Atypical femoral neck fracture after prolonged bisphosphonate therapy
- Affiliations
-
- 1Department of Orthopaedic Surgery, Konyang Unversity Hospital, Daejeon, Korea
- 2Department of Pathology, Konyang Unversity Hospital, Daejeon, Korea
- KMID: 2504566
- DOI: http://doi.org/10.4132/jptm.2020.05.14
Abstract
- Of the drugs developed to prevent and treat osteoporosis, bisphosphonate has played a very important role in preventing osteoporotic fractures. However, case reports describing atypical femoral fractures in patients using long-term bisphosphonates have emerged. The majority of atypical femur fractures occurs in the lateral aspect of the subtrochanteric or femur diaphysis, which is explained by accumulation of tensile stress in these areas. Although the superior cortex of the femur neck withstands maximum tensile stress, to our knowledge, there have been only two reports (three cases) of atypical femoral neck fracture. In addition, none of those case reports revealed detailed pathology related to suppressed bone turnover rate. We encountered an incomplete femoral neck fracture and diagnosed it as “atypical” on the basis of the patient’s lack of trauma and medication history and pathological findings. For patients with groin pain, minimal or no trauma, and a history of long-term bisphosphonate use, an atypical femoral neck fracture should be considered.
Figure
-

Fig. 1. (A) A radiograph performed 3 weeks before referral to our hospital shows a minimal fracture line (white arrow) on the superior cortex of the right femoral neck. (B) A radiograph performed at our hospital at admission shows a more definite and nearly vertical radiolucent line (fracture) in the right femoral neck. (C) T1 magnetic resonance imaging shows a decreased signal intensity in the superior and central aspect of the right femoral neck, which represents bone marrow edema.

Fig. 2. (A) Specimen shows a definite incomplete fracture of the superior femoral neck (arrow). (B) A thin fracture line (arrows) extends through the entire thickness of the cortex. (C) A thin fracture gap contained amorphous acellular material (asterisk) but no hematoma, vessels, chondrocytes, or inflammatory cells. However, remodeling cavities with increased cellular activity are seen in the bone adjacent to the fracture gap (arrows). (D) A deep portion of the fracture site is mostly replaced by fibrovascular tissue with a focal area of osteoid formation representing the fracture-healing process (magnification of square area of B).
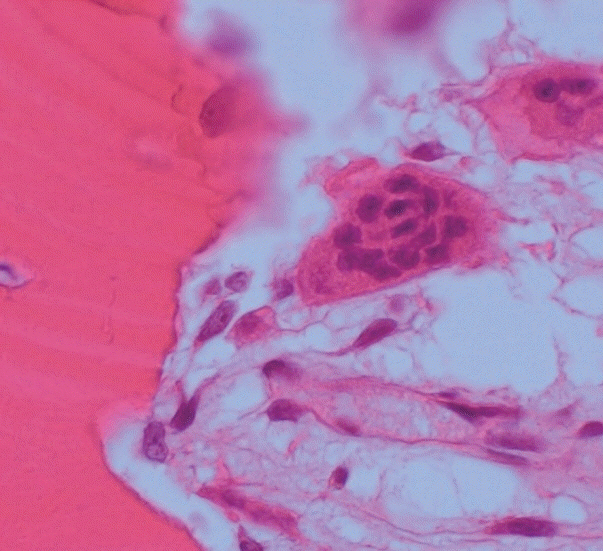
Fig. 3. A giant multinucleated osteoclast with more than 8 nuclei detached from the shallow resorption cavity.
Reference
-
1. Shane E, Burr D, Ebeling PR, et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2010; 25:2267–94.
Article2. Koh JS, Goh SK, Png MA, Ng AC, Howe TS. Distribution of atypical fractures and cortical stress lesions in the femur: implications on pathophysiology. Singapore Med J. 2011; 52:77–80.3. Koch JC. The laws of bone architecture. Am J Anat. 1917; 21:177–298.
Article4. Kim DH, Lee EC, Kang SK. Insufficiency fracture of ipsilateral femur neck in patient treated with long term bisphosphonate treatment: a case report. J Bone Metab. 2012; 19:159–62.5. Khan SK, Savaridas T, Hemers JS, Maarouf Z, Orgee JM, Orr MM. Atraumatic intracapsular neck of femur fractures after prolonged bisphosphonate treatment: a new atypical variant? Clin Cases Miner Bone Metab. 2016; 13:38–41.
Article6. Schilcher J, Sandberg O, Isaksson H, Aspenberg P. Histology of 8 atypical femoral fractures: remodeling but no healing. Acta Orthop. 2014; 85:280–6.7. Kajino Y, Kabata T, Watanabe K, Tsuchiya H. Histological finding of atypical subtrochanteric fracture after long-term alendronate therapy. J Orthop Sci. 2012; 17:313–8.
Article8. Weinstein RS, Roberson PK, Manolagas SC. Giant osteoclast formation and long-term oral bisphosphonate therapy. N Engl J Med. 2009; 360:53–62.
Article9. Whyte MP, Wenkert D, Clements KL, McAlister WH, Mumm S. Bisphosphonate-induced osteopetrosis. N Engl J Med. 2003; 349:457–63.
Article10. Jain N, Weinstein RS. Giant osteoclasts after long-term bisphosphonate therapy: diagnostic challenges. Nat Rev Rheumatol. 2009; 5:341–6.
Article11. Lorget F, Kamel S, Mentaverri R, et al. High extracellular calcium concentrations directly stimulate osteoclast apoptosis. Biochem Biophys Res Commun. 2000; 268:899–903.
Article12. Nielsen RH, Karsdal MA, Sorensen MG, Dziegiel MH, Henriksen K. Dissolution of the inorganic phase of bone leading to release of calcium regulates osteoclast survival. Biochem Biophys Res Commun. 2007; 360:834–9.
Article13. Rogers MJ, Crockett JC, Coxon FP, Mönkkönen J. Biochemical and molecular mechanisms of action of bisphosphonates. Bone. 2011; 49:34–41.
Article14. Cremers S, Papapoulos S. Pharmacology of bisphosphonates. Bone. 2011; 49:42–9.
Article15. Parks TG, Baird DS, Wilson RI. Stress fractures of the neck of the femur. Ulster Med J. 1970; 39:111–8.16. Bone HG, Hosking D, Devogelaer JP, et al. Ten years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med. 2004; 350:1189–99.
Article17. Greenblatt MB, Tsai JN, Wein MN. Bone turnover markers in the diagnosis and monitoring of metabolic bone disease. Clin Chem. 2017; 63:464–74.
Article18. Osada R, Zukawa M, Kimura T. Atypical ulnar fracture associated with long-term bisphosphonate use. J Orthop Sci. 2015; 20:1132–5.
Article19. Breglia MD, Carter JD. Atypical insufficiency fracture of the tibia associated with long-term bisphosphonate therapy. J Clin Rheumatol. 2010; 16:76–8.
Article20. Patel V, Graves L, Lukert B. Pelvic fractures associated with longterm bisphosphonate therapy-case report. J Musculoskelet Neuronal Interact. 2013; 13:251–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Epidemiology and Clinical Features of Atypical Femoral Fractures
- Atypical Fracture of the Proximal Shaft of the Ulna Associated with Prolonged Bisphosphonate Therapy
- Is It a Simple Stress Fracture or Bisphosphonate-related Atypical Fracture?
- Management Challenges in Atypical Femoral Fractures: A Case Report
- Atypical Fracture of the Ulna Associated with 3 Years of Bisphosphonate Medication
