Three-Dimensional Flexible Endoscopy Can Facilitate Efficient and Reliable Endoscopic Hand Suturing: An ex-vivo Study
- Omori J
 1
1 - Goto O1
- Higuchi K1
- Umeda T1
- Akimoto N1
- Suzuki M1
- Kirita K1
- Koizumi E1
- Noda H1
- Akimoto T1
- Kaise M1
- Iwakiri K1
- Affiliations
-
- 1Department of Gastroenterology, Nippon Medical School, Graduate School of Medicine, Tokyo, Japan
- KMID: 2502768
- DOI: http://doi.org/10.5946/ce.2019.207
Abstract
- Background/Aims
Three-dimensional (3D) flexible endoscopy, a new imaging modality that provides a stereoscopic view, can facilitate endoscopic hand suturing (EHS), a novel intraluminal suturing technique. This ex-vivo pilot study evaluated the usefulness of 3D endoscopy in EHS.
Methods
Four endoscopists (two certified, two non-certified) performed EHS in six sessions on a soft resin pad. Each session involved five stitches, under alternating 3D and two-dimensional (2D) conditions. Suturing time (sec/session), changes in suturing time, and accuracy of suturing were compared between 2D and 3D conditions.
Results
The mean suturing time was shorter in 3D than in 2D (9.8±3.4 min/session vs. 11.2±5.1 min/session) conditions and EHS was completed faster in 3D conditions, particularly by non-certified endoscopists. The suturing speed increased as the 3D sessions progressed. Error rates (failure to grasp the needle, failure to thread the needle, and puncture retrial) in the 3D condition were lower than those in the 2D condition, whereas there was no apparent difference in deviation distance.
Conclusions
3D endoscopy may contribute to increasing the speed and accuracy of EHS in a short time period. Stereoscopic viewing during 3D endoscopy may help in efficient skill acquisition for EHS, particularly among novice endoscopists.
Figure
-
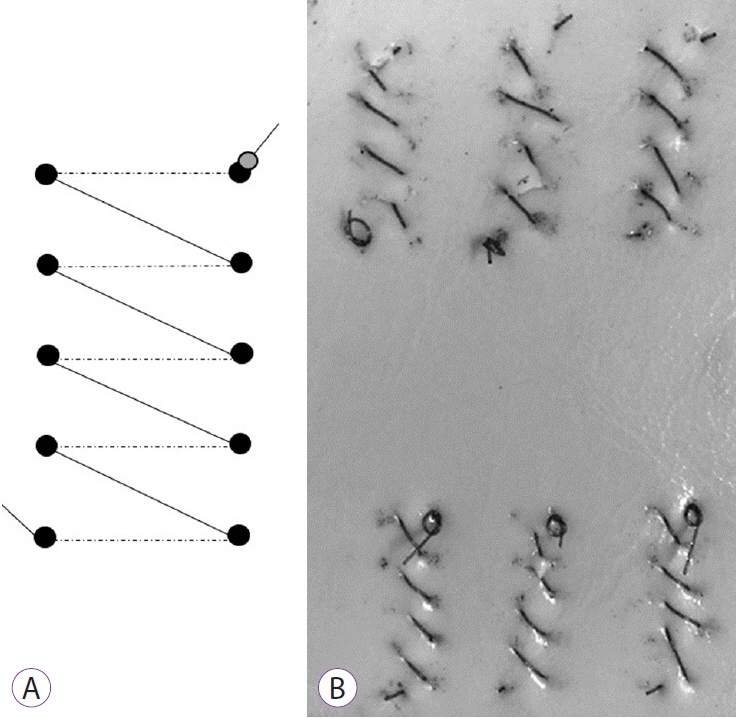
Fig. 1. Ex-vivo settings of endoscopic hand suturing. (A) Locations of the markings on the urethane pad. Five markings at 5-mm intervals are linearly placed in both the right and left rows. (B) The pad after suturing. The suture needle is inserted from the marking point on the right row and pulled out from the marking point on the left row; this suturing is repeated five times per session.
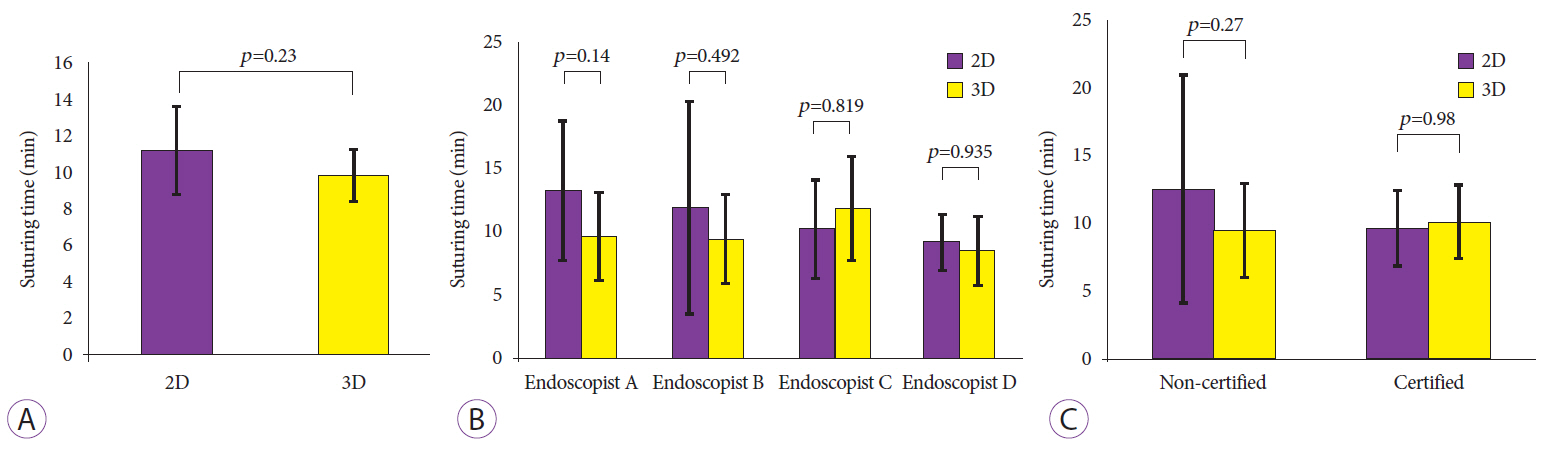
Fig. 2. Suturing time during endoscopic hand suturing (EHS). (A) Comparison of suturing time (min/session) between two-dimensional (2D) and three-dimensional (3D) endoscopy showing a shorter time in 3D. (B) Comparison of suturing time for each endoscopist. (C) Among non-certified participants, EHS is completed faster in 3D than in 2D. Bar: 95% confidence interval.
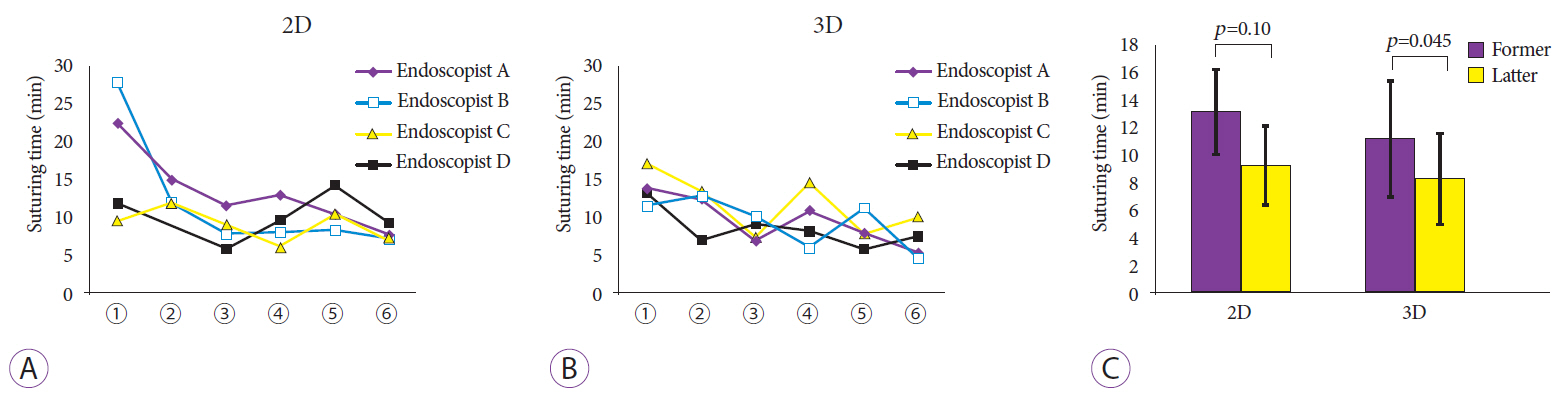
Fig. 3. Changes in suturing time. (A) Under two-dimensional (2D) conditions, the suturing time per session tends to decrease as the study proceeded. (B) The time also decreases in the three-dimensional (3D) condition, although the magnitude of change is less than that seen under 2D conditions. (C) Comparison of suturing times in the former and latter halves of the suture sessions showing a reduced time in the 3D condition. Bar: 95% confidence interval.
Reference
-
1. Goto O, Sasaki M, Ishii H, et al. A new endoscopic closure method for gastric mucosal defects: feasibility of endoscopic hand suturing in an ex vivo porcine model (with video). Endosc Int Open. 2014; 2:E111–E116.
Article2. Goto O, Sasaki M, Akimoto T, et al. Endoscopic hand-suturing for defect closure after gastric endoscopic submucosal dissection: a pilot study in animals and in humans. Endoscopy. 2017; 49:792–797.
Article3. Becker H, Melzer A, Schurr MO, Buess G. 3-D video techniques in endoscopic surgery. Endosc Surg Allied Technol. 1993; 1:40–46.4. Fergo C, Burcharth J, Pommergaard HC, Kildebro N, Rosenberg J. Three-dimensional laparoscopy vs 2-dimensional laparoscopy with high-definition technology for abdominal surgery: a systematic review. Am J Surg. 2017; 213:159–170.
Article5. Nomura K, Kaise M, Kikuchi D, et al. Recognition accuracy using 3D endoscopic images for superficial gastrointestinal cancer: a crossover study. Gastroenterol Res Pract. 2016; 2016:4561468.
Article6. Nomura K, Kaise M, Kikuchi D, et al. Recognition accuracy of tumor extent using a prototype 3D endoscope for superficial gastric tumor: an ex vivo crossover study. Endosc Int Open. 2018; 6:E652–E658.
Article7. Kikuchi D, Kaise M, Nomura K, et al. Feasibility study of the three-dimensional flexible endoscope in endoscopic submucosal dissection: an ex vivo animal study. Digestion. 2017; 95:237–241.
Article8. Nomura K, Kikuchi D, Kaise M, et al. Comparison of 3D endoscopy and conventional 2D endoscopy in gastric endoscopic submucosal dissection: an ex vivo animal study. Surg Endosc. 2019; 33:4164–4170.
Article9. Akizue N, Matsumura T, Maruoka D, et al. Novel three-dimensional imaging system may facilitate gastric endoscopic submucosal dissection procedure: an ex vivo animal study. Endosc Int Open. 2018; 6:E1431–E1435.
Article10. Sakata S, Grove PM, Hill A, Watson MO, Stevenson ARL. Impact of simulated three-dimensional perception on precision of depth judgements, technical performance and perceived workload in laparoscopy. Br J Surg. 2017; 104:1097–1106.
Article11. Blavier A, Gaudissart Q, Cadière GB, Nyssen AS. Comparison of learning curves and skill transfer between classical and robotic laparoscopy according to the viewing conditions: implications for training. Am J Surg. 2007; 194:115–121.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The development of robotic flexible endoscopic platforms
- Successive Suture Device for Gastrointestinal Endoscopes
- Flexible endoscopic treatment of Zenker’s diverticulum: a retrospective study in a single center from Turkey
- Endoscopic Submucosal Dissection (ESD) Training and Performing ESD with Accurate and Safe Techniques
- Review of Pure Endoscopic Full-Thickness Resection of the Upper Gastrointestinal Tract
