J Korean Neurosurg Soc.
2020 Jul;63(4):427-432. 10.3340/jkns.2019.0151.
Paradigm Shift in Intra-Arterial Mechanical Thrombectomy for Acute Ischemic Stroke : A Review of Randomized Controlled Trials after 2015
- Affiliations
-
- 1Department of Neurosurgery, Uijeongbu St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Uijeongbu, Korea
- KMID: 2504636
- DOI: http://doi.org/10.3340/jkns.2019.0151
Abstract
- Three randomized control trials (RCTs), published in 2013, investigated efficacy of mechanical thrombectomy in large vessel occlusions and did not show better results compared to intravenous (IV) recombinant tissue-type plasminogen activator (tPA) alone. However, most clinicians treating stroke consider mechanical thrombectomy as the standard treatment rather than using IV tPA alone. This paradigm shift was based on five RCTs investigating efficacy of mechanical thrombectomy in acute ischemic stroke conducted from 2010 to 2015. They demonstrated that mechanical thrombectomy was effective and safe in acute ischemic stroke with anterior circulation occlusion when performed within 6 hours of stroke onset. There are four reasons underlying the different results observed between the trials conducted in 2013 and 2015. First, the three RCTs of 2013 used low-efficiency thrombectomy devices. Second, the three RCTs used insufficient image selection criteria. Third, following the initial presentation at the hospital, reperfusion treatment required a long time. Fourth, the three RCTs showed a low rate of successful recanalization. Time is the most important factor in the treatment of acute ischemic stroke. However, current trends utilize advanced imaging techniques, such as diffusion-weighted imaging and multi-channel computer tomographic perfusion, to facilitate the detection of core infarction, penumbra, and collateral flows. These efforts demonstrate that patient selection may overcome the barriers of time in specific cases.
Keyword
Figure
-
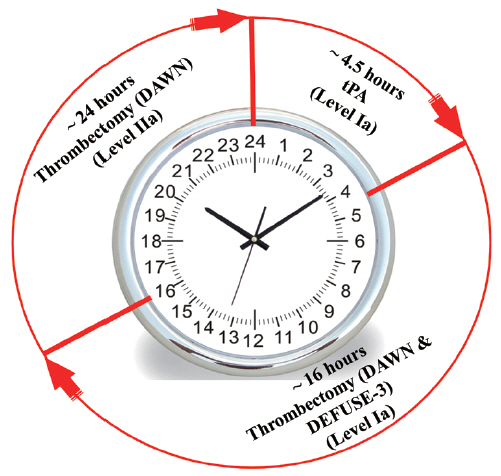
Fig. 1. 2018 Stroke guidelines extend the thrombectomy window to 24 hours. In selected patients with acute ischemic stroke who have large vessel occlusion in the anterior circulation, mechanical thrombectomy is recommended 1) within 6 to 16 hours of last known normal and meet DAWN or DEFUSE 3 eligibility criteria and 2) within 16 to 24 hours of last known normal and meet DAWN eligibility criteria. DAWN : DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo, DEFUSE-3 : Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke.
Reference
-
References
1. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutierrez S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 378:708–718. 2018.
Article2. Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 372:11–20. 2015.3. Bracard S, Ducrocq X, Mas JL, Soudant M, Oppenheim C, Moulin T, et al. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol. 15:1138–1147. 2016.
Article4. Broderick JP, Palesch YY, Demchuk AM, Yeatts SD, Khatri P, Hill MD, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 368:893–903. 2013.
Article5. Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 372:1009–1018. 2015.
Article6. Ciccone A, Valvassori L, Nichelatti M, Sgoifo A, Ponzio M, Sterzi R, et al. Endovascular treatment for acute ischemic stroke. N Engl J Med. 368:904–913. 2013.
Article7. Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 372:1019–1030. 2015.
Article8. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 387:1723–1731. 2016.
Article9. Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med. 372:2296–2306. 2015.
Article10. Kidwell CS, Jahan R, Gornbein J, Alger JR, Nenov V, Ajani Z, et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med. 368:914–923. 2013.
Article11. Muir KW, Ford GA, Messow CM, Ford I, Murray A, Clifton A, et al. Endovascular therapy for acute ischaemic stroke: the Pragmatic Ischaemic Stroke Thrombectomy Evaluation (PISTE) randomised, controlled trial. J Neurol Neurosurg Psychiatry. 88:38–44. 2017.
Article12. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 378:11–21. 2018.13. Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, et al. 2015 American Heart Association/American Stroke Association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 46:3020–3035. 2015.
Article14. Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 372:2285–2295. 2015.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evolution of Endovascular Therapy in Acute Stroke: Implications of Device Development
- Endovascular Treatment of Acute Ischemic Stroke
- Intra-Arterial Thrombolysis to Improve Final Thrombolysis in Cerebral Infarction Score after Thrombectomy: A Case-Series Analysis
- Forced Arterial Suction Thrombectomy Using Distal Access Catheter in Acute Ischemic Stroke
- Adjuvant Tirofiban Injection Through Deployed Solitaire Stent As a Rescue Technique After failed Mechanical Thrombectomy in Acute Stroke
