Korean J Leg Med.
2020 Feb;44(1):37-40. 10.7580/kjlm.2020.44.1.37.
Lung Pathology in Septic Shock with Leukopenia
- Affiliations
-
- 1Department of Forensic Medicine, Pusan National University School of Medicine, Yangsan, Korea. gyhuh@pusan.ac.kr
- 2Department of Pathology, Pusan National University Hospital, Busan, Korea.
- KMID: 2471743
- DOI: http://doi.org/10.7580/kjlm.2020.44.1.37
Abstract
- Sepsis-related deaths are occasionally encountered in forensic practice. However, forensic pathologists are reluctant to use the terminology "sepsis" or "septic shock" as a cause of death because of the lack of definite morphological evidence. When sepsis is considered a cause of death, pathologic assessment is essential to identify the foci of infection or consequences of sepsis, such as diffuse alveolar damage (DAD). Pneumonia is known to be a common source of sepsis and can develop into DAD with progression of sepsis. The histology of DAD varies according to the immunologic status. An autopsy of a 55-year-old man who died of septic shock with leukopenia revealed only abundant gram-negative bacilli in the alveoli without typical DAD pathology.
Keyword
MeSH Terms
Figure
-
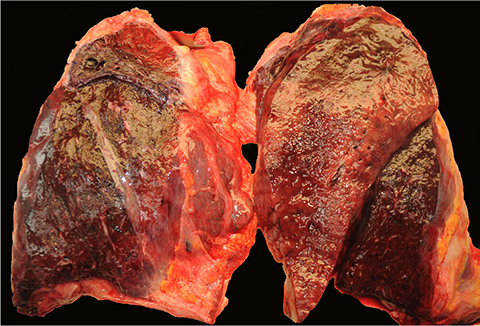
Fig. 1 Section of the enlarged lungs shows consolidations on the upper lobe of the left lung and middle lobe of the right lung and reveals oily mucoid material exuded on the surface.

Fig. 2 (A) Dilated alveoli are filled with proteinaceous material and foamy macrophages (H&E, × 100). (B) Medium-power view shows abundant gram-negative bacilli in the alveoli, without neutrophilic infiltrate and hyaline membrane formation (H&E, × 200).
Reference
-
1. Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016; 315:801–810.2. Lucas S. The autopsy pathology of sepsis-related death. Curr Diagn Pathol. 2007; 13:375–388.
Article3. Morris JA, Harrison LM, Partridge SM. Postmortem bacteriology: a re-evaluation. J Clin Pathol. 2006; 59:1–9.
Article4. Laufe MD, Simon RH, Flint A, et al. Adult respiratory distress syndrome in neutropenic patients. Am J Med. 1986; 80:1022–1026.
Article5. Altaf E, Mitchel EK, Berry C, et al. Death due to pulmonary alveolar proteinosis. Am J Forensic Med Pathol. 2017; 38:11–13.
Article6. Warny M, Helby J, Nordestgaard BG, et al. Lymphopenia and risk of infection and infection-related death in 98,344 individuals from a prospective Danish population-based study. PLoS Med. 2018; 15:e1002685.
Article7. Schiel X, Hebart H, Kern WV, et al. Sepsis in neutropenia: guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Oncology (DGHO). Ann Hematol. 2003; 82 Suppl 2:S158–S166.8. Gyawali B, Ramakrishna K, Dhamoon AS. Sepsis: the evolution in definition, pathophysiology, and management. SAGE Open Med. 2019; 7:2050312119835043.
Article9. Drewry AM, Samra N, Skrupky LP, et al. Persistent lymphopenia after diagnosis of sepsis predicts mortality. Shock. 2014; 42:383–391.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Prognostic Factors of Pneumonia with Septic Shock in Patients Presenting to the Emergency Department
- Septic Shock due to Vibrio alginolyticus in a Cirrhotic Patient: The First Case in Korea
- Treatment Guidelines of Sepsis and Septic Shock
- Prognostic Factors in Septic Shock Patients on Arrival at Emergency Department
- Septic Shock