Thyroid-Stimulating Hormone-Secreting Pituitary Adenomas : Single Institutional Experience of 14 Consecutive Cases
- Affiliations
-
- 1Department of Neurological Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2504644
- DOI: http://doi.org/10.3340/jkns.2019.0169
Abstract
Objective
: Thyroid-stimulating hormone (TSH)-secreting pituitary adenoma (PA) is an extremely rare functioning form of PA that accounts for 0.7–2% of all such cases. The previously reported outcomes of the surgical removal of TSH-PA are poor. Owing to its extremely low incidence, most available reports on TSH-PA are case reports or small case series. Thus, we investigated the clinical and endocrinological outcomes of surgically treated TSH-PA through our institutional series.
Methods
: We retrospectively reviewed 14 consecutive cases of surgically treated TSH-PA, focusing on the clinical, radiological, surgical, and endocrinological data.
Results
: There were seven male (50%) and seven female (50%) patients. The mean age was 42.5 years (range, 19–63). The mean tumor size was 16.6 mm (range, 4–30). Optic chiasm compression was noted in six patients (42.9%), and no patient showed cavernous sinus invasion. Thirteen of 14 patients (92.8%) underwent transnasal transsphenoidal approach (TSA), and one patient underwent TSA followed by transcranial approach for residual tumor removal. Thirteen of 14 patients (92.8%) showed endocrinological remission; all patients who experienced remission showed subnormal levels of TSH (<0.4 μU/mL) on postoperative day 2. Recurrence occurred in two patients (14.2%). One patient underwent subsequent revision transnasal TSA for recurrent tumor removal, and the other patient underwent gamma knife radiosurgery for recurrence.
Conclusion
: Surgical treatment showed excellent surgical outcomes. The TSH level in the immediate postoperative period may be a predictor for endocrinological remission.
Figure
-
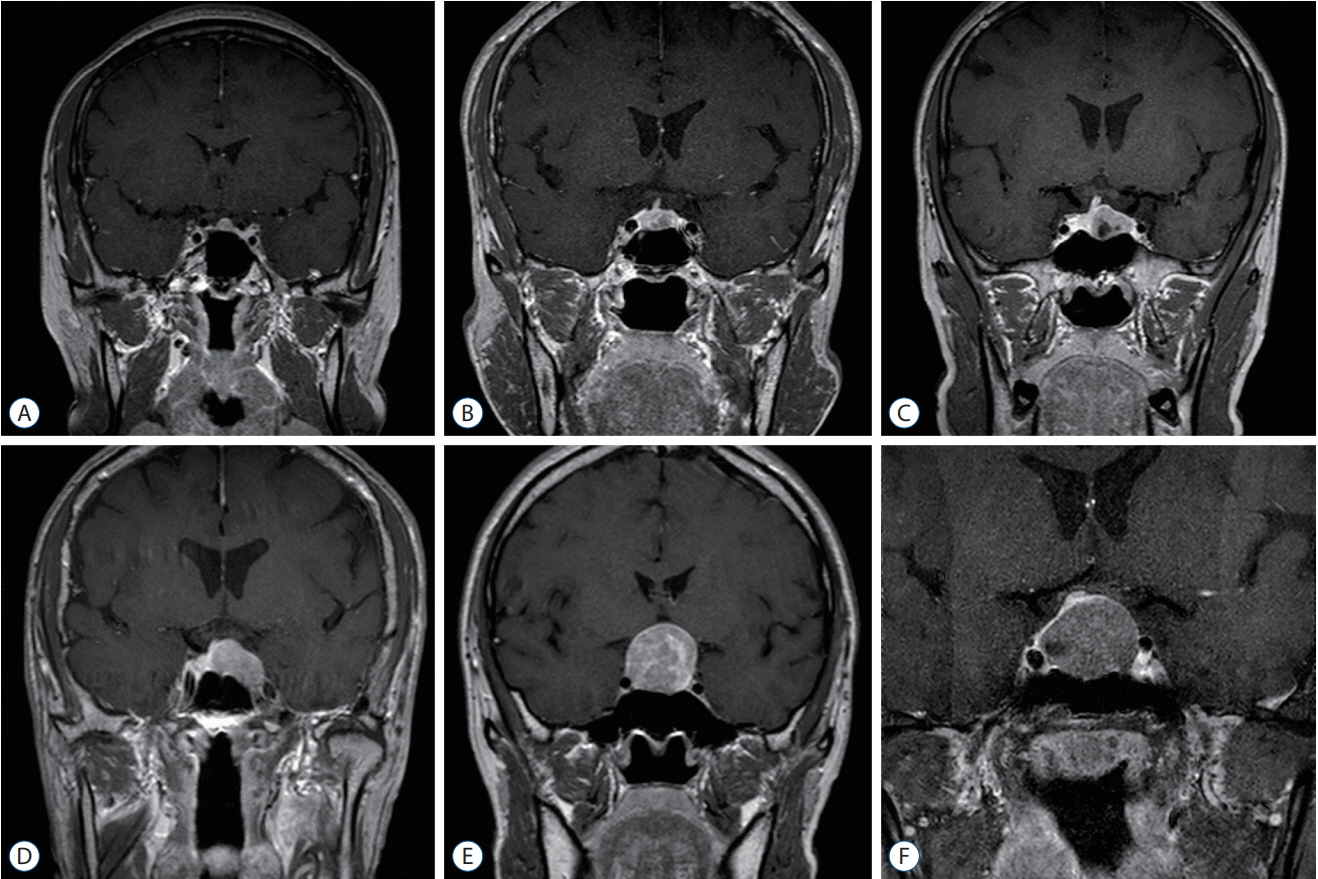
Fig. 1. Various radiological findings of TSH-secreting pituitary adenomas. A–F : Various shapes and sizes of TSH-PA tumors. All of these patients underwent transnasal transsphenoidal surgery and experienced endocrinological remission. TSH : thyroid-stimulating hormone, PA : pituitary adenoma.
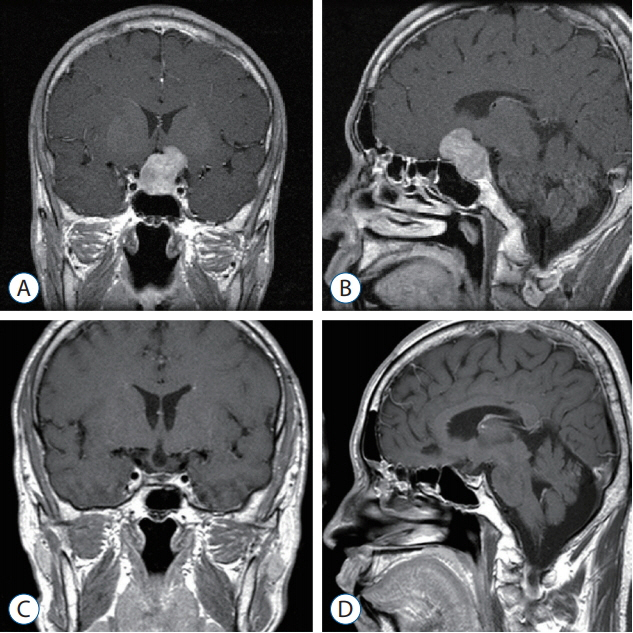
Fig. 2. Representative case of TSH-secreting pituitary adenomas. In a 33-year-old male patient, the tumor grew in the suprasellar area and extended to the anterior cranial fossa. The patient underwent combined transnasal transsphenoidal surgery followed by transcranial surgery via left pterional craniotomy. Postoperative endocrinological remission was achieved (A and B : preoperative sagittal and coronal T1-weighted enhanced MRI image, C and D : postoperative coronal and sagittal T1-weighted enhanced MRI image). TSH : thyroid-stimulating hormone, MRI : magnetic resonance imaging.
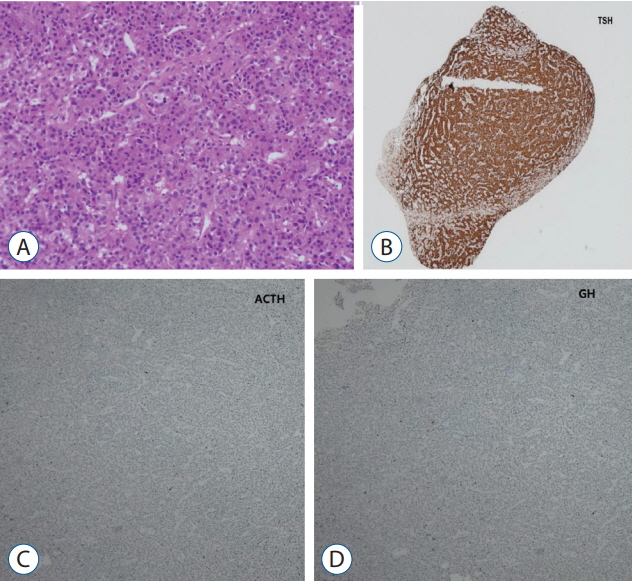
Fig. 3. A : Monomorphic cell with granular cytoplasm, round nuclei, and dispersed chromatin are present in the adenoma (Hematoxylin-Eosin staining, ×100). B-D : Immunostaining for TSH, ACTH, GH, and tumor showed positivity for TSH (B : TSH immuostaining, ×4; C : ACTH immunostaining, ×40; D : GH immunostaining, ×40). TSH : thyroid-stimulating hormone, ACTH : adrenocorticotropic hormone, GH : growth hormone.

Fig. 4. A case of recurrent TSH-secreting pituitary adenoma. A : A 46-yearold female patient with a tumor located on left side of the sella and deviated pituitary stalk on brain MRI. The patient underwent transnasal transsphenoidal surgery and experienced hormonal remission after surgery. B : Follow-up MRI performed at postoperative 3 months showed no evidence of residual tumor. C and D : Gamma knife radiosurgery planning image; irradiation field included sella and left cavernous sinus. TSH : thyroid-stimulating hormone, MRI : magnetic resonance imaging.

Fig. 5. Kaplan-Meier analysis of recurrence-free survival. Recurrence-free survival of enrolled patients. The 5-year and 20-year recurrence-free survival rates were 88.9% and 76.2%, respectively. TSH : thyroid-stimulating hormone.
Reference
-
References
1. Beck-Peccoz P, Lania A, Beckers A, Chatterjee K, Wemeau JL. 2013 European thyroid association guidelines for the diagnosis and treatment of thyrotropin-secreting pituitary tumors. Eur Thyroid J. 2:76–82. 2013.
Article2. Beck-Peccoz P, Persani L. Medical management of thyrotropin-secreting pituitary adenomas. Pituitary. 5:83–88. 2002.3. Brucker-Davis F, Oldfield EH, Skarulis MC, Doppman JL, Weintraub BD. Thyrotropin-secreting pituitary tumors: diagnostic criteria, thyroid hormone sensitivity, and treatment outcome in 25 patients followed at the National Institutes of Health. J Clin Endocrinol Metab. 84:476–486. 1999.
Article4. Ezzat S, Horvath E, Kovacs K, Smyth HS, Singer W, Asa SL. Basic fibroblast growth factor expression by two prolactin and thyrotropinproducing pituitary adenomas. Endocr Pathol. 6:125–134. 1995.
Article5. Hughes JD, Young WF, Chang AY, Link MJ, Garces YI, Laack NN, et al. Radiosurgical management of patients with persistent or recurrent cushing disease after prior transsphenoidal surgery: a management algorithm based on a 25-year experience. Neurosurgery. 86:557–564. 2020.
Article6. Knosp E, Steiner E, Kitz K, Matula C. Pituitary adenomas with invasion of the cavernous sinus space: a magnetic resonance imaging classification compared with surgical findings. Neurosurgery. 33:610–617. discussion 617-618. 1993.
Article7. Macchia E, Gasperi M, Lombardi M, Morselli L, Pinchera A, Acerbi G, et al. Clinical aspects and therapeutic outcome in thyrotropin-secreting pituitary adenomas: a single center experience. J Endocrinol Invest. 32:773–779. 2009.
Article8. Micko AS, Wöhrer A, Wolfsberger S, Knosp E. Invasion of the cavernous sinus space in pituitary adenomas: endoscopic verification and its correlation with an MRI-based classification. J Neurosurg. 122:803–811. 2015.
Article9. Minniti G, Osti MF, Niyazi M. Target delineation and optimal radiosurgical dose for pituitary tumors. Radiat Oncol. 11:135. 2016.
Article10. Minnitia G, Clarkea E, Scaringia C, Enrici RM. Stereotactic radiotherapy and radiosurgery for non-functioning and secreting pituitary adenomas. Rep Pract Oncol Radiother. 21:370–378. 2016.
Article11. Mouslech Z, Somali M, Sakali AK, Savopoulos C, Mastorakos G, Hatzitolios AI. TSH-secreting pituitary adenomas treated by gamma knife radiosurgery: our case experience and a review of the literature. Hormones (Athens). 15:122–128. 2016.
Article12. Mouslech Z, Somali M, Sakali AK, Savopoulos C, Mastorakos G, Hatzitolios AI. TSH-secreting pituitary adenomas treated by gamma knife radiosurgery: our case experience and a review of the literature. Hormones. 15:122–128. 2016.
Article13. Ónnestam L, Berinder K, Burman P, Dahlqvist P, EdenEngström B, Wahlberg J, et al. National incidence and prevalence of TSH-secreting pituitary adenomas in Sweden. J Clin Endocrinol Metab. 98:626–635. 2013.
Article14. Ostrom QT, Gittleman H, Fulop J, Liu M, Blanda R, Kromer C, et al. CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2008-2012. Neuro Oncol 17 Suppl 4. iv1–iv62. 2015.
Article15. Palace MR. Perioperative management of thyroid dysfunction. Health Serv Insights. 10:1178632916689677. 2017.
Article16. Rotermund R, Riedel N, Burkhardt T, Matschke J, Schmidt N-O, Aberle J, et al. Surgical treatment and outcome of TSH-producing pituitary adenomas. Acta Neurochir (Wien). 159:1219–1226. 2017.
Article17. Sanno N, Teramoto A, Osamura RY. Long-term surgical outcome in 16 patients with thyrotropin pituitary adenoma. J Neurosurg. 93:194–200. 2000.
Article18. Tjornstrand A, Gunnarsson K, Evert M, Holmberg E, Ragnarsson O, Rosén T, et al. The incidence rate of pituitary adenomas in western Sweden for the period 2001-2011. Eur J Endocrinol. 171:519–526. 2014.
Article19. Tjörnstrand A, Nyström HF. Diagnostic approach to TSH-producing pituitary adenoma. Eur J Endocrinol. 177:R183–R197. 2017.20. Yamada S, Fukuhara N, Horiguchi K, Yamaguchi-Okada M, Nishioka H, Takeshita A, et al. Clinicopathological characteristics and therapeutic outcomes in thyrotropin-secreting pituitary adenomas: a single-center study of 90 cases. J Neurosurg. 121:1462–1473. 2014.
Article21. Zhao W, Ye H, Li Y, Zhou L, Lu B, Zhang S, et al. Thyrotropin-secreting pituitary adenomas: diagnosis and management of patients from one Chinese center. Wien Klin Wochenschr. 124:678–684. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Microsurgical Transsphenoidal Approach for Pituitary Denomas
- Comparative evaluation of CT and secreting hormones in pituitary adenomas
- MRI of the TSH(Thyroid Stimulating Hormone) -Secreting Pituitary Adenoma
- Clinical Characteristics and Treatments of Patients with TSH Secreting Pituitary Adenoma
- Pituitary Adenomas in Childhood and Adolescence
