Clin Exp Otorhinolaryngol.
2020 Feb;13(1):69-76. 10.21053/ceo.2019.00388.
Evaluation of Prognostic Factors for the Parotid Cancer Treated With Surgery and Postoperative Radiotherapy
- Affiliations
-
- 1Department of Radiation Oncology, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Hwasun, Korea
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Chonnam National University Hwasun Hospital, Chonnam National University Medical School, Hwasun, Korea
- KMID: 2501301
- DOI: http://doi.org/10.21053/ceo.2019.00388
Abstract
Objectives
. To investigate the prognostic factors and treatment outcomes of primary parotid carcinoma treated with surgery and postoperative radiotherapy (PORT).
Methods
. We reviewed retrospectively 57 patients with primary parotid carcinoma who were treated with surgery and PORT between 2005 and 2014. Superficial parotidectomy was performed in 19 patients, total parotidectomy in 10 patients, and total parotidectomy with lymph node dissection in 28 patients PORT on the tumor bed was performed in 41 patients, while PORT on tumor bed and ipsilateral cervical lymph nodes was performed in 16 patients.
Results
. With a median follow-up of 66 months, the 5-year overall survival, disease-free survival, locoregional control, and distant control rates were 77.0%, 60.2%, 77.6%, and 72.8%, respectively. The 5-year overall survival by stage was 100%, 100%, 80.0%, and 46.4% in stage I, II, III, and IV, respectively. Recurrences at primary lesions were found in seven patients, while at cervical nodes in six patients. Distant recurrences were developed in 12 patients. No patient with the low and intermediate histologic grade developed distant failure. As prognostic factors, the histologic grade for overall survival (P=0.005), pathological T-stage (P=0.009) and differentiation grade (P=0.009) for disease-free survival, pathological T-stage for locoregional control (P=0.007), and lympho-vascular invasion (P=0.023) for distant recurrence were significant on multivariate analysis.
Conclusion
. This study revealed that differentiation grade, histologic grade, pathological T-stage, and lympho-vascular invasion were significant independent prognostic factors on clinical outcomes.
Figure
-
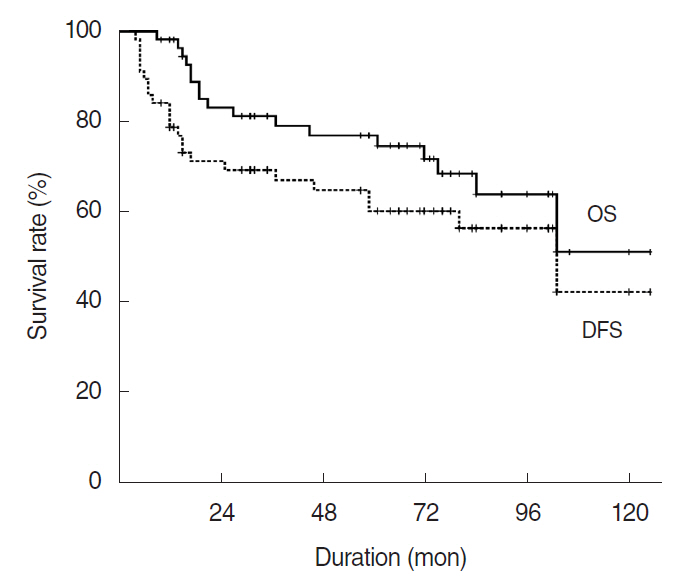
Fig. 1. Overall survival (OS) and disease-free survival (DFS) rates for 57 patients with parotid gland carcinoma.
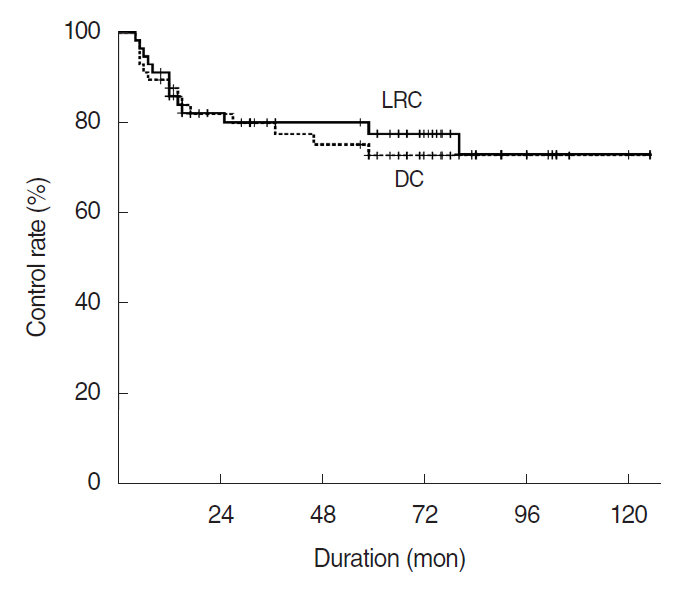
Fig. 2. Locoregional control (LRC) and distant control (DC) rates for 57 patients with parotid gland carcinoma.
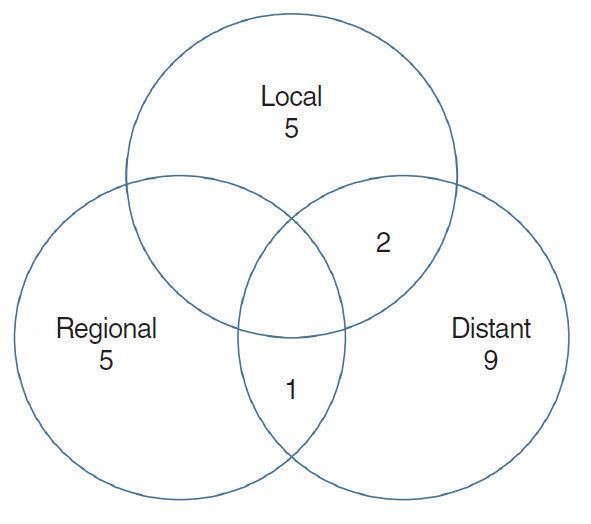
Fig. 3. Treatment failure patterns after postoperative radiotherapy with parotid gland carcinoma. Of 22 patients of failures, seven (12.3%) of local, six (10.5%) of regional, and 12 (21.1%) of distant failure were observed, respectively.
Cited by 1 articles
-
Optimal Treatment for the High-Risk Salivary Gland Cancer
Jeong-Soo Woo
Clin Exp Otorhinolaryngol. 2020;13(1):6-7. doi: 10.21053/ceo.2019.01907.
Reference
-
1. Calearo C, Pastore A, Storchi OF, Polli G. Parotid gland carcinoma: analysis of prognostic factors. Ann Otol Rhinol Laryngol. 1998; Nov. 107(11 Pt 1):969–73.
Article2. Lewis AG, Tong T, Maghami E. Diagnosis and management of malignant salivary gland tumors of the parotid gland. Otolaryngol Clin North Am. 2016; Apr. 49(2):343–80.
Article3. Terhaard CH, Lubsen H, Van der Tweel I, Hilgers FJ, Eijkenboom WM, Marres HA, et al. Salivary gland carcinoma: independent prognostic factors for locoregional control, distant metastases, and overall survival: results of the Dutch head and neck oncology cooperative group. Head Neck. 2004; Aug. 26(8):681–92.
Article4. Terhaard CH, Lubsen H, Rasch CR, Levendag PC, Kaanders HH, Tjho-Heslinga RE, et al. The role of radiotherapy in the treatment of malignant salivary gland tumors. Int J Radiat Oncol Biol Phys. 2005; Jan. 61(1):103–11.
Article5. Jeannon JP, Calman F, Gleeson M, McGurk M, Morgan P, O’Connell M, et al. Management of advanced parotid cancer: a systematic review. Eur J Surg Oncol. 2009; Sep. 35(9):908–15.
Article6. Noh JM, Ahn YC, Nam H, Park W, Baek CH, Son YI, et al. Treatment results of major salivary gland cancer by surgery with or without postoperative radiation therapy. Clin Exp Otorhinolaryngol. 2010; Jun. 3(2):96–101.
Article7. Stennert E, Kisner D, Jungehuelsing M, Guntinas-Lichius O, Schroder U, Eckel HE, et al. High incidence of lymph node metastasis in major salivary gland cancer. Arch Otolaryngol Head Neck Surg. 2003; Jul. 129(7):720–3.
Article8. Chen AM, Garcia J, Lee NY, Bucci MK, Eisele DW. Patterns of nodal relapse after surgery and postoperative radiation therapy for carcinomas of the major and minor salivary glands: what is the role of elective neck irradiation. Int J Radiat Oncol Biol Phys. 2007; Mar. 67(4):988–94.
Article9. Ali S, Palmer FL, DiLorenzo M, Shah JP, Patel SG, Ganly I. Treatment of the neck in carcinoma of the parotid gland. Ann Surg Oncol. 2014; Sep. 21(9):3042–8.
Article10. Lau VH, Aouad R, Farwell DG, Donald PJ, Chen AM. Patterns of nodal involvement for clinically N0 salivary gland carcinoma: refining the role of elective neck irradiation. Head Neck. 2014; Oct. 36(10):1435–9.
Article11. Shinomiya H, Otsuki N, Yamashita D, Nibu K. Patterns of lymph node metastasis of parotid cancer. Auris Nasus Larynx. 2016; Aug. 43(4):446–50.
Article12. Terhaard CH. Postoperative and primary radiotherapy for salivary gland carcinomas: indications, techniques, and results. Int J Radiat Oncol Biol Phys. 2007; 69(2 Suppl):S52–5.
Article13. Ettl T, Schwarz-Furlan S, Gosau M, Reichert TE. Salivary gland carcinomas. Oral Maxillofac Surg. 2012; Sep. 16(3):267–83.
Article14. Cox JD, Stetz J, Pajak TF. Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys. 1995; Mar. 31(5):1341–6.
Article15. Chen AM, Granchi PJ, Garcia J, Bucci MK, Fu KK, Eisele DW. Localregional recurrence after surgery without postoperative irradiation for carcinomas of the major salivary glands: implications for adjuvant therapy. Int J Radiat Oncol Biol Phys. 2007; Mar. 67(4):982–7.
Article16. Garden AS, el-Naggar AK, Morrison WH, Callender DL, Ang KK, Peters LJ. Postoperative radiotherapy for malignant tumors of the parotid gland. Int J Radiat Oncol Biol Phys. 1997; Jan. 37(1):79–85.
Article17. Mendenhall WM, Morris CG, Amdur RJ, Werning JW, Villaret DB. Radiotherapy alone or combined with surgery for salivary gland carcinoma. Cancer. 2005; Jun. 103(12):2544–50.
Article18. Al-Mamgani A, van Rooij P, Verduijn GM, Meeuwis CA, Levendag PC. Long-term outcomes and quality of life of 186 patients with primary parotid carcinoma treated with surgery and radiotherapy at the Daniel den Hoed Cancer Center. Int J Radiat Oncol Biol Phys. 2012; Sep. 84(1):189–95.
Article19. Schoenfeld JD, Sher DJ, Norris CM Jr, Haddad RI, Posner MR, Balboni TA, et al. Salivary gland tumors treated with adjuvant intensity-modulated radiotherapy with or without concurrent chemotherapy. Int J Radiat Oncol Biol Phys. 2012; Jan. 82(1):308–14.
Article20. Amini A, Waxweiler TV, Brower JV, Jones BL, McDermott JD, Raben D, et al. Association of adjuvant chemoradiotherapy vs radiotherapy alone with survival in patients with resected major salivary gland carcinoma: data from the national cancer data base. JAMA Otolaryngol Head Neck Surg. 2016; Nov. 142(11):1100–10.21. Hsieh CE, Lin CY, Lee LY, Yang LY, Wang CC, Wang HM, et al. Adding concurrent chemotherapy to postoperative radiotherapy improves locoregional control but not overall survival in patients with salivary gland adenoid cystic carcinoma: a propensity score matched study. Radiat Oncol. 2016; Mar. 11:47.
Article22. Mifsud MJ, Tanvetyanon T, Mccaffrey JC, Otto KJ, Padhya TA, Kish J, et al. Adjuvant radiotherapy versus concurrent chemoradiotherapy for the management of high-risk salivary gland carcinomas. Head Neck. 2016; Nov. 38(11):1628–33.
Article23. Therkildsen MH, Christensen M, Andersen LJ, Schiodt T, Hansen HS. Salivary gland arcinomas: prognostic factors. Acta Oncol. 1998; 37(7-8):701–13.24. National Comprehensive Cancer Network. Head and Neck Cancer Cancers: v1.2018 [Internet]. Plymouth Meeting, PA: National Comprehensive Cancer Network;2018. [cited 2019 Aug 1]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.25. Ali S, Palmer FL, Yu C, DiLorenzo M, Shah JP, Kattan MW, et al. A predictive nomogram for recurrence of carcinoma of the major salivary glands. JAMA Otolaryngol Head Neck Surg. 2013; Jul. 139(7):698–705.26. Kim JY, Lee S, Cho KJ, Kim SY, Nam SY, Choi SH, et al. Treatment results of post-operative radiotherapy in patients with salivary duct carcinoma of the major salivary glands. Br J Radiol. 2012; Oct. 85(1018):e947–52.
Article27. Mariano FV, da Silva SD, Chulan TC, de Almeida OP, Kowalski LP. Clinicopathological factors are predictors of distant metastasis from major salivary gland carcinomas. Int J Oral Maxillofac Surg. 2011; May. 40(5):504–9.
Article28. Poorten VV, Meulemans J, Delaere P, Nuyts S, Clement P. Molecular markers and chemotherapy for advanced salivary cancer. Curr Otorhinolaryngol Rep. 2014; Jun. 2(2):85–96.
Article29. Schmitt NC, Kang H, Sharma A. Salivary duct carcinoma: an aggressive salivary gland malignancy with opportunities for targeted therapy. Oral Oncol. 2017; Nov. 74:40–8.
Article30. Mukaigawa T, Hayashi R, Hashimoto K, Ugumori T, Hato N, Fujii S. Programmed death ligand-1 expression is associated with poor disease free survival in salivary gland carcinomas. J Surg Oncol. 2016; Jul. 114(1):36–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Facial Nerve Graft in Parotid Malignancy
- A Case of Metachronous Carcinosarcoma and Squamous Cell Carcinoma of the Both Parotid Glands
- Eosinophilic, Polymorphic, and Pruritic Eruption Associated with Radiotherapy in a Patient with Parotid Gland Cancer
- Radiation Therapy in Malignant Tumors of the Parotid Gland
- The Study of Prognostic Factor of the Parotid Tumor
