Type-Specific Viral Load and Physical State of HPV Type 16, 18,and 58 as Diagnostic Biomarkers for High-Grade SquamousIntraepithelial Lesions or Cervical Cancer
- Affiliations
-
- 1Department of Family Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, Seoul, Korea
- 2Department of Tumor Biology, Seoul National University, Seoul, Korea
- 3Department of Obstetrics and Gynecology, Soonchunhyang University College of Medicine, Gumi, Korea
- 4Department of Obstetrics and Gynecology, Dongguk University Ilsan Hospital, Goyang, Korea
- 5Proton Therapy Center, Research Institute and Hospital, National Cancer Center, Goyang, Korea
- 6Center for Uterine Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea
- KMID: 2500325
- DOI: http://doi.org/10.4143/crt.2019.152
Abstract
- Purpose
High rate of false-positive tests is a major obstacle to use human papillomavirus (HPV) detection as a diagnostic tool for high-grade squamous intraepithelial lesions or cervical cancer (HSIL+). We investigated whether type-specific viral load or physical state of HPV 16, 18, and 58 are useful biomarkers for HSIL+.
Materials and Methods
Type-specific viral loads of E6 and E2 genes in cervical cells from 240, 83, and 79 HPV 16–, 18–, and 58–infected women, respectively, were determined using real-time polymerase chain reaction. Viral loads were normalized to cellular DNA (copy/cell). Total and integrated viral loads and physical state were compared between HSIL+ and controls, and diagnostic value was determined using receiver operating characteristic analysis.
Results
Viral loads of HPV 16, 18, and 58 were significantly different in lesions in the same pathologic grade. High type-specific total viral loads were significantly associated with HSIL+ (odds ratio [OR], 14.065, 39.472, and 7.103 for HPV 16, 18, and 58, respectively). High integrated viral load was related to HSIL+ in women with HPV 16 (OR, 8.242), and integrated state was associated with HSIL+ in women with HPV 18 (OR, 9.443). Type-specific total viral load was significantly associated with HSIL+ (area under curve, 0.914, 0.937, and 0.971 for HPV 16, 18, and 58, respectively), indicating an excellent performance in detecting HSIL+.
Conclusion
Type-specific total viral load may be a powerful diagnostic marker for HSIL+ in HPV 16–, 18–, and 58–infected HSIL+ lesions. If demonstrated in all other high-risk HPV types, this method can lead to a paradigm shift in the strategy of equivocal cytologic abnormalities.
Keyword
Figure
-
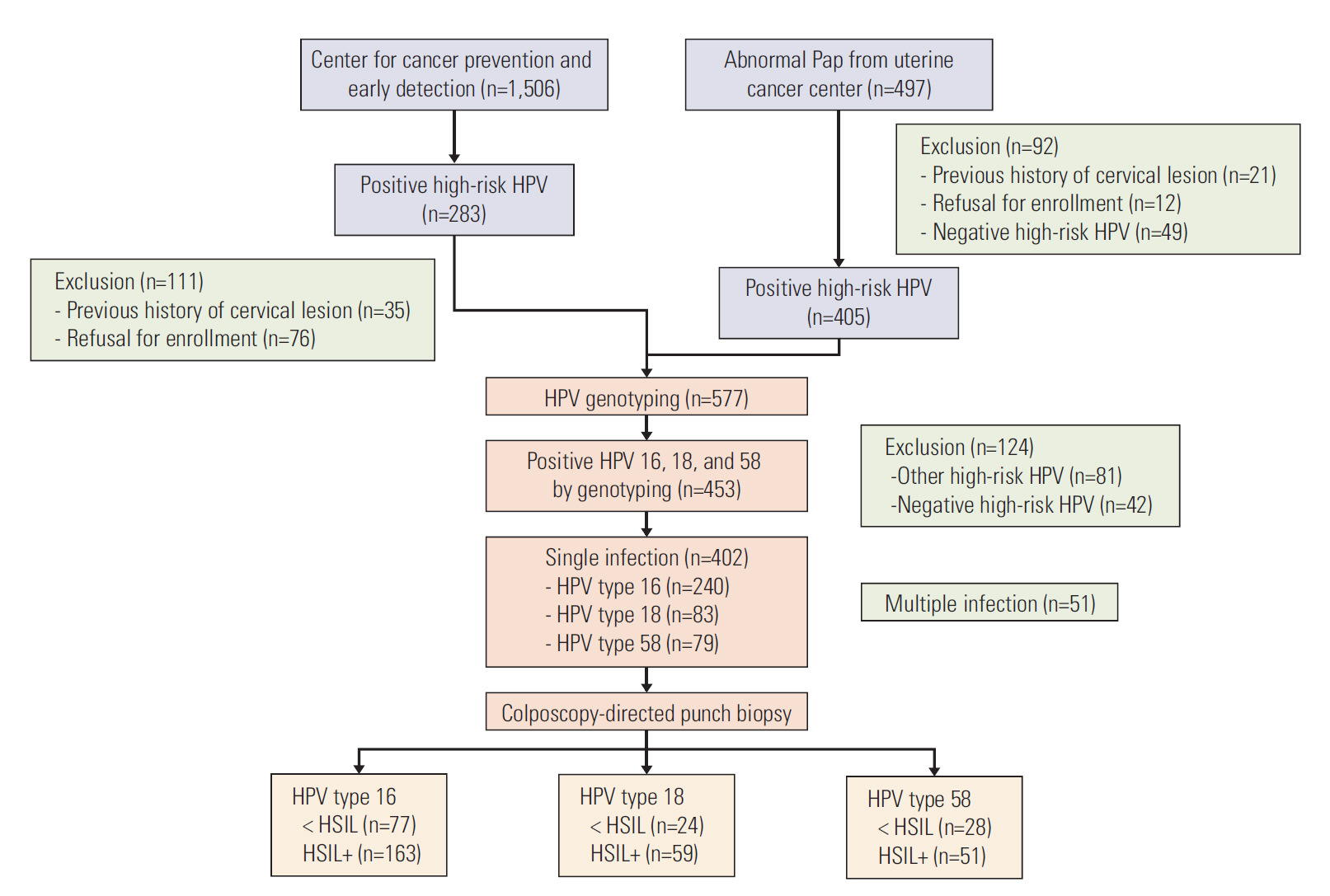
Fig. 1. Flowchart of the study subjects. Pap, Papanicolaou; HPV, human papillomavirus; HSIL, high-grade squamous intraepithelial lesions; HSIL+, high-grade squamous intraepithelial lesions or cervical cancer.
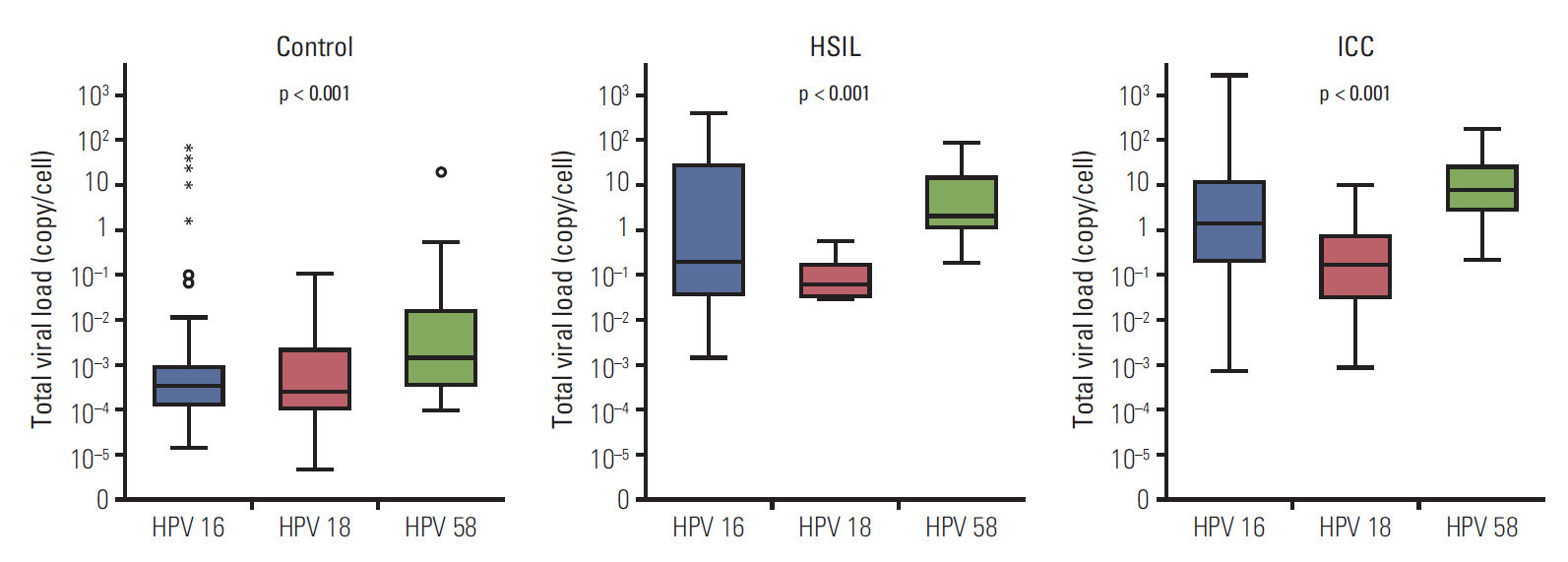
Fig. 2. Type-specific normalized total viral load of human papillomavirus (HPV) 16, 18, and 58 in patients with cervical lesions at the same pathologic grade. Box plots show median and interquartile range. Controls include patients without pathologic abnormalities or with low-grade squamous intraepithelial lesions. p-values were evaluated using Kruskal-Wallis tests. HSIL, high-grade squamous intraepithelial lesions; ICC, invasive cervical cancer.

Fig. 3. Receiver operating characteristic curve analysis of human papillomavirus (HPV) 16, 18, and 58 for the detection of high-grade squamous intraepithelial lesions or cervical cancer by type-specific total and integrated viral load. AUC, area under the curve.
Reference
-
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018; 68:394–424.
Article2. Bosch FX, Manos MM, Munoz N, Sherman M, Jansen AM, Peto J, et al. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International Biological Study on Cervical Cancer (IBSCC) Study Group. J Natl Cancer Inst. 1995; 87:796–802.3. Woodman CB, Collins SI, Young LS. The natural history of cervical HPV infection: unresolved issues. Nat Rev Cancer. 2007; 7:11–22.
Article4. Sankaranarayanan R, Nene BM, Shastri SS, Jayant K, Muwonge R, Budukh AM, et al. HPV screening for cervical cancer in rural India. N Engl J Med. 2009; 360:1385–94.
Article5. Ouh YT, Lee JK. Proposal for cervical cancer screening in the era of HPV vaccination. Obstet Gynecol Sci. 2018; 61:298–308.
Article6. Arbyn M, Ronco G, Anttila A, Meijer CJ, Poljak M, Ogilvie G, et al. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer. Vaccine. 2012; 30 Suppl 5:F88–99.
Article7. Dillner J, Rebolj M, Birembaut P, Petry KU, Szarewski A, Munk C, et al. Long term predictive values of cytology and human papillomavirus testing in cervical cancer screening: joint European cohort study. BMJ. 2008; 337:a1754.
Article8. Darragh TM, Colgan TJ, Thomas Cox J, Heller DS, Henry MR, Luff RD, et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: background and consensus recommendations from the College of American Pathologists and the American Society for Colposcopy and Cervical Pathology. Int J Gynecol Pathol. 2013; 32:76–115.9. Drolet M, Brisson M, Maunsell E, Franco EL, Coutlee F, Ferenczy A, et al. The psychosocial impact of an abnormal cervical smear result. Psychooncology. 2012; 21:1071–81.
Article10. Castle PE, Stoler MH, Wright TC Jr, Sharma A, Wright TL, Behrens CM. Performance of carcinogenic human papillomavirus (HPV) testing and HPV16 or HPV18 genotyping for cervical cancer screening of women aged 25 years and older: a subanalysis of the ATHENA study. Lancet Oncol. 2011; 12:880–90.
Article11. Josefsson AM, Magnusson PK, Ylitalo N, Sorensen P, Qwarforth-Tubbin P, Andersen PK, et al. Viral load of human papilloma virus 16 as a determinant for development of cervical carcinoma in situ: a nested case-control study. Lancet. 2000; 355:2189–93.
Article12. Moberg M, Gustavsson I, Wilander E, Gyllensten U. High viral loads of human papillomavirus predict risk of invasive cervical carcinoma. Br J Cancer. 2005; 92:891–4.
Article13. Carcopino X, Henry M, Mancini J, Giusiano S, Boubli L, Olive D, et al. Significance of HPV 16 and 18 viral load quantitation in women referred for colposcopy. J Med Virol. 2012; 84:306–13.
Article14. Briolat J, Dalstein V, Saunier M, Joseph K, Caudroy S, Pretet JL, et al. HPV prevalence, viral load and physical state of HPV-16 in cervical smears of patients with different grades of CIN. Int J Cancer. 2007; 121:2198–204.
Article15. Pett M, Coleman N. Integration of high-risk human papillomavirus: a key event in cervical carcinogenesis? J Pathol. 2007; 212:356–67.
Article16. Origoni M, Carminati G, Rolla S, Clementi M, Sideri M, Sandri MT, et al. Human papillomavirus viral load expressed as relative light units (RLU) correlates with the presence and grade of preneoplastic lesions of the uterine cervix in atypical squamous cells of undetermined significance (ASCUS) cytology. Eur J Clin Microbiol Infect Dis. 2012; 31:2401–6.
Article17. Jarboe EA, Venkat P, Hirsch MS, Cibas ES, Crum CP, Garner EI. A weakly positive human papillomavirus Hybrid Capture II result correlates with a significantly lower risk of cervical intraepithelial neoplasia 2,3 after atypical squamous cells of undetermined significance cytology. J Low Genit Tract Dis. 2010; 14:174–8.
Article18. Ho CM, Chien TY, Huang SH, Lee BH, Chang SF. Integrated human papillomavirus types 52 and 58 are infrequently found in cervical cancer, and high viral loads predict risk of cervical cancer. Gynecol Oncol. 2006; 102:54–60.
Article19. Kim J, Kim BK, Lee CH, Seo SS, Park SY, Roh JW. Human papillomavirus genotypes and cofactors causing cervical intraepithelial neoplasia and cervical cancer in Korean women. Int J Gynecol Cancer. 2012; 22:1570–6.
Article20. Burk RD, Ho GY, Beardsley L, Lempa M, Peters M, Bierman R. Sexual behavior and partner characteristics are the predominant risk factors for genital human papillomavirus infection in young women. J Infect Dis. 1996; 174:679–89.
Article21. Kim CJ, Lee YS, Kwack HS, Yoon WS, Park TC, Park JS. Specific human papillomavirus types and other factors on the risk of cervical intraepithelial neoplasia: a case-control study in Korea. Int J Gynecol Cancer. 2010; 20:1067–73.
Article22. Peitsaro P, Johansson B, Syrjanen S. Integrated human papillomavirus type 16 is frequently found in cervical cancer precursors as demonstrated by a novel quantitative real-time PCR technique. J Clin Microbiol. 2002; 40:886–91.
Article23. Saunier M, Monnier-Benoit S, Mauny F, Dalstein V, Briolat J, Riethmuller D, et al. Analysis of human papillomavirus type 16 (HPV16) DNA load and physical state for identification of HPV16-infected women with high-grade lesions or cervical carcinoma. J Clin Microbiol. 2008; 46:3678–85.
Article24. Shukla S, Mahata S, Shishodia G, Pande S, Verma G, Hedau S, et al. Physical state & copy number of high risk human papillomavirus type 16 DNA in progression of cervical cancer. Indian J Med Res. 2014; 139:531–43.25. Hesselink AT, Berkhof J, Heideman DA, Bulkmans NW, van Tellingen JE, Meijer CJ, et al. High-risk human papillomavirus DNA load in a population-based cervical screening cohort in relation to the detection of high-grade cervical intraepithelial neoplasia and cervical cancer. Int J Cancer. 2009; 124:381–6.
Article26. Sherman ME, Wang SS, Wheeler CM, Rich L, Gravitt PE, Tarone R, et al. Determinants of human papillomavirus load among women with histological cervical intraepithelial neoplasia 3: dominant impact of surrounding low-grade lesions. Cancer Epidemiol Biomarkers Prev. 2003; 12:1038–44.27. Badaracco G, Venuti A, Sedati A, Marcante ML. HPV16 and HPV18 in genital tumors: significantly different levels of viral integration and correlation to tumor invasiveness. J Med Virol. 2002; 67:574–82.
Article28. Marongiu L, Godi A, Parry JV, Beddows S. Human papillomavirus 16, 18, 31 and 45 viral load, integration and methylation status stratified by cervical disease stage. BMC Cancer. 2014; 14:384.
Article29. Wu Z, Qin Y, Yu L, Lin C, Wang H, Cui J, et al. Association between human papillomavirus (HPV) 16, HPV18, and other HR-HPV viral load and the histological classification of cervical lesions: results from a large-scale cross-sectional study. J Med Virol. 2017; 89:535–41.
Article30. Takehara K, Toda T, Nishimura T, Sakane J, Kawakami Y, Mizunoe T, et al. Human papillomavirus types 52 and 58 are prevalent in uterine cervical squamous lesions from Japanese women. Patholog Res Int. 2011; 2011:246936.
Article31. Pett MR, Herdman MT, Palmer RD, Yeo GS, Shivji MK, Stanley MA, et al. Selection of cervical keratinocytes containing integrated HPV16 associates with episome loss and an endogenous antiviral response. Proc Natl Acad Sci U S A. 2006; 103:3822–7.
Article32. Vinokurova S, Wentzensen N, Kraus I, Klaes R, Driesch C, Melsheimer P, et al. Type-dependent integration frequency of human papillomavirus genomes in cervical lesions. Cancer Res. 2008; 68:307–13.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Physical Status and Viral load in Women with Positive Human Papillomavirus (HPV) Infection in Uterine Cervix
- Prognostic Significance of Human Papillomavirus Types 16 and 18 in Invasive Cervical Cancer
- Detection of Human Papillomavirus Type 16 and 18 in Cervical Specimens by Nested Polymerase Chain Reaction
- Prevalence and Genotyping of HPV in Different Grades of Cervical Intraepithelial Neoplasia and Cervical Cancer
- Detection of Human Papillomavirus DNA 16/18 in Cervical Adenocarcinomas by Polymerase Chain Reaction
