Ann Clin Neurophysiol.
2020 Apr;22(1):19-23. 10.14253/acn.2020.22.1.19.
Immobilization-induced rhabdomyolysispatients with peripheral neuropathy:clinical, laboratory and imagingfindings
- Affiliations
-
- 1Department of Neurology, Catholic University of Daegu School of Medicine, Daegu, Korea
- 2Department of Nephrology, Catholic University of Daegu School of Medicine, Daegu, Korea
- 3Medical Statistics & Informatics, Catholic University of Daegu School of Medicine, Daegu, Korea
- KMID: 2500299
- DOI: http://doi.org/10.14253/acn.2020.22.1.19
Abstract
- Background
Peripheral nerve injury rarely occurs in patients with rhabdomyolysis. Based on our experience and previous reports, we consider prolonged immobilization a risk factor for the development of peripheral neuropathy in rhabdomyolysis patients.
Methods
This study analyzed 28 patients with rhabdomyolysis due to prolonged immobilization. We analyzed their demographic and laboratory data, clinical and imaging findings, and outcomes, and compared these factors between patients with and without neuropathy.
Results
Seven of the 28 patients had peripheral neuropathy, including sciatic neuropathy or lumbosacral plexopathy. Compared to those without neuropathy, the patients with neuropathy were younger (p = 0.02), had higher peak creatine kinase (CK) levels (p = 0.02), had higher muscle uptake in bone scans (p = 0.03), and more frequently exhibited abnormal muscle findings in computed tomography (CT) (p = 0.004).
Conclusions
Patients with prolonged immobilization-induced rhabdomyolysis and neuropathy had higher CK levels, increased uptake on bone scans, and more-frequent abnormal muscles on CT than those without neuropathy. These findings indicate that peripheral neuropathy is more likely to develop in patients with severe muscle injury.
Figure
-
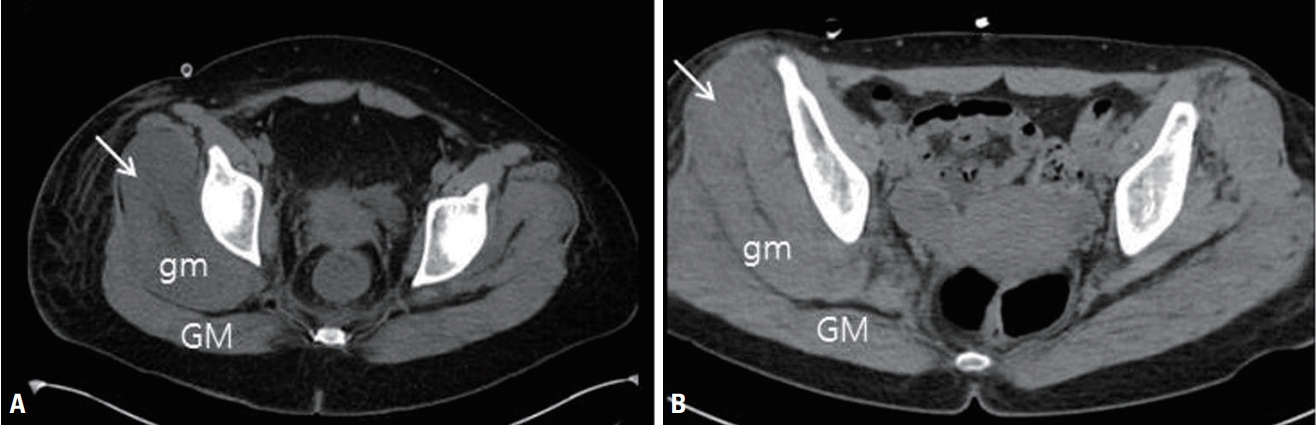
Fig. 1. Examples of abnormal computed tomography findings. (A) Axial image showing a low muscle signal intensity and swelling of the right gluteus medius muscle (arrow). (B) Axial image showing diffuse swelling of the right gluteous medius muscle (arrow). GM, gluteus maximus; gm, gluteus medius.
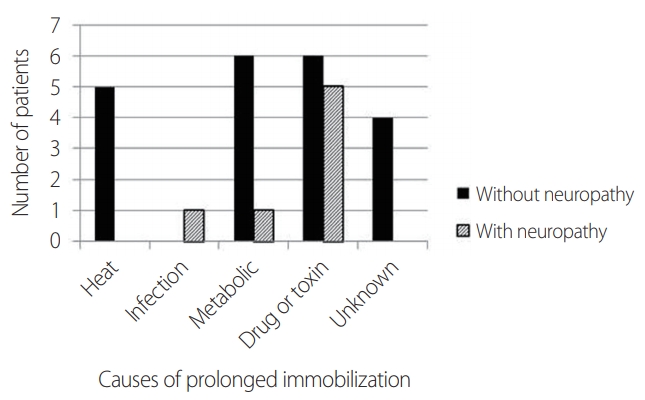
Fig. 2. Causes of prolonged immobilization in the two study groups.
Reference
-
1. Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009; 361:62–72.
Article2. Seok JI, Lee IH, Ahn KS, Kang GW, Kim JH. Peripheral neuropathies in patients with rhabdomyolysis: clinical characteristics and electrodiagnostic findings in the acute/subacute stage. J Korean Neurol Assoc. 2019; 37:26–29.
Article3. Maddison P. Acute rhabdomyolysis and brachial plexopathy following alcohol ingestion. Muscle Nerve. 2002; 25:283–285.4. Nicolle M, Doherty T, Algahtani H. Bilateral femoral neuropathy complicating rhabdomyolysis and acute renal failure. J Clin Neuromuscul Dis. 2005; 6:153–156.
Article5. Ji JW. Acute compartment syndrome which causes rhabdomyolysis by carbon monoxide poisoning and sciatic nerve injury associated with it: a case report. Hip Pelvis. 2017; 29:204–209.
Article6. Kim IS, Lee WH, Lim JY. Multiple peripheral neuropathies adjacent to necrotizing myositis related to rhabdomyolysis. AGMR. 2017; 21:31–34.
Article7. McMahon GM, Zeng X, Waikar SS. A risk prediction score for kidney failure or mortality in rhabdomyolysis. JAMA Intern Med. 2013; 173:1821–1828.
Article8. Hamel Y, Mamoune A, Mauvais FX, Habarou F, Lallement L, Romero NB, et al. Acute rhabdomyolysis and inflammation. J Inherit Metab Dis. 2015; 38:621–628.
Article9. Feng Q, Wilke RA, Baye TM. Individualized risk for statin-induced myopathy: current knowledge, emerging challenges and potential solutions. Pharmacogenomics. 2012; 13:579–594.
Article10. Knapik JJ, O’Connor FG. Exertional rhabdomyolysis: epidemiology, diagnosis, treatment, and prevention. J Spec Oper Med. 2016; 16:65–71.11. Chang HR, Kao CH, Lian JD, Shu KH, Cheng CH, Wu MJ, et al. Evaluation of the severity of traumatic rhabdomyolysis using technetium-99m pyrophosphate scintigraphy. Am J Nephrol. 2001; 21:208–214.
Article12. Keltz E, Khan FY, Mann G. Rhabdomyolysis. The role of diagnostic and prognostic factors. Muscles Ligaments Tendons J. 2014; 3:303–312.
Article13. Lamminen AE, Hekali PE, Tiula E, Suramo I, Korhola OA. Acute rhabdomyolysis: evaluation with magnetic resonance imaging compared with computed tomography and ultrasonography. Br J Radiol. 1989; 62:326–330.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Peripheral Neuropathies in Patients with Rhabdomyolysis: Clinical Characteristics and Electrodiagnostic Findings in the Acute/Subacute Stage
- Neurofibromatous Polyneuropathy
- Clinical Scales for Peripheral Neuropathy - Revision 2021
- Paraproteinemic neuropathy
- Treatment of peripheral neuropathy: a multidisciplinary approach is necessary
