Perioperative risk factors of progressive chronic kidney disease following liver transplantation: analyses of a 10-year follow-up single-center cohort
- Affiliations
-
- 1Division of Nephrology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 2Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 3Department of Anesthesiology and Pain Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
- 4Statistics and Data Center, Research Institute for Future Medicine, Samsung Medical Center, Seoul, Korea
- KMID: 2503460
- DOI: http://doi.org/10.4174/astr.2020.99.1.52
Abstract
- Purpose
The incidence of chronic kidney disease (CKD) has been increasing due to improved survival after liver transplantation (LT). Risk factors of kidney injury after LT, especially perioperative management factors, are potentially modifiable. We investigated the risk factors associated with progressive CKD for 10 years after LT.
Methods
This retrospective cohort study included 292 adult patients who underwent LT at a tertiary referral hospital between 2000 and 2008. Renal function was assessed by the e stimated glomerular filtration rate (eGFR) using the Modification of Diet in Renal Disease formula. The area under the curve of serial eGFR (AUCeGFR) was calculated for each patient to assess the trajectory of eGFR over the 10 years. Low AUCeGFR was considered progressive CKD. Linear regression analyses were performed to examine the associations between the variables and AUCeGFR.
Results
Multivariable analysis showed that older age (regression coefficient = -0.53, P < 0.001), diabetes mellitus (DM) (regression coefficient = -6.93, P = 0.007), preoperative proteinuria (regression coefficient = -16.11, P < 0.001), preoperative acute kidney injury (AKI) (regression coefficient = -14.35, P < 0.001), postoperative AKI (regression coefficient = -3.86, P = 0.007), and postoperative mean vasopressor score (regression coefficient = -0.45, P = 0.034) were independently associated with progressive CKD.
Conclusion
More careful renoprotective management is required in elderly LT patients with DM or preexisting proteinuria. Postoperative AKI and vasopressor dose may be potentially modifiable risk factors for progressive CKD.
Figure
-
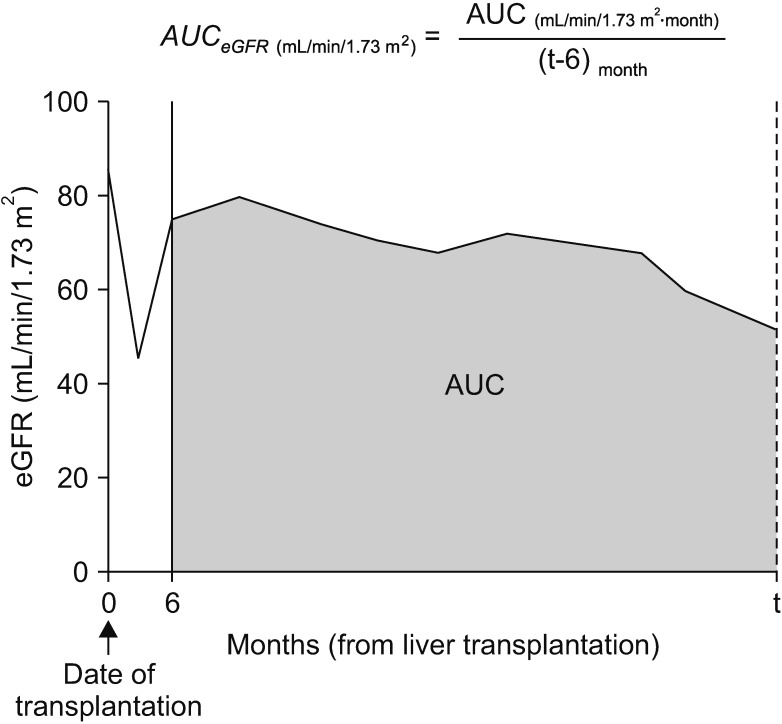
Fig. 1 An example of serial changes in eGFR after transplantation and calculation of AUCeGFR. Month 0 corresponds to the time of transplantation. The initial 6 months following transplantation were excluded from AUC calculation. AUC was divided by individual follow-up duration (t). In patients who died or were lost to follow-up within 10 years, “t” corresponds to survival duration or follow-up duration, respectively. In other cases (patients who survived 10 years or more after transplantation with complete follow-up), “t” corresponds to 120 (months). AUC, area under the curve; eGFR, estimated glomerular filtration rate.
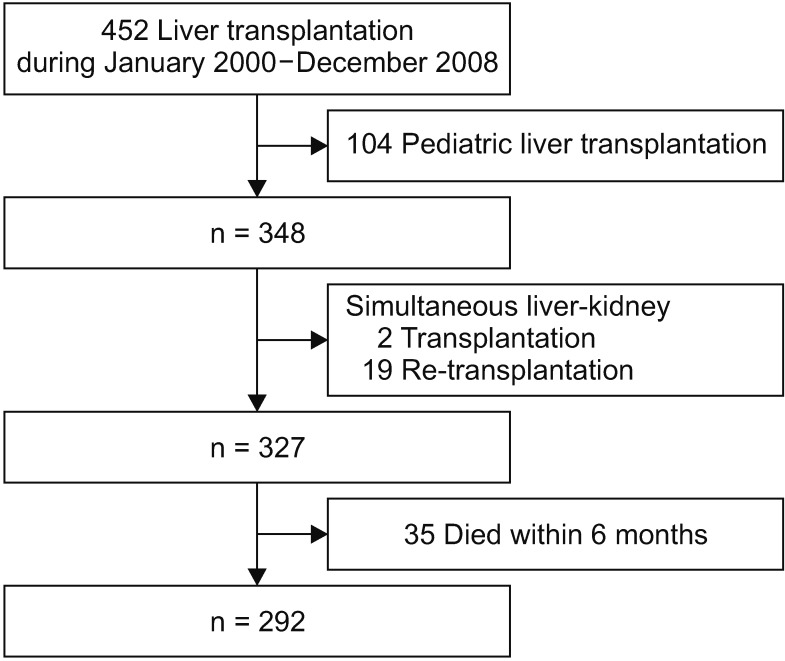
Fig. 2 The flow of study cohort.

Fig. 3 Time-dependent changes in eGFR according to the risk factors in the multivariable analysis. Each dot represents average eGFR according to subgroups of patients (Bars represent standard deviation). AKI, acute kidney injury; eGFR, estimated glomerular filtration rate. *P < 0.05, compared with the reference group (t-test).
Reference
-
1. Thongprayoon C, Kaewput W, Thamcharoen N, Bathini T, Watthanasuntorn K, Lertjitbanjong P, et al. Incidence and impact of acute kidney injury after liver transplantation: a meta-analysis. J Clin Med. 2019; 8:372.2. Bahirwani R, Reddy KR. Outcomes after liver transplantation: chronic kidney disease. Liver Transpl. 2009; 15 Suppl 2:S70–S74. PMID: 19876956.3. Ojo AO, Held PJ, Port FK, Wolfe RA, Leichtman AB, Young EW, et al. Chronic renal failure after transplantation of a nonrenal organ. N Engl J Med. 2003; 349:931–940. PMID: 12954741.4. Kim HY, Lee JE, Ko JS, Gwak MS, Lee SK, Kim GS. Intraoperative management of liver transplant recipients having severe renal dysfunction: results of 42 cases. Ann Surg Treat Res. 2018; 95:45–53. PMID: 29963539.5. Chen J, Singhapricha T, Hu KQ, Hong JC, Steadman RH, Busuttil RW, et al. Postliver transplant acute renal injury and failure by the RIFLE criteria in patients with normal pretransplant serum creatinine concentrations: a matched study. Transplantation. 2011; 91:348–353. PMID: 21127462.6. Utsumi M, Umeda Y, Sadamori H, Nagasaka T, Takaki A, Matsuda H, et al. Risk factors for acute renal injury in living donor liver transplantation: evaluation of the RIFLE criteria. Transpl Int. 2013; 26:842–852. PMID: 23855657.7. Hilmi IA, Damian D, Al-Khafaji A, Planinsic R, Boucek C, Sakai T, et al. Acute kidney injury following orthotopic liver transplantation: incidence, risk factors, and effects on patient and graft outcomes. Br J Anaesth. 2015; 114:919–926. PMID: 25673576.8. Leithead JA, Ferguson JW, Bates CM, Davidson JS, Simpson KJ, Hayes PC. Chronic kidney disease after liver transplantation for acute liver failure is not associated with perioperative renal dysfunction. Am J Transplant. 2011; 11:1905–1915. PMID: 21827620.9. Rana A, Petrowsky H, Hong JC, Agopian VG, Kaldas FM, Farmer D, et al. Blood transfusion requirement during liver transplantation is an important risk factor for mortality. J Am Coll Surg. 2013; 216:902–907. PMID: 23478547.10. Richer M, Robert S, Lebel M. Renal hemodynamics during norepinephrine and low-dose dopamine infusions in man. Crit Care Med. 1996; 24:1150–1156. PMID: 8674327.11. Levey AS, Coresh J, Greene T, Stevens LA, Zhang YL, Hendriksen S, et al. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006; 145:247–254. PMID: 16908915.12. Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007; 11:R31. PMID: 17331245.13. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002; 39(2 Suppl 1):S1–S266. PMID: 11904577.14. Bang SR, Ahn HJ, Kim GS, Yang M, Gwak MS, Ko JS, et al. Predictors of high intraoperative blood loss derived by simple and objective method in adult living donor liver transplantation. Transplant Proc. 2010; 42:4148–4150. PMID: 21168648.15. Zuppa AF, Nadkarni V, Davis L, Adamson PC, Helfaer MA, Elliott MR, et al. The effect of a thyroid hormone infusion on vasopressor support in critically ill children with cessation of neurologic function. Crit Care Med. 2004; 32:2318–2322. PMID: 15640648.16. Olthoff KM, Kulik L, Samstein B, Kaminski M, Abecassis M, Emond J, et al. Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transpl. 2010; 16:943–949. PMID: 20677285.17. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007; 370:1453–1457. PMID: 18064739.18. Saliba F, Fischer L, de Simone P, Bernhardt P, Bader G, Fung J. Association between renal dysfunction and major adverse cardiac events after liver transplantation: evidence from an Internat ional Randomized Trial of Everolimus-Based Immunosuppression. Ann Transplant. 2018; 23:751–757. PMID: 30361470.19. Yilmaz S, Yilmaz A, Häyry P. Chronic renal allograft rejection can be predicted by area under the serum creatinine versus time curve (AUCCr). Kidney Int. 1995; 48:251–258. PMID: 7564086.20. Coresh J, Turin TC, Matsushita K, Sang Y, Ballew SH, Appel LJ, et al. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA. 2014; 311:2518–2531. PMID: 24892770.21. Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, Plattner B, et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013; 382:260–272. PMID: 23727169.22. Rifkin DE, Coca SG, Kalantar-Zadeh K. Does AKI truly lead to CKD? J Am Soc Nephrol. 2012; 23:979–984. PMID: 22460531.23. Basile DP, Donohoe D, Roethe K, Osborn JL. Renal ischemic injury results in permanent damage to peritubular capillaries and influences long-term function. Am J Physiol Renal Physiol. 2001; 281:F887–F899. PMID: 11592947.24. Basile DP, Leonard EC, Tonade D, Friedrich JL, Goenka S. Distinct effects on long-term function of injured and contralateral kidneys following unilateral renal ischemia-reperfusion. Am J Physiol Renal Physiol. 2012; 302:F625–F635. PMID: 22114210.25. Northup PG, Argo CK, Bakhru MR, Schmitt TM, Berg CL, Rosner MH. Pretransplant predictors of recovery of renal function after liver transplantation. Liver Transpl. 2010; 16:440–446. PMID: 20205164.26. Bucaloiu ID, Kirchner HL, Norfolk ER, Hartle JE 2nd, Perkins RM. Increased risk of death and de novo chronic kidney disease following reversible acute kidney injury. Kidney Int. 2012; 81:477–485. PMID: 22157656.27. Kellum JA. Persistent acute kidney injury. Crit Care Med. 2015; 43:1785–1786. PMID: 26181122.28. Xia VW, Du B, Braunfeld M, Neelakanta G, Hu KQ, Nourmand H, et al. Preoperative characteristics and intraoperative transfusion and vasopressor requirements in patients with low vs. high MELD scores. Liver Transpl. 2006; 12:614–620. PMID: 16555319.29. Bellomo R, Wan L, May C. Vasoactive drugs and acute kidney injury. Crit Care Med. 2008; 36(4 Suppl):S179–S186. PMID: 18382191.30. Bijker JB, van Klei WA, Kappen TH, van Wolfswinkel L, Moons KG, Kalkman CJ. Incidence of intraoperative hypotension as a function of the chosen definition: literature definitions applied to a retrospective cohort using automated data collection. Anesthesiology. 2007; 107:213–220. PMID: 17667564.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Risk Factors and Natural History of Chronic Kidney Disease in Liver Transplant Recipients
- Incidence of Post-transplant Malignancy after Renal Transplantation: Single Center Analysis
- Risk Factors for the Progression of Chronic Kidney Disease in Children
- Cause-specific mortality and associated factors related to death after kidney and liver transplantation: a Korean nationwide study
- Study on patients without underlying chronic liver disease to improve survival outcome in pediatric liver transplantation
