Endoscopic Management of Iatrogenic Colon Perforation
- Affiliations
-
- 1Division of Gastroenterology, Department of Medicine, Soonchunhyang University College of Medicine, Cheonan, Korea
- KMID: 2500902
- DOI: http://doi.org/10.5946/ce.2019.061
Abstract
- Colon perforations are difficult to resolve because they occur unexpectedly and infrequently. If the clinician is unprepared or lacks training in dealing with perforations, the clinical prognosis will be affected, which can lead to legal issues. We describe here the proper approach to the management of perforations, including deciding on endoscopic or surgical treatment, selection of endoscopic devices, endoscopic closure procedures, and general management of perforations that occur during diagnostic or therapeutic colonoscopy.
Keyword
Figure
-

Fig. 1. (A) A 7-mm sessile polyp was resected using a snare. (B) A perforation was observed at the site of polypectomy. (C) Mirror target sign of the specimen.
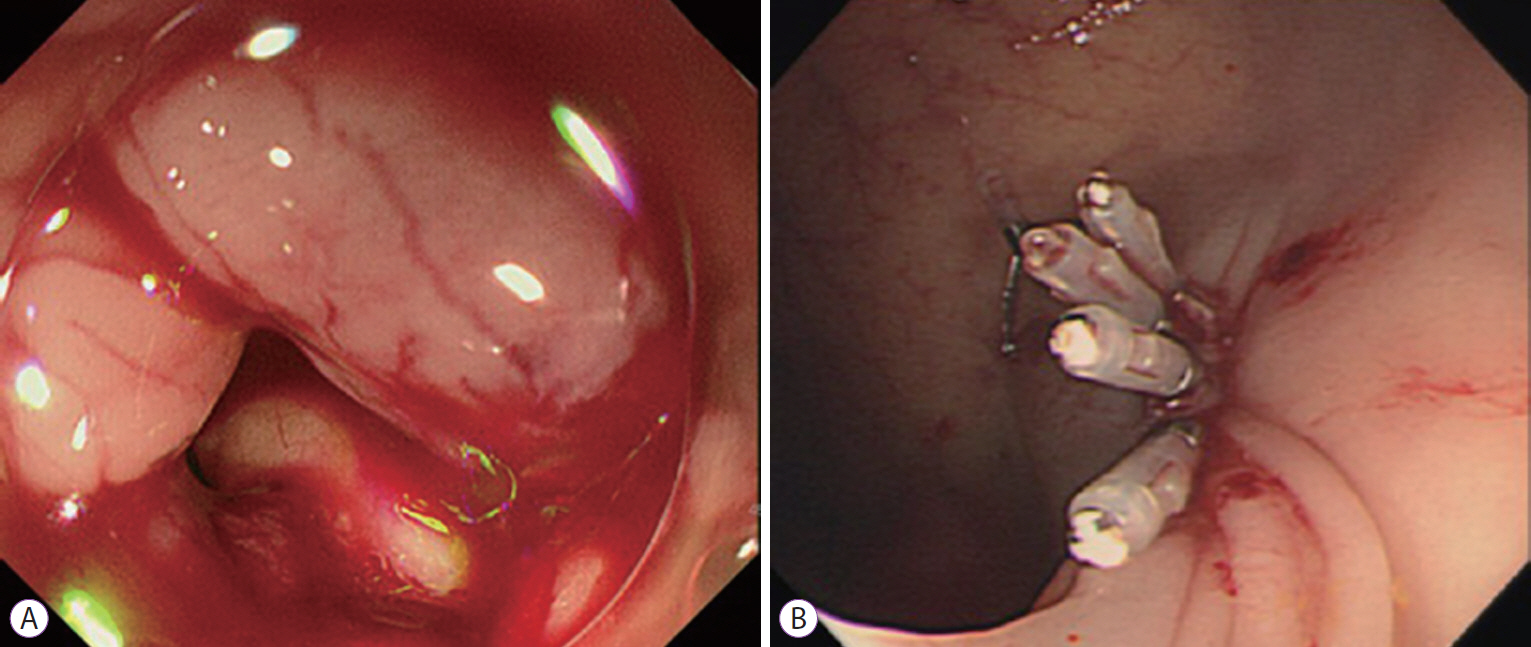
Fig. 2. (A) A 6-mm penetrating perforation occurred in the sigmoid colon during a diagnostic colonoscopy. (B) Successful closure of the perforation with hemoclips.
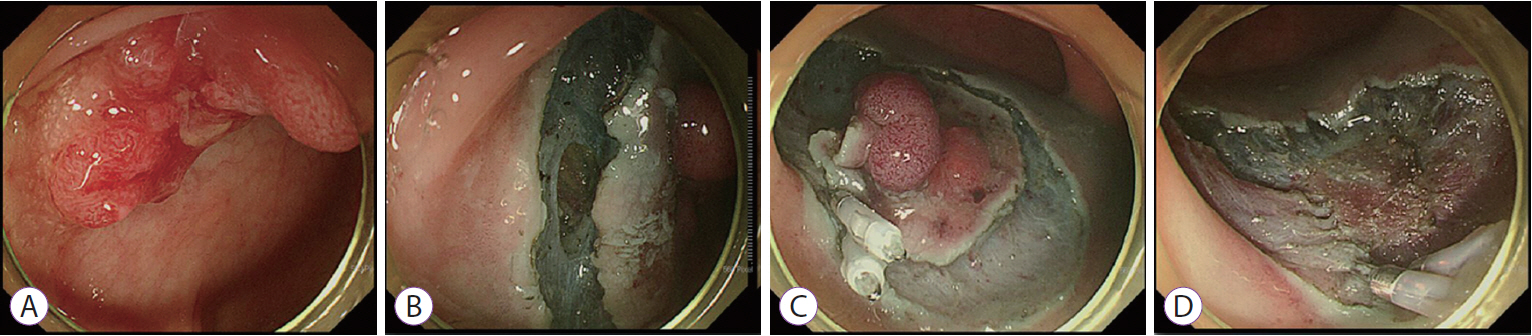
Fig. 3. (A) A 2-cm nodular mixed-type lateral spreading tumor in the rectosigmoid colon. (B) A 4-mm perforation occurred during an endoscopic submucosal dissection (ESD). (C) After further dissection of the submucosal layer, hemoclips were applied to the perforation and the circumferential incision was completed. (D) The lesion was removed using the hybrid ESD technique.
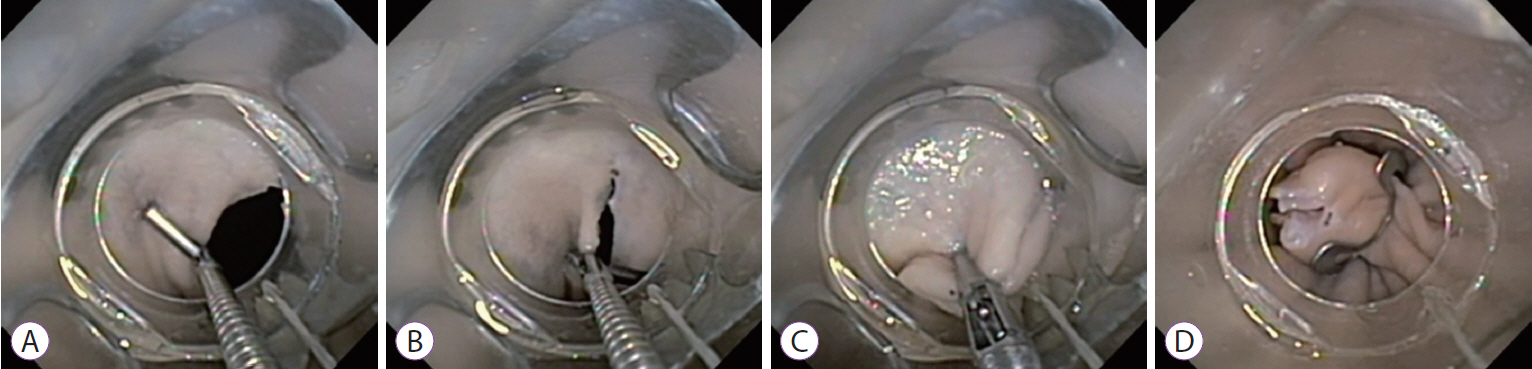
Fig. 4. (A) One of the lateral edges of the defect was grasped using one arm of the twin grasper. (B) The other edge of the defect was grasped using the second arm of the twin grasper. (C) The re-apposed tissue was pulled into the over-the-scope clip (OTSC) cap. (D) The OTSC was released by turning a wheel on the shaft of the endoscope.
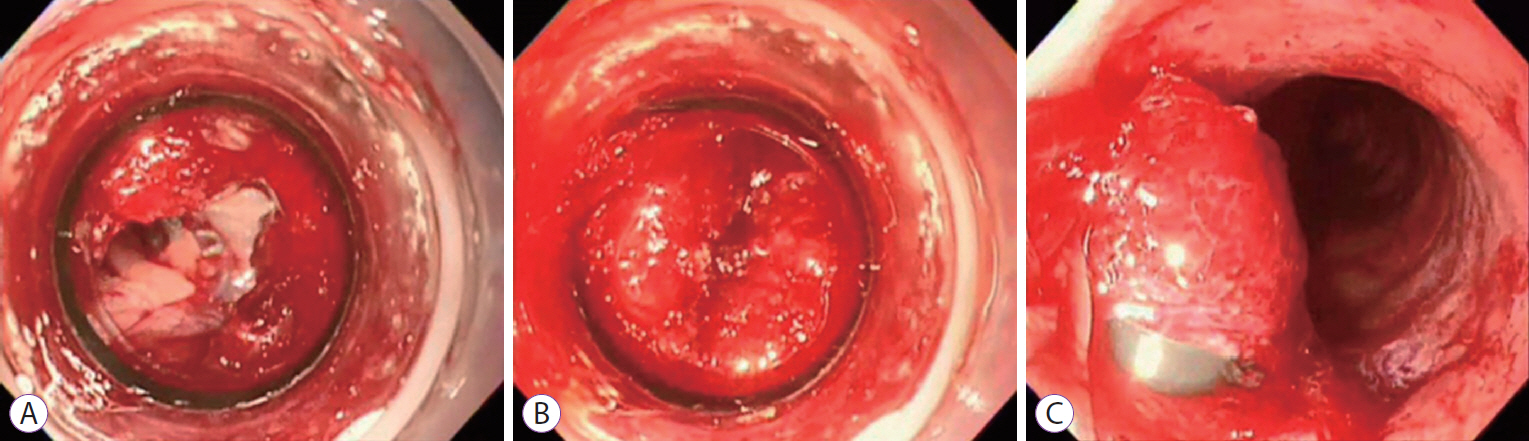
Fig. 5. (A) An approximately 7-mm perforation in the intestine. (B) The surrounding perforated tissues and the perforation were suctioned sufficiently into the banding cap until a “pink or red out sign” was observed. (C) The iatrogenic perforation was successfully closed using the band-ligation method (Adapted from Jung [19]).

Fig. 6. (A) The endoloop was placed around the perforated tissue through one channel of a double-channel endoscope. (B) Several hemoclips were applied through the other channel to fix the endoloop and surrounding perforated tissues. (C) The endoloop was tightened to close or reduce the perforation. (D) Complete closure of the perforation was achieved (Adapted from Jung [19]).
Cited by 1 articles
-
Safety of Gastrointestinal Endoscopy in Korea: A Nationwide Survey and Population-Based Study
Yunho Jung, Jung-Wook Kim, Jong Pil Im, Yu Kyung Cho, Tae Hee Lee, Jae-Young Jang
J Korean Med Sci. 2022;37(4):e24. doi: 10.3346/jkms.2022.37.e24.
Reference
-
1. Jovanovic I, Zimmermann L, Fry LC, Mönkemüller K. Feasibility of endoscopic closure of an iatrogenic colon perforation occurring during colonoscopy. Gastrointest Endosc. 2011; 73:550–555.
Article2. Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010; 71:446–454.
Article3. Reumkens A, Rondagh EJ, Bakker CM, Winkens B, Masclee AA, Sanduleanu S. Post-colonoscopy complications: a systematic review, time trends, and meta-analysis of population-based studies. Am J Gastroenterol. 2016; 111:1092–1101.
Article4. Akintoye E, Kumar N, Aihara H, Nas H, Thompson CC. Colorectal endoscopic submucosal dissection: a systematic review and meta-analysis. Endosc Int Open. 2016; 4:E1030–E1044.
Article5. Avgerinos DV, Llaguna OH, Lo AY, Leitman IM. Evolving management of colonoscopic perforations. J Gastrointest Surg. 2008; 12:1783–1789.
Article6. Iqbal CW, Cullinane DC, Schiller HJ, Sawyer MD, Zietlow SP, Farley DR. Surgical management and outcomes of 165 colonoscopic perforations from a single institution. Arch Surg. 2008; 143:701–706. discussion 706-707.
Article7. Panteris V, Haringsma J, Kuipers EJ. Colonoscopy perforation rate, mechanisms and outcome: from diagnostic to therapeutic colonoscopy. Endoscopy. 2009; 41:941–951.
Article8. Wada Y, Kudo SE, Tanaka S, et al. Predictive factors for complications in endoscopic resection of large colorectal lesions: a multicenter prospective study. Surg Endosc. 2015; 29:1216–1222.
Article9. Rutter MD, Nickerson C, Rees CJ, Patnick J, Blanks RG. Risk factors for adverse events related to polypectomy in the English Bowel Cancer Screening Programme. Endoscopy. 2014; 46:90–97.
Article10. Lee EJ, Lee JB, Choi YS, et al. Clinical risk factors for perforation during endoscopic submucosal dissection (ESD) for large-sized, nonpedunculated colorectal tumors. Surg Endosc. 2012; 26:1587–1594.
Article11. Kim ES, Cho KB, Park KS, et al. Factors predictive of perforation during endoscopic submucosal dissection for the treatment of colorectal tumors. Endoscopy. 2011; 43:573–578.
Article12. Thirumurthi S, Raju GS. Management of polypectomy complications. Gastrointest Endosc Clin N Am. 2015; 25:335–357.
Article13. Swan MP, Bourke MJ, Moss A, Williams SJ, Hopper A, Metz A. The target sign: an endoscopic marker for the resection of the muscularis propria and potential perforation during colonic endoscopic mucosal resection. Gastrointest Endosc. 2011; 73:79–85.
Article14. Yang DH, Byeon JS, Lee KH, et al. Is endoscopic closure with clips effective for both diagnostic and therapeutic colonoscopy-associated bowel perforation? Surg Endosc. 2010; 24:1177–1185.
Article15. Iqbal CW, Chun YS, Farley DR. Colonoscopic perforations: a retrospective review. J Gastrointest Surg. 2005; 9:1229–1235. discussion 1236.
Article16. Cobb WS, Heniford BT, Sigmon LB, et al. Colonoscopic perforations: incidence, management, and outcomes. Am Surg. 2004; 70:750–757. discussion 757-758.17. Anderson ML, Pasha TM, Leighton JA. Endoscopic perforation of the colon: lessons from a 10-year study. Am J Gastroenterol. 2000; 95:3418–3422.
Article18. Paspatis GA, Vardas E, Theodoropoulou A, et al. Complications of colonoscopy in a large public county hospital in Greece. A 10-year study. Dig Liver Dis. 2008; 40:951–957.
Article19. Jung Y. Management of gastrointestinal tract perforations. Gastrointestinal Intervention. 2017; 6:157–161.
Article20. Paspatis GA, Dumonceau JM, Barthet M, et al. Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) position statement. Endoscopy. 2014; 46:693–711.
Article21. Fujishiro M, Yahagi N, Kakushima N, et al. Successful nonsurgical management of perforation complicating endoscopic submucosal dissection of gastrointestinal epithelial neoplasms. Endoscopy. 2006; 38:1001–1006.
Article22. Raju GS. Endoscopic closure of gastrointestinal leaks. Am J Gastroenterol. 2009; 104:1315–1320.
Article23. Binmoeller KF, Grimm H, Soehendra N. Endoscopic closure of a perforation using metallic clips after snare excision of a gastric leiomyoma. Gastrointest Endosc. 1993; 39:172–174.
Article24. Raju GS, Ahmed I, Xiao SY, et al. Controlled trial of immediate endoluminal closure of colon perforations in a porcine model by use of a novel clip device (with videos). Gastrointest Endosc. 2006; 64:989–997.
Article25. Verlaan T, Voermans RP, van Berge Henegouwen MI, Bemelman WA, Fockens P. Endoscopic closure of acute perforations of the GI tract: a systematic review of the literature. Gastrointest Endosc. 2015; 82:618–628. e5.
Article26. Hawkins AT, Sharp KW, Ford MM, Muldoon RL, Hopkins MB, Geiger TM. Management of colonoscopic perforations: a systematic review. Am J Surg. 2018; 215:712–718.
Article27. Jung Y, Kim JW, Byeon JS, et al. Factors predictive of complete excision of large colorectal neoplasia using hybrid endoscopic submucosal dissection: a KASID multicenter study. Dig Dis Sci. 2018; 63:2773–2779.
Article28. von Renteln D, Schmidt A, Vassiliou MC, Rudolph HU, Caca K. Endoscopic full-thickness resection and defect closure in the colon. Gastrointest Endosc. 2010; 71:1267–1273.
Article29. Matthes K, Jung Y, Kato M, Gromski MA, Chuttani R. Efficacy of full-thickness GI perforation closure with a novel over-the-scope clip application device: an animal study. Gastrointest Endosc. 2011; 74:1369–1375.
Article30. von Renteln D, Vassiliou MC, Rothstein RI. Randomized controlled trial comparing endoscopic clips and over-the-scope clips for closure of natural orifice transluminal endoscopic surgery gastrotomies. Endoscopy. 2009; 41:1056–1061.
Article31. Kobara H, Mori H, Nishiyama N, et al. Over-the-scope clip system: a review of 1517 cases over 9 years. J Gastroenterol Hepatol. 2019; 34:22–30.32. Haito-Chavez Y, Law JK, Kratt T, et al. International multicenter experience with an over-the-scope clipping device for endoscopic management of GI defects (with video). Gastrointest Endosc. 2014; 80:610–622.
Article33. Voermans RP, Le Moine O, von Renteln D, et al. Efficacy of endoscopic closure of acute perforations of the gastrointestinal tract. Clin Gastroenterol Hepatol. 2012; 10:603–608.
Article34. Han JH, Park S, Youn S. Endoscopic closure of colon perforation with band ligation; salvage technique after endoclip failure. Clin Gastroenterol Hepatol. 2011; 9:e54–e55.
Article35. Yang Y, Lin X, Tan S, et al. Endoscopic band ligation is able to close perforations caused by colonoscopy: a porcine model study. Gastroenterol Res Pract. 2018; 2018:4325675.
Article36. Han JH, Kim M, Lee TH, et al. Endoluminal closure of colon perforation with endoscopic band ligation: technical feasibility and safety in an in vivo canine model. Clin Endosc. 2015; 48:534–541.37. Martínek J, Ryska O, Tuckova I, et al. Comparing over-the-scope clip versus endoloop and clips (KING closure) for access site closure: a randomized experimental study. Surg Endosc. 2013; 27:1203–1210.
Article38. Katsinelos P, Lazaraki G, Chatzimavroudis G, Zavos C. Closure of an iatrogenic rectal perforation with the endoloop/clips technique in a purse-string fashion. Ann Gastroenterol. 2014; 27:264.39. Ryu JY, Park BK, Kim WS, et al. Endoscopic closure of iatrogenic colon perforation using dual-channel endoscope with an endoloop and clips: methods and feasibility data (with videos). Surg Endosc. 2019; 33:1342–1348.
Article40. Swinnen J, Eisendrath P, Rigaux J, et al. Self-expandable metal stents for the treatment of benign upper GI leaks and perforations. Gastrointest Endosc. 2011; 73:890–899.
Article41. Kim SW, Lee WH, Kim JS, Lee HN, Kim SJ, Lee SJ. Successful management of colonic perforation with a covered metal stent. Korean J Intern Med. 2013; 28:715–717.
Article42. Cho SB, Lee WS, Joo YE, et al. Therapeutic options for iatrogenic colon perforation: feasibility of endoscopic clip closure and predictors of the need for early surgery. Surg Endosc. 2012; 26:473–479.
Article43. Taku K, Sano Y, Fu KI, et al. Iatrogenic perforation associated with therapeutic colonoscopy: a multicenter study in Japan. J Gastroenterol Hepatol. 2007; 22:1409–1414.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Successful Clipping of a Colonic Perforation during Diagnostic Colonoscopy
- A Case of Successful Endoscopic Therapy in Delayed Diagnosed Perforation after Endoscopic Colon Polypectomy
- A Case of Iatrogenic Colonic Perforation Repaired by Endoscopic Clipping
- A Case of Successful Endoscopic Therapy in Iatrogenic Perforation of the Colon during Colonoscopy
- Iatrogenic Gallbladder Perforation during Gastric Endoscopic Mucosal Resection
