Anesth Pain Med.
2020 Apr;15(2):247-250. 10.17085/apm.2020.15.2.247.
Novel alternative for submental intubation - A case report -
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea
- KMID: 2500979
- DOI: http://doi.org/10.17085/apm.2020.15.2.247
Abstract
- Background
Submental intubation is commonly used during general anesthesia for maxillofacial surgeries as it provides a safe unrestricted surgical access compared to tracheostomy. During submental intubation, soft tissues and blood clots can become lodged in the endotracheal tube. To overcome this problem, we used a laparoscopic trocar. Case: A 52-year-old man with maxillofacial injury was scheduled to undergo an open reduction and internal fixation. We performed submental intubation using laparoscopic trocar, which created sufficient space for the insertion of the endotracheal tube. Unlike conventional methods, our method did not require any blunt dissection and caused significantly less soft tissue damage and required significantly less time.
Conclusions
Submental intubation with laparoscopic trocar is a one-step method and is quick and easy-to-perform technique with less complications.
Figure
-
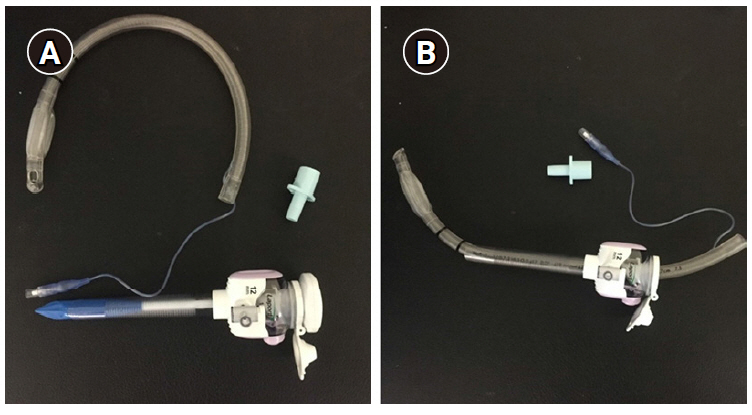
Fig. 1. (A) Removal of the armored tube connector. (B) The armored endotracheal tube (internal diameter, 7.5 mm) passes through the 12-mm diameter lumen of the laparoscopic trocar.

Fig. 2. (A) The 12-mm laparoscopic trocar is inserted in the skin-to-oral direction. (B) The tube is pulled through the passage of the trocar’s lumen.
Reference
-
1. Bähr W, Stoll P, Schilli W, Scheramet R. [Nasal intubation for frontobasal fractures?]. Dtsch Zahnarztl Z. 1992; 47:43–5. German.2. Junsanto T, Chira T. Perimortem intracranial orogastric tube insertion in a pediatric trauma patient with a basilar skull fracture. J Trauma. 1997; 42:746–7.3. Schade K, Borzotta A, Michaels A. Intracranial malposition of nasopharyngeal airway. J Trauma. 2000; 49:967–8.4. Joo DT, Orser BA. External compression of a nasotracheal tube due to the displaced bony fragments of multiple LeFort fractures. Anesthesiology. 2000; 92:1830–2.5. Sprung J, Bourke DL, Harrison C, Barnas GM. Endotracheal tube and tracheobronchial obstruction as causes of hypoventilation with high inspiratory pressures. Chest. 1994; 105:550–2.6. Ujam A, Perry M. Minimally traumatic submental intubation: a novel dilational technique. Eur J Trauma Emerg Surg. 2017; 43:359–62.7. Walker DG. Complications of tracheostomy: their prevention and treatment. J Oral Surg. 1973; 31:480–2.8. Kita R, Kikuta T, Takahashi M, Ootani T, Takaoka M, Matsuda M, et al. Efficacy and complications of submental tracheal intubation compared with tracheostomy in maxillofacial trauma patients. J Oral Sci. 2016; 58:23–8.9. de Toledo GL, Bueno SC, Mesquita RA, Amaral MB. Complications from submental endotracheal intubation: a prospective study and literature review. Dent Traumatol. 2013; 29:197–202.10. Tidke AS, Borle RM, Madan RS, Bhola ND, Jadhav AA, Bhoyar AG. Transmylohoid/submental endotracheal intubation in pan-facial trauma: a paradigm shift in airway management with prospective study of 35 cases. Indian J Otolaryngol Head Neck Surg. 2013; 65:255–9.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Submental/submandibular intubation: a journey from past to future
- Management of Detachment of Pilot Balloon During Intraoral Repositioning of the Submental Endotracheal Tube
- Modified submental intubation techniques for maxillofacial surgery - A report of five cases -
- Two Cases of Submental Endotracheal Intubation in Patients Having Multiple Facial Fractures
- Submental intubation in maxillofacial fracture: a case report
