Right trisectionectomy with en bloc portal vein resection for cholangiocarcinoma after preoperative stenting for main portal vein occlusion
- Affiliations
-
- 1Departments of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- 2Departments of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2500802
- DOI: http://doi.org/10.14701/ahbps.2020.24.2.174
Abstract
- Deprivation of portal blood flow decreases the hepatic function, thus hepatobiliary cancer patients with total occlusion of the main portal vein (PV) are usually not indicated for major hepatectomy. We herein present a 37-year-old male patient with advanced intrahepatic cholangiocarcinoma, in whom right trisectionectomy was indicated. However, the main PV was nearly completely occluded by tumor invasion, thus resolution of jaundice was markedly slow. To restore the liver function through PV recanalization, a wall stent was inserted percutaneously. Jaundice resolved progressively after PV stenting. Right trisectionectomy, caudate lobectomy, bile duct resection, and en bloc PV segmental resection with iliac vein homograft interposition were performed. However, PV thrombosis developed at the site of PV stent removal, thus a new wall stent was inserted during the operation. The pathology report presented that the tumor was a 5.2 cm-sized well-differentiated adenocarcinoma of periductal infiltrating type with lymph node metastasis. During the follow-up, the interposed PV segment with a wall stent was gradually occluded with development of portal collaterals. At 5 years after surgery, the PV stent was completely occluded and collaterals developed. The patient experienced repetition of febrile episodes of unknown causes. He is currently alive for 8 years with no evidence of tumor recurrence. The detailed surgical procedures were presented with a supplementary video clip of 5 minutes.
Figure
-

Fig. 1 Preoperative computed tomography findings. The portal vein was invaded by the tumor (A and B), progressively occluded (C), and expanded after stent insertion (D). Arrows indicate the sites of portal vein invasion.
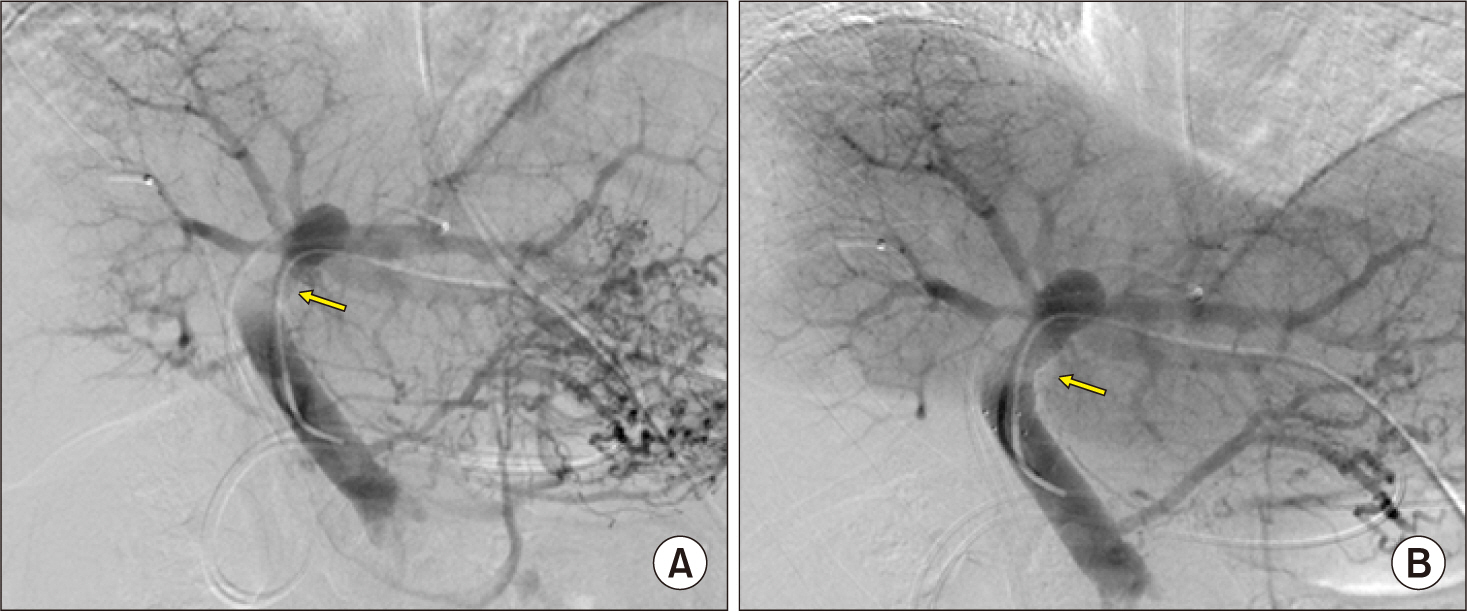
Fig. 2 Preoperative percutaneous portal vein stenting. The transverse portion of the left portal vein was stenotic (A) and expanded after insertion of a self- expandable wall stent of 12 mm× 6 cm in size (B). Arrows indicate the sites of portal vein invasion.
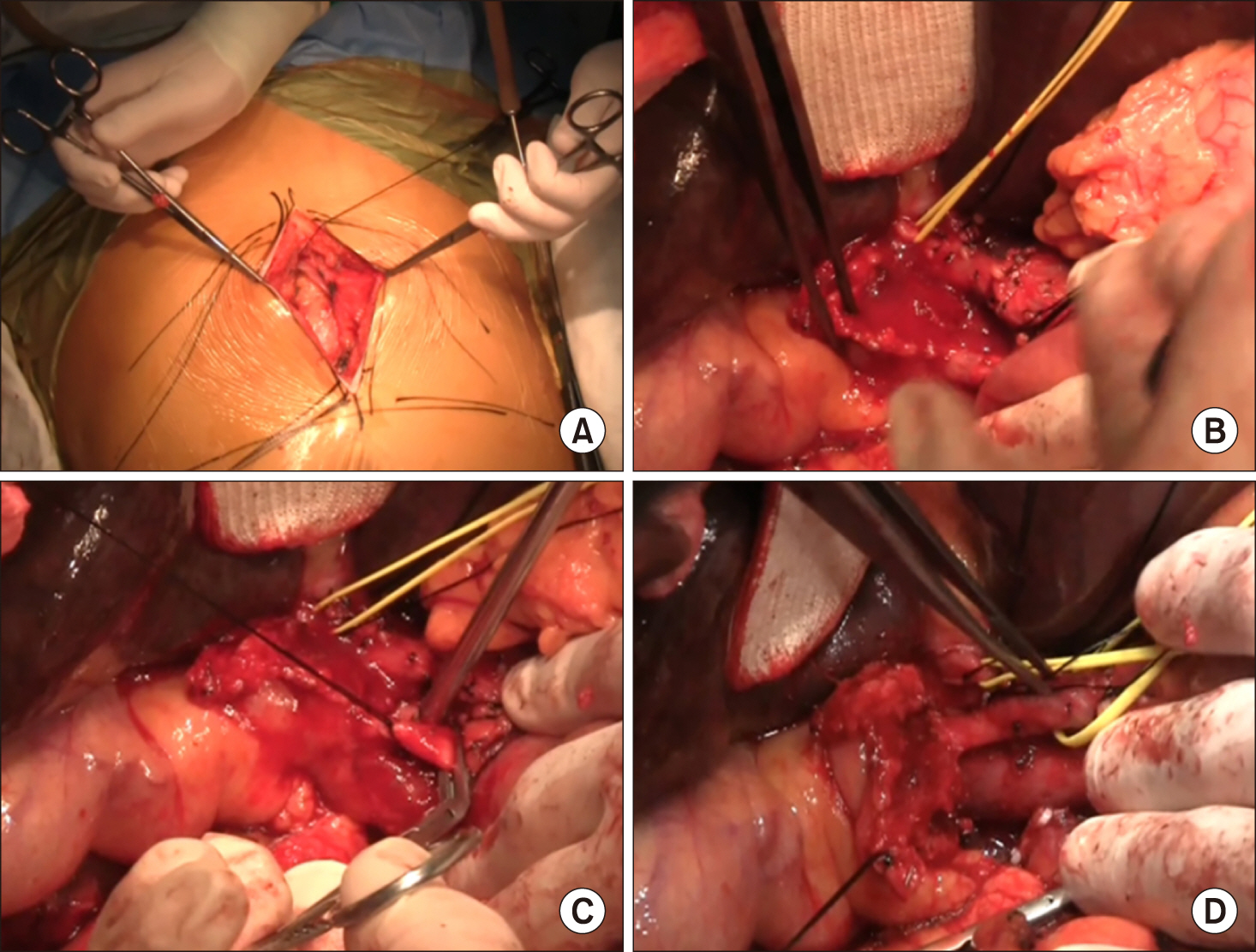
Fig. 3 Intraoperative photographs. (A) Abdominal exploration through mini-laparotomy. (B-D) dissection of the hepatoduodenal ligament.
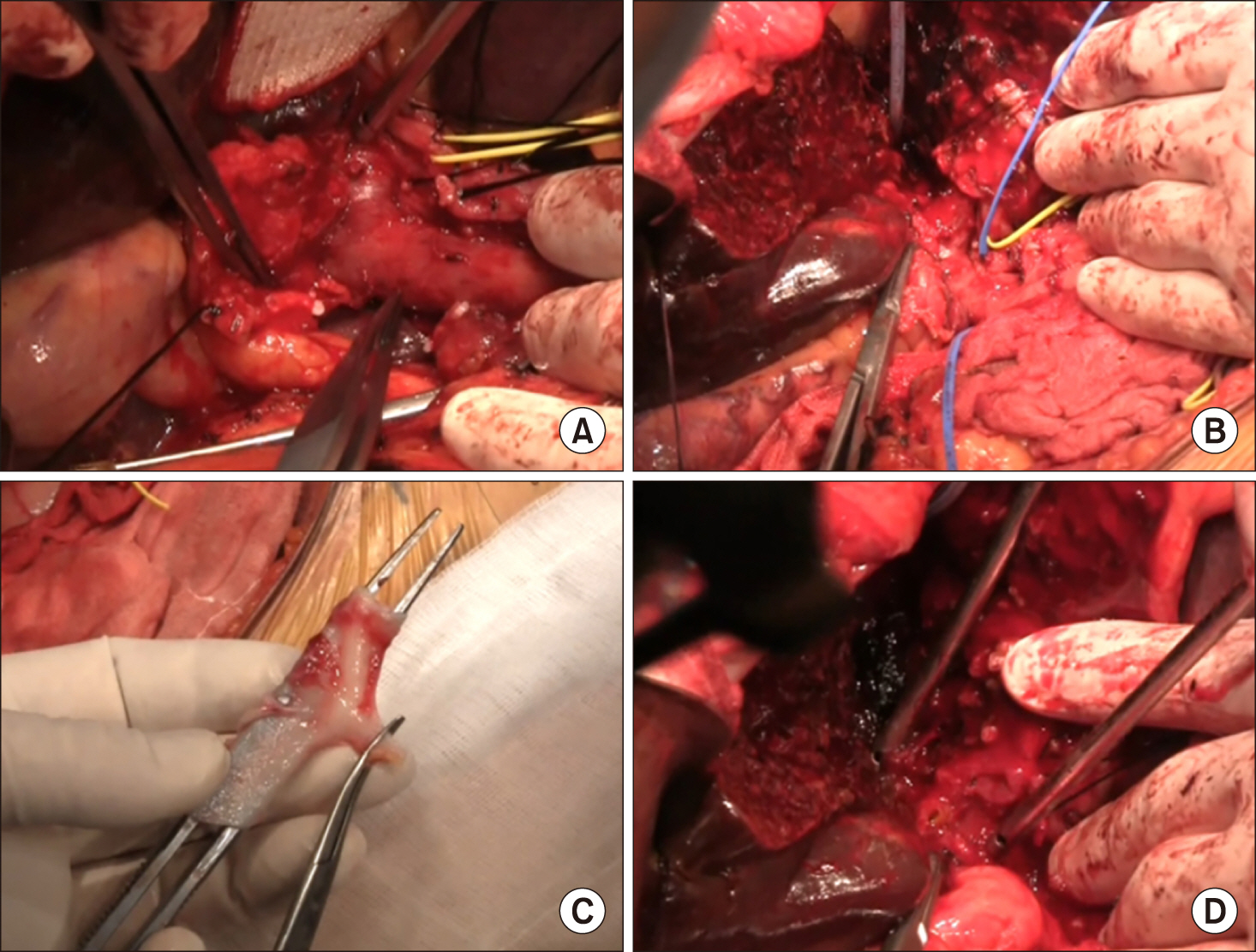
Fig. 4 Intraoperative photographs. (A and B) Exposure of the portal vein system. (C) A segment of cold-stored iliac vein homograft was prepared. (D) The left hepatic duct was transected, thus showing 2 duct openings.
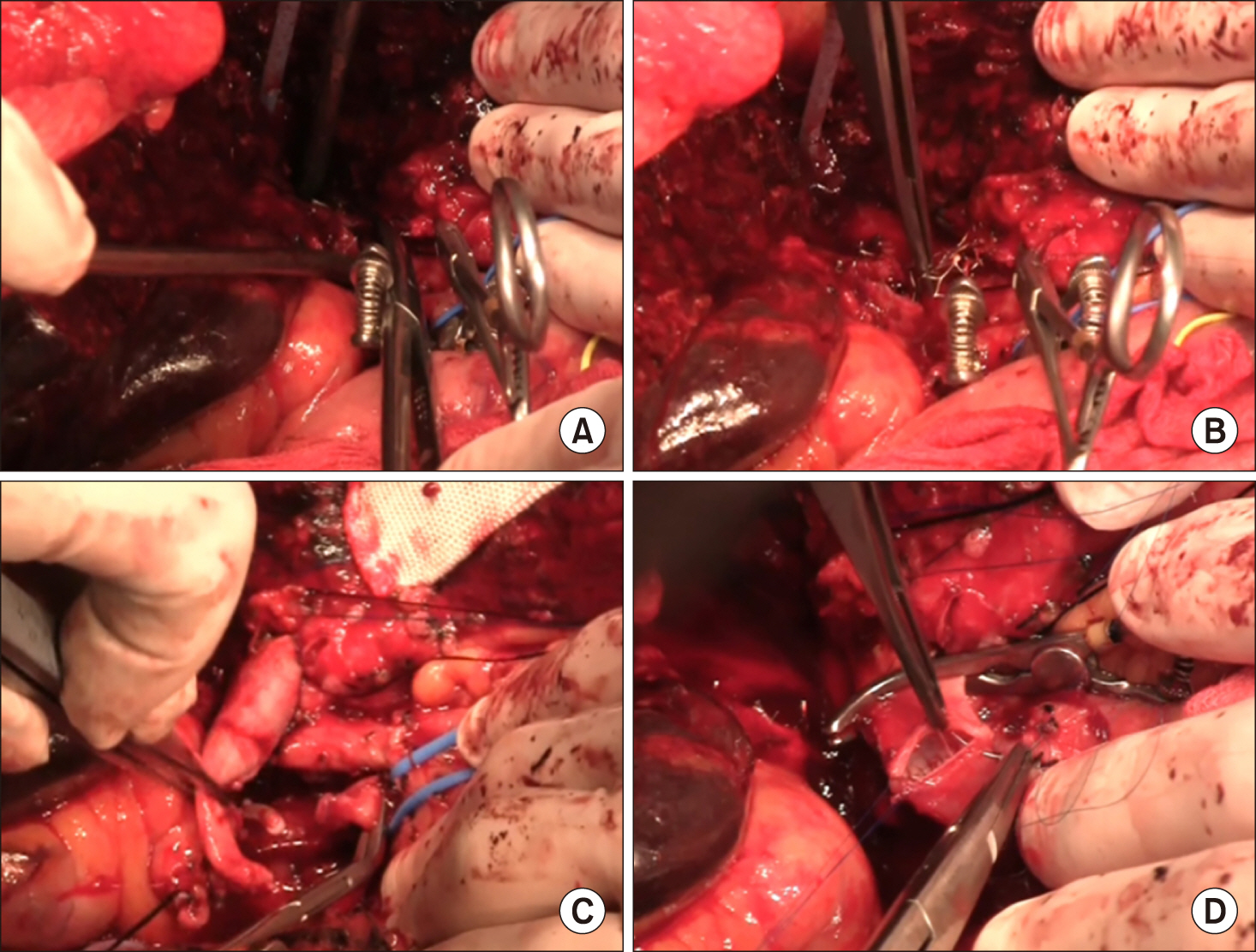
Fig. 5 Intraoperative photographs. (A) The transverse portion of the left portal vein was transected. (B) The fragmented wire network of the disrupted wall stent was removed from the left portal vein stump. (C and D) A 4 cm-long iliac vein homograft was interposed with end-to-end anastomosis.
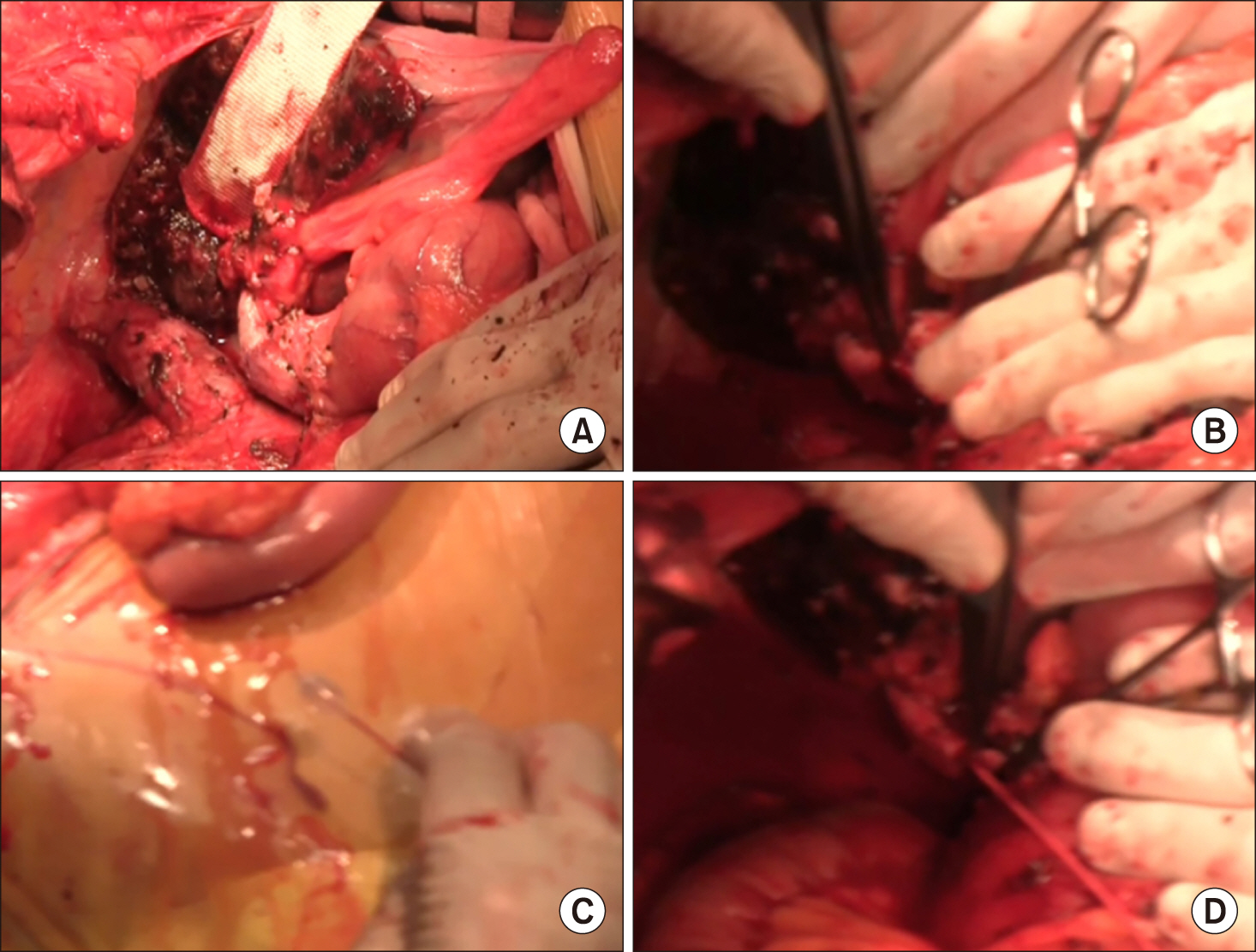
Fig. 6 Intraoperative photographs. (A) The main portal vein was distended with loss of blood flow on palpation. (B-D) A Fogarty catheter was inserted through a small incision at the homograft and thrombus was removed.
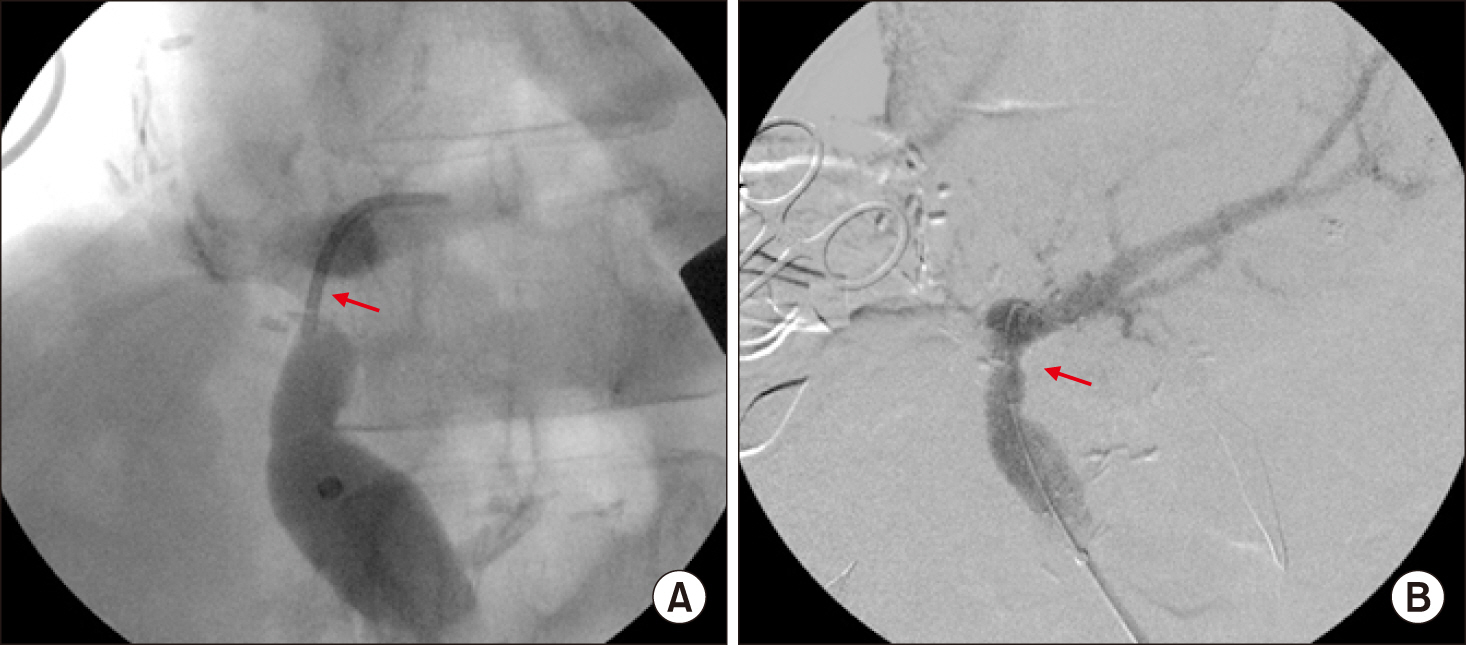
Fig. 7 Intraoperative portal vein stenting. The transverse and umbilical portion of the left portal vein was occluded (A) and expanded after insertion of a self-expandable wall stent of 12 mm×6 cm in size (B). Arrows indicate the sites of portal vein thrombosis.
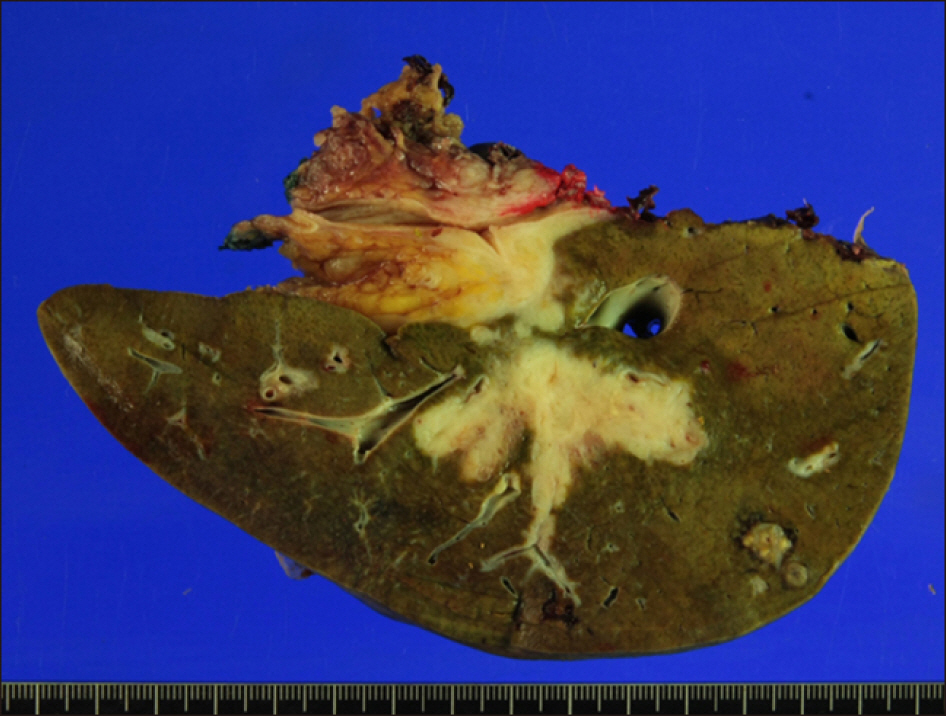
Fig. 8 Gross photograph of the resected specimen.
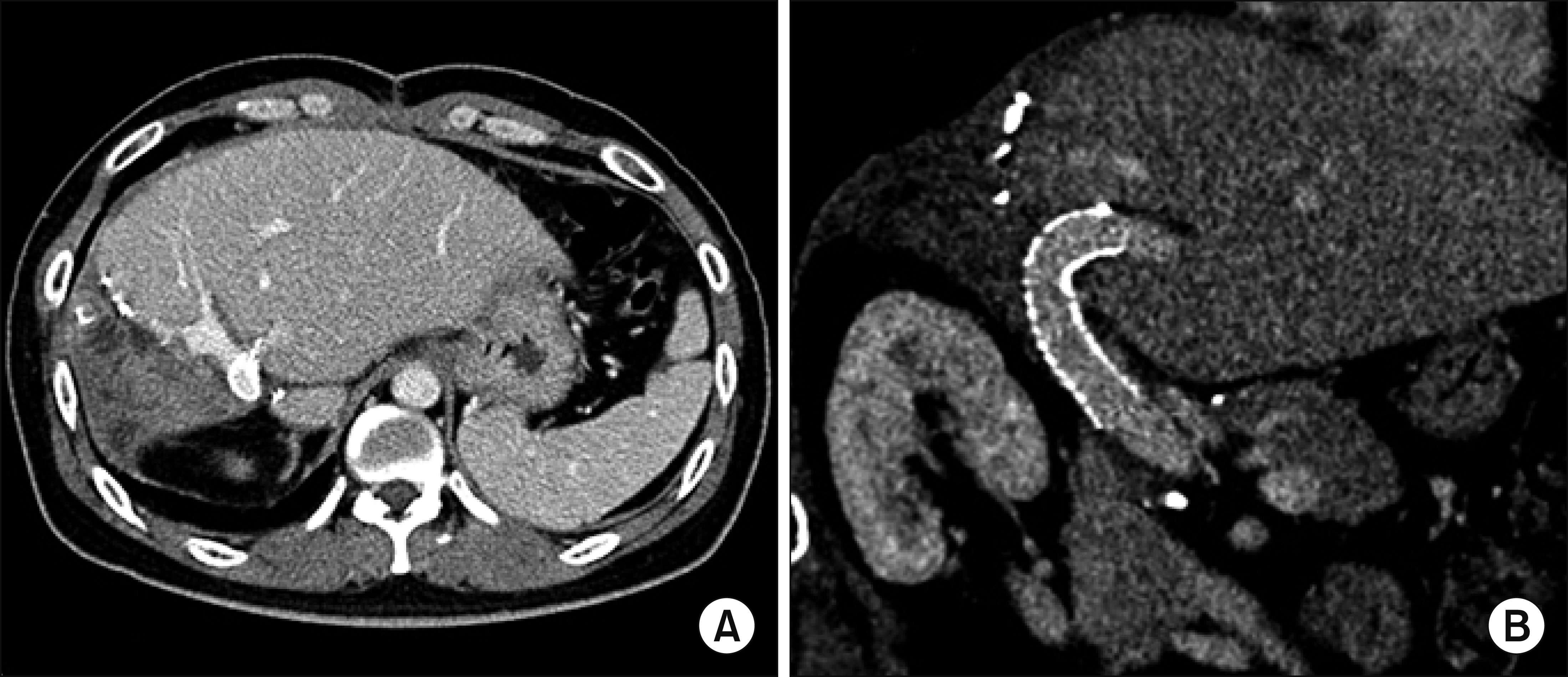
Fig. 9 Postoperative computed tomography findings taken 1 month after surgery. The portal vein conduit was patent on the axial image (A) and reconstructed image (B).

Fig. 10 Postoperative computed tomography follow-up. (A and B) At 4 years after surgery, the portal vein stent was partially occluded with thrombus and the intrahepatic ducts at the hepaticojejunostomy were stenotic with mild ductal dilatation. (C and D) At 7 years, the portal vein stent was completely occluded with cavernous transformation and collaterals were developed.
Cited by 2 articles
-
Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: A report of two cases
Sung-Min Kim, Shin Hwang
Ann Hepatobiliary Pancreat Surg. 2021;25(1):132-138. doi: 10.14701/ahbps.2021.25.1.132.Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
Byeong-Gon Na, Shin Hwang, Dong-Hwan Jung, Sung-Gyu Lee
Ann Hepatobiliary Pancreat Surg. 2021;25(4):509-516. doi: 10.14701/ahbps.2021.25.4.509.
Reference
-
1. Kaneoka Y, Yamaguchi A, Isogai M, Hori A. 1998; Intraportal stent placement combined with right portal vein embolization against advanced gallbladder carcinoma. Surg Today. 28:862–865. DOI: 10.1007/s005950050243. PMID: 9719013.2. Hyodo R, Suzuki K, Ebata T, Komada T, Mori Y, Yokoyama Y, et al. 2015; Assessment of percutaneous transhepatic portal vein embolization with portal vein stenting for perihilar cholangiocarcinoma with severe portal vein stenosis. J Hepatobiliary Pancreat Sci. 22:310–315. DOI: 10.1002/jhbp.200. PMID: 25546292.
Article3. Novellas S, Denys A, Bize P, Brunner P, Motamedi JP, Gugenheim J, et al . 2009; Palliative portal vein stent placement in malignant and symptomatic extrinsic portal vein stenosis or occlusion. Cardiovasc Intervent Radiol. 32:462–470. DOI: 10.1007/s00270-008-9455-9. PMID: 18956224.
Article4. Woodrum DA, Bjarnason H, Andrews JC. 2009; Portal vein venoplasty and stent placement in the nontransplant population. J Vasc Interv Radiol. 20:593–599. DOI: 10.1016/j.jvir.2009.02.010. PMID: 19339200.
Article5. Yamakado K, Nakatsuka A, Tanaka N, Fujii A, Terada N, Takeda K. 2001; Malignant portal venous obstructions treated by stent placement: significant factors affecting patency. J Vasc Interv Radiol. 12:1407–1415. DOI: 10.1016/S1051-0443(07)61699-6. PMID: 11742015.
Article6. Zhou ZQ, Lee JH, Song KB, Hwang JW, Kim SC, Lee YJ, et al. 2014; Clinical usefulness of portal venous stent in hepatobiliary pancreatic cancers. ANZ J Surg. 84:346–352. DOI: 10.1111/ans.12046. PMID: 23421858.
Article7. Ko GY, Sung KB, Yoon HK, Lee S. 2007; Early posttransplantation portal vein stenosis following living donor liver transplantation: percutaneous transhepatic primary stent placement. Liver Transpl. 13:530–536. DOI: 10.1002/lt.21068. PMID: 17394150.
Article8. Kim YJ, Ko GY, Yoon HK, Shin JH, Ko HK, Sung KB. 2007; Intraoperative stent placement in the portal vein during or after liver transplantation. Liver Transpl. 13:1145–1152. DOI: 10.1002/lt.21076. PMID: 17663391.
Article9. Ohm JY, Ko GY, Sung KB, Gwon DI, Ko HK. 2017; Safety and efficacy of transhepatic and transsplenic access for endovascular management of portal vein complications after liver transplantation. Liver Transpl. 23:1133–1142. DOI: 10.1002/lt.24737. PMID: 28152572.
Article10. Hwang S, Sung KB, Park YH, Jung DH, Lee SG. 2007; Portal vein stenting for portal hypertension caused by local recurrence after pancreatoduodenectomy for periampullary cancer. J Gastrointest Surg. 11:333–337. DOI: 10.1007/s11605-006-0058-y. PMID: 17458607.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Right trisectionectomy with en bloc portal vein resection for perihilar cholangiocarcinoma after preoperative left portal vein stenting and sequential right portal and hepatic vein embolization
- Portal Vein Occlusion after Biliary Metal Stent Placement in Hilar Cholangiocarcinoma
- Anatomical variation of the Main and Right Portal Vein on Indirect Portogram: Correlated with CT and Hepatic Angiogram
- Blood flow volume difference (P-SS) between the portal vein and thesum of splenic vein and superior mesenteric vein in portal hypertension
- Noncancerous Right Portal Vein Occlusion: 2 cases
