. Laryngoscope. 2018; Jan. 128(1):283–9.
Article22. Wu CW, Chiang FY, Randolph GW, Dionigi G, Kim HY, Lin YC, et al. Feasibility of intraoperative neuromonitoring during thyroid surgery using transcartilage surface recording electrodes. Thyroid. 2018; Nov. 28(11):1508–16.
Article23. Wu CW, Chiang FY, Randolph GW, Dionigi G, Kim HY, Lin YC, et al. Transcutaneous recording during intraoperative neuromonitoring in thyroid surgery. Thyroid. 2018; Nov. 28(11):1500–7.
Article24. Chiang FY, Lu IC, Kuo WR, Lee KW, Chang NC, Wu CW. The mechanism of recurrent laryngeal nerve injury during thyroid surgery: the application of intraoperative neuromonitoring. Surgery. 2008; Jun. 143(6):743–9.25. Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, et al. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg. 2010; Feb. 34(2):223–9.
Article26. Schneider R, Randolph GW, Sekulla C, Phelan E, Thanh PN, Bucher M, et al. Continuous intraoperative vagus nerve stimulation for identification of imminent recurrent laryngeal nerve injury. Head Neck. 2013; Nov. 35(11):1591–8.
Article27. Sung ES, Lee JC, Shin SC, Kwon HG, Kim MS, Kim DJ, et al. Development of a novel intraoperative neuromonitoring system using a surface pressure sensor to detect muscle movement: a rabbit model study. Clin Exp Otorhinolaryngol. 2019; May. 12(2):217–23.
Article28. Sanabria A, Silver CE, Suarez C, Shaha A, Khafif A, Owen RP, et al. Neuromonitoring of the laryngeal nerves in thyroid surgery: a critical appraisal of the literature. Eur Arch Otorhinolaryngol. 2013; Sep. 270(9):2383–95.
Article29. Lifante JC, McGill J, Murry T, Aviv JE, Inabnet WB 3rd. A prospective, randomized trial of nerve monitoring of the external branch of the superior laryngeal nerve during thyroidectomy under local/regional anesthesia and IV sedation. Surgery. 2009; Dec. 146(6):1167–73.
Article30. Barczynski M, Konturek A, Cichon S. Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg. 2009; Mar. 96(3):240–6.31. Higgins TS, Gupta R, Ketcham AS, Sataloff RT, Wadsworth JT, Sinacori JT. Recurrent laryngeal nerve monitoring versus identification alone on post-thyroidectomy true vocal fold palsy: a meta-analysis. Laryngoscope. 2011; May. 121(5):1009–17.
Article32. Dionigi G, Boni L, Rovera F, Bacuzzi A, Dionigi R. Neuromonitoring and video-assisted thyroidectomy: a prospective, randomized case-control evaluation. Surg Endosc. 2009; May. 23(5):996–1003.
Article33. Chan WF, Lo CY. Pitfalls of intraoperative neuromonitoring for predicting postoperative recurrent laryngeal nerve function during thyroidectomy. World J Surg. 2006; May. 30(5):806–12.
Article34. Bai B, Chen W. Protective effects of intraoperative nerve monitoring (IONM) for recurrent laryngeal nerve injury in thyroidectomy: meta-analysis. Sci Rep. 2018; May. 8(1):7761.
Article35. Chiang FY, Lu IC, Chang PY, Dionigi G, Randolph GW, Sun H, et al. Comparison of EMG signals recorded by surface electrodes on endotracheal tube and thyroid cartilage during monitored thyroidectomy. Kaohsiung J Med Sci. 2017; Oct. 33(10):503–9.
Article36. Sung ES, Lee JC, Shin SC, Kwon HK, Na HS, Park DH, et al. Development of a novel intraoperative neuromonitoring system using an accelerometer sensor in thyroid surgery: a porcine model study. Clin Exp Otorhinolaryngol. 2019; Nov. 12(4):420–6.
Article37. Randolph GW, Kobler JB, Wilkins J. Recurrent laryngeal nerve identification and assessment during thyroid surgery: laryngeal palpation. World J Surg. 2004; Aug. 28(8):755–60.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Neuromonitoring during Thyroid Surgery
- Development of a Novel Intraoperative Neuromonitoring System Using an Accelerometer Sensor in Thyroid Surgery: A Porcine Model Study
- Development of a Novel Intraoperative Neuromonitoring System Using a Surface Pressure Sensor to Detect Muscle Movement: A Rabbit Model Study
- Development of the Novel Intraoperative Neuromonitoring for Thyroid Surgery
- Intraoperative Neuromonitoring System Using Needle and Skin Electrode during Thyroid Surgery
