Incidental Diagnosis of Pediatric Arytenoid Cartilage Dislocation During Videofluoroscopic Swallowing Study: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea
- 2Department of Rehabilitation Medicine, Seoul Rehabilitation Hospital, Seoul, Korea
- KMID: 2501051
- DOI: http://doi.org/10.5535/arm.2020.44.1.94
Abstract
- Arytenoid cartilage dislocation is one of the most common mechanical causes of vocal fold immobility. The most common etiologies are intubation and external trauma, but its incidence is lower than 0.1%. Its symptoms include dysphonia, vocal fatigue, loss of vocal control, breathiness, odynophagia, dysphagia, dyspnea, and cough. Although there are some reports of arytenoid cartilage dislocation in adults, there are only few reports on its occurrence in children. It is particularly difficult to detect the symptoms of arytenoid cartilage dislocation in uncooperative pediatric patients with brain lesions without verbal output or voluntary expression. We report a case of arytenoid cartilage dislocation with incidental findings in a videofluoroscopic swallowing study performed to evaluate the swallowing function.
Figure
-
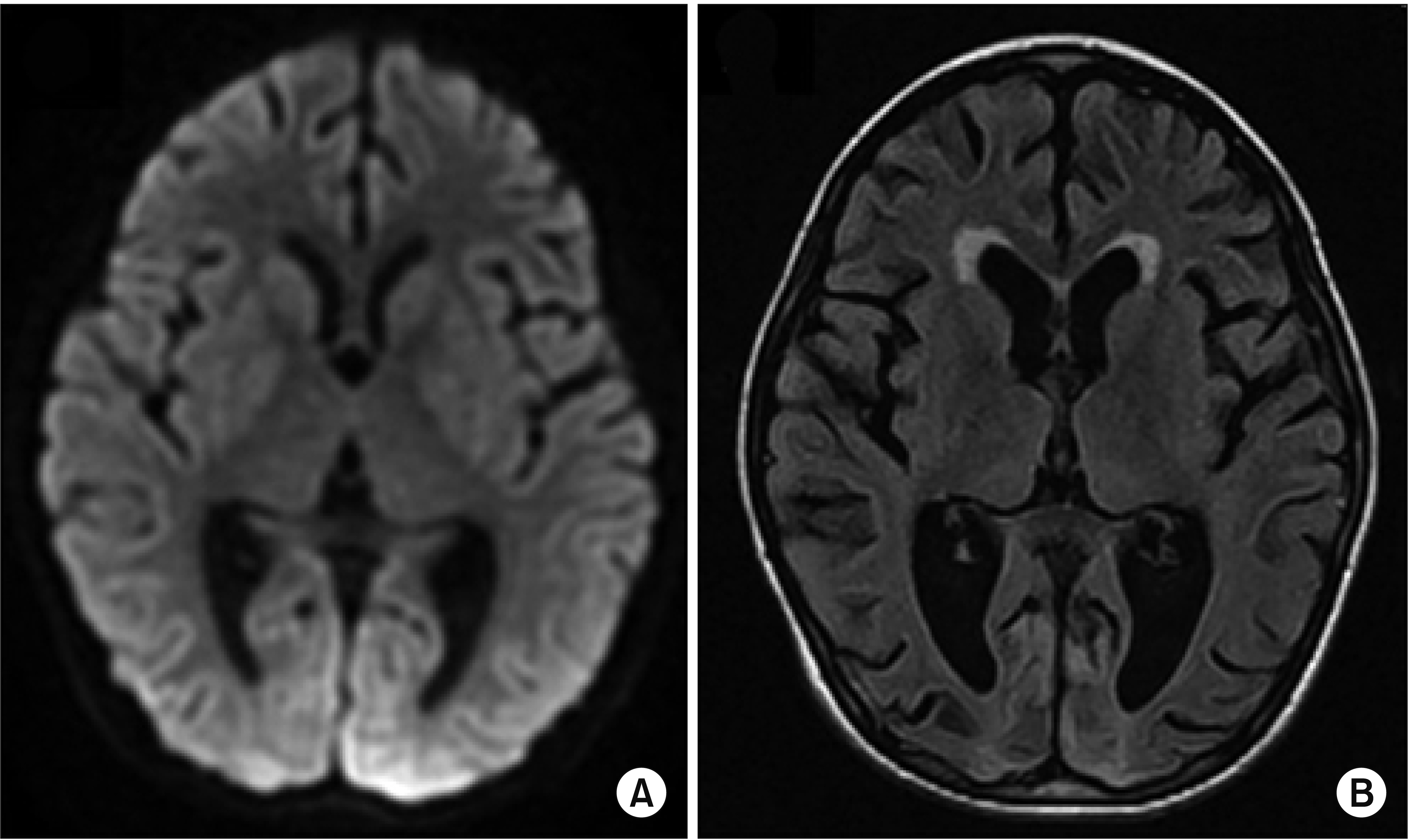
Fig. 1. A diffusion-weighted magnetic resonance imaging images taken 2 weeks after the event showed increased signal intensity in bilateral occipital lobes, thalamus and basal ganglia (A). A T2-weighted FLAIR image taken 3 months after the event showed diffused cerebral atrophy of thalamus and basal ganglia, and encephalomalacia of bilateral occipital lobes (B).

Fig. 2. The arytenoid cartilage in the videofluoroscopic swallowing study (VFSS) shows airway obstruction during inspiration (A) and opening during expiration (B). After 1 month of observation, the anterior dislocation of arytenoid cartilage was alleviated on the VFSS (C).
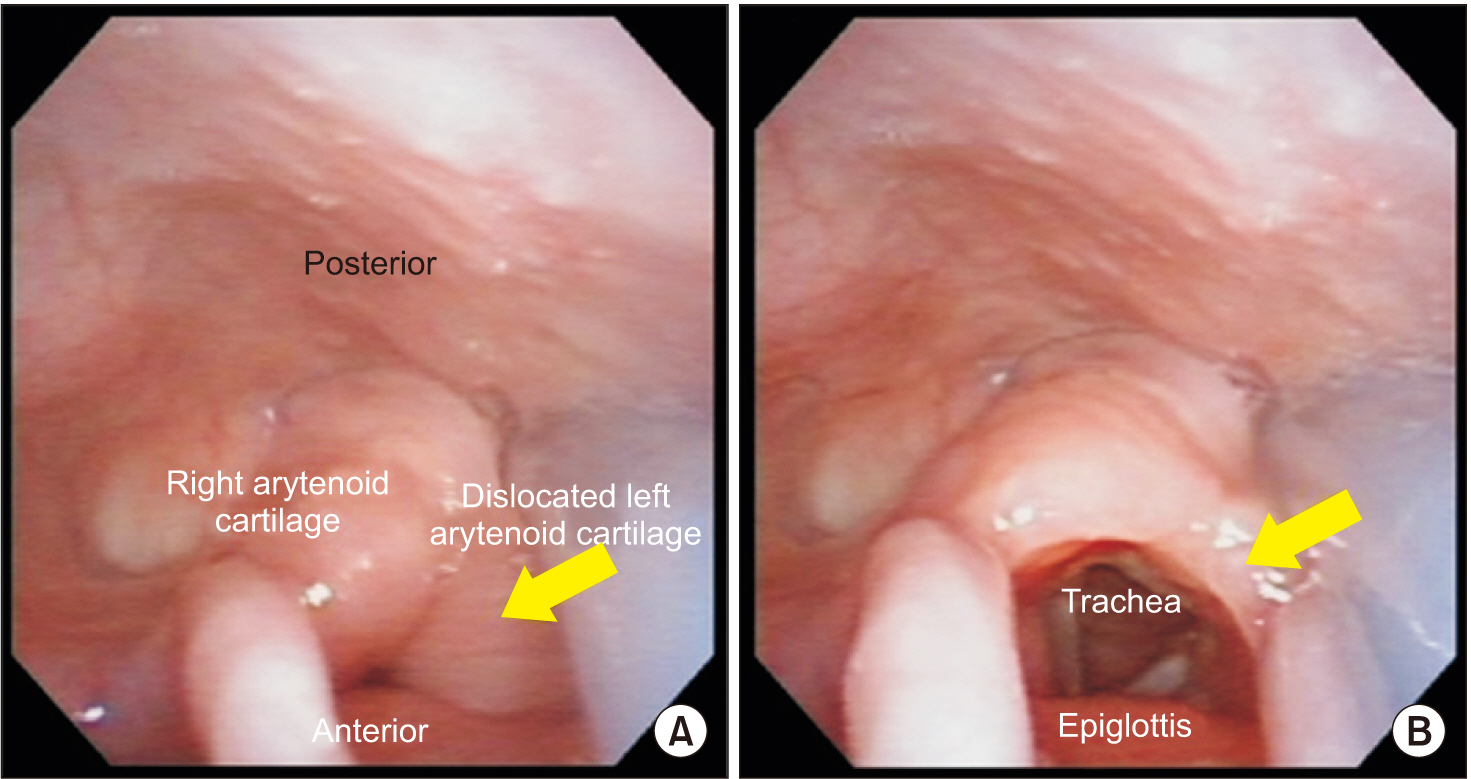
Fig. 3. On the laryngoscope, anterior dislocation of arytenoid cartilage (arrow) during inspiration induces airway obstruction (A) and opening during expiration (B).
Reference
-
1. Rubin AD, Hawkshaw MJ, Moyer CA, Dean CM, Sataloff RT. Arytenoid cartilage dislocation: a 20-year experience. J Voice. 2005; 19:687–701.
Article2. Szigeti CL, Baeuerle JJ, Mongan PD. Arytenoid dislocation with lighted stylet intubation: case report and retrospective review. Anesth Analg. 1994; 78:185–6.3. Yamanaka H, Hayashi Y, Watanabe Y, Uematu H, Mashimo T. Prolonged hoarseness and arytenoid cartilage dislocation after tracheal intubation. Br J Anaesth. 2009; 103:452–5.
Article4. Close LG, Merkel M, Watson B, Schaefer SD. Cricoarytenoid subluxation, computed tomography, and electromyography findings. Head Neck Surg. 1987; 9:341–8.
Article5. Yin SS, Qiu WW, Stucker FJ. Value of electromyography in differential diagnosis of laryngeal joint injuries after intubation. Ann Otol Rhinol Laryngol. 1996; 105:446–51.
Article6. Dudley JP, Mancuso AA, Fonkalsrud EW. Arytenoid dislocation and computed tomography. Arch Otolaryngol. 1984; 110:483–4.
Article7. Quick CA, Merwin GE. Arytenoid dislocation. Arch Otolaryngol. 1978; 104:267–70.
Article8. Niwa Y, Nakae A, Ogawa M, Takashina M, Hagihira S, Ueyama H, et al. Arytenoid dislocation after cardiac surgery. Acta Anaesthesiol Scand. 2007; 51:1397–400.
Article9. Goz V, Qureshi S, Hecht AC. Arytenoid dislocation as a cause of prolonged hoarseness after cervical discectomy and fusion. Global Spine J. 2013; 3:47–50.
Article10. Mallon AS, Portnoy JE, Landrum T, Sataloff RT. Pediatric arytenoid dislocation: diagnosis and treatment. J Voice. 2014; 28:115–22.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Arytenoid cartilage dislocation after reversed total shoulder replacement surgery in the beach chair position: a case report
- Arytenoid dislocation after uneventful endotracheal intubation: a case report
- Swallowing and Aspiration: How Much Is Affected by the Number of Arytenoid Cartilages Remaining After Supracricoid Partial Laryngectomy?
- Dislocation of Left Arytenoid Cartilage after Endotracheal Intubation Using Light Wand: A case report
- Dysphagia after Multiple Fractures of the Neck Structures Due to Near-Hanging: A Case Report
