Is Follow-up of Adrenal Incidentalomas Always Mandatory?
- Affiliations
-
- 1Division of Internal Medicine, Department of Clinical and Biological Sciences, San Luigi Gonzaga Hospital, University of Turin, Orbassano, Italy. sorayapuglisi@yahoo.com
- KMID: 2471717
- DOI: http://doi.org/10.3803/EnM.2020.35.1.26
Abstract
- Adrenal masses are mainly detected unexpectedly by an imaging study performed for reasons unrelated to any suspect of adrenal diseases. Such masses are commonly defined as "adrenal incidentalomas" and represent a public health challenge because they are increasingly recognized in current medical practice. Management of adrenal incidentalomas is currently matter of debate. Although there is consensus on the need of a multidisciplinary expert team evaluation and surgical approach in patients with significant hormonal excess and/or radiological findings suspicious of malignancy demonstrated at the diagnosis or during follow-up, the inconsistency between official guidelines and the consequent diffuse uncertainty on management of small adrenal incidentalomas still represents a considerable problem in terms of clinical choices in real practice. The aim of the present work is to review the proposed strategies on how to manage patients with adrenal incidentalomas that are not candidates to immediate surgery. The recent European Society of Endocrinology/European Network for the Study of Adrenal Tumors guidelines have supported the view to avoid surveillance in patients with clear benign adrenal lesions <4 cm and/or without any hormonal secretion; however, newer prospective studies are needed to confirm safety of this strategy, in particular in younger patients.
Keyword
MeSH Terms
Figure
-
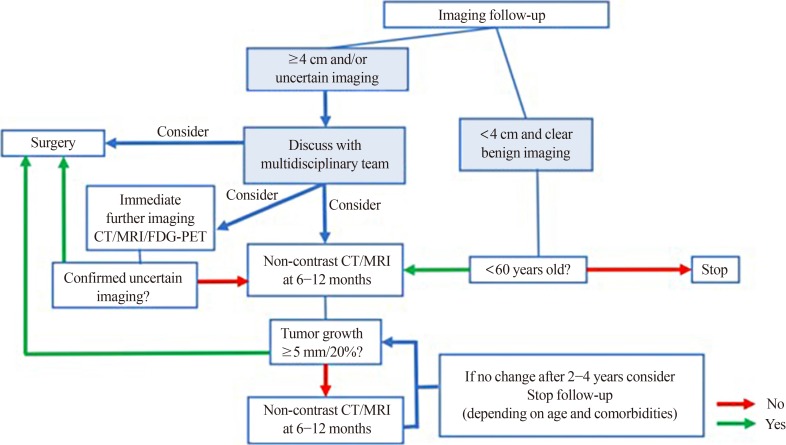
Fig. 1 Flowchart on the radiological follow-up of adrenal incidentalomas. After first radiological evaluation of adrenal masses <4 cm with clear radiological benign features, we suggest no further imaging in patients ages >60 years. For patients aged <60 years, we suggest one single imaging control after 6 to 12 months. After first radiological evaluation of adrenal masses ≥4 cm and/or uncertain radiological features, three possibilities can be considered and should be discussed by a multidisciplinary team: immediate surgery, immediate further imaging with another technique or delayed radiological re-evaluation after 6 to 12 months. If the uncertain nature of the adrenal lesion is confirmed, or if the imaging follow-up shows a growth >5 mm or >20%, surgery should be considered. If no changes of the lesion are observed at 6 to 12 months, radiological follow-up can be continued up to 2 to 4 years, depending on age and comorbidities of the patients, and then stopped if stability of the lesion is confirmed. CT, computed tomography; MRI, magnetic resonance imaging; FDG-PET, fluorodeoxyglucose positron emission tomography.
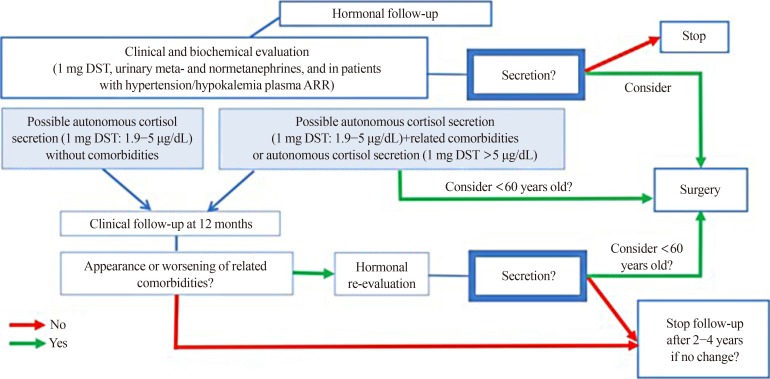
Fig. 2 Flowchart on the biochemical follow-up of adrenal incidentalomas. At first evaluation, patients with adrenal incidentaloma should undergo a clinical and biochemical evaluation for hormonal secretion, consisting of 1 mg-dexamethasone suppression test (DST), plasma-free or urinary fractionated metanephrines and aldosterone/renin ratio (ARR) in patients with hypertension or unexplained hypokalemia. If hormonal secretion at diagnosis is excluded, biochemical follow-up is not indicated. In case of overt Cushing's syndrome, pheochromocytoma or primary hyperaldosteronism, surgery should be considered. Surgery can also be considered in patients with autonomous cortisol secretion or possible autonomous cortisol secretion with related comorbidities; if surgery is not performed, patients with possible autonomous cortisol secretion without comorbidities should undergo a clinical follow-up after 12 months with a subsequent biochemical re-evaluation in case of clinical worsening. If the biochemical re-evaluation shows hormonal secretion, surgery should be considered, particularly in patients aged <60 years. In case of clinical and biochemical stability, biochemical follow-up can be stopped after 2 to 4 years.
Reference
-
1. Terzolo M, Stigliano A, Chiodini I, Loli P, Furlani L, Arnaldi G, et al. AME position statement on adrenal incidentaloma. Eur J Endocrinol. 2011; 164:851–870. PMID: 21471169.
Article2. Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2016; 175:G1–G34. PMID: 27390021.
Article3. Glazer HS, Weyman PJ, Sagel SS, Levitt RG, McClennan BL. Nonfunctioning adrenal masses: incidental discovery on computed tomography. AJR Am J Roentgenol. 1982; 139:81–85. PMID: 6979870.
Article4. Prinz RA, Brooks MH, Churchill R, Graner JL, Lawrence AM, Paloyan E, et al. Incidental asymptomatic adrenal masses detected by computed tomographic scanning: is operation required? JAMA. 1982; 248:701–704. PMID: 7097921.5. Abecassis M, McLoughlin MJ, Langer B, Kudlow JE. Serendipitous adrenal masses: prevalence, significance, and management. Am J Surg. 1985; 149:783–788. PMID: 4014556.6. Belldegrun A, Hussain S, Seltzer SE, Loughlin KR, Gittes RF, Richie JP. Incidentally discovered mass of the adrenal gland. Surg Gynecol Obstet. 1986; 163:203–208. PMID: 3750174.
Article7. Herrera MF, Grant CS, van Heerden JA, Sheedy PF, Ilstrup DM. Incidentally discovered adrenal tumors: an institutional perspective. Surgery. 1991; 110:1014–1021. PMID: 1745970.8. Caplan RH, Strutt PJ, Wickus GG. Subclinical hormone secretion by incidentally discovered adrenal masses. Arch Surg. 1994; 129:291–296. PMID: 8129606.
Article9. Bovio S, Cataldi A, Reimondo G, Sperone P, Novello S, Berruti A, et al. Prevalence of adrenal incidentaloma in a contemporary computerized tomography series. J Endocrinol Invest. 2006; 29:298–302. PMID: 16699294.
Article10. Hammarstedt L, Muth A, Wangberg B, Bjorneld L, Sigurjonsdottir HA, Gotherstrom G, et al. Adrenal lesion frequency: a prospective, cross-sectional CT study in a defined region, including systematic re-evaluation. Acta Radiol. 2010; 51:1149–1156. PMID: 20969508.
Article11. Grossman A, Koren R, Tirosh A, Michowiz R, Shohat Z, Rahamimov R, et al. Prevalence and clinical characteristics of adrenal incidentalomas in potential kidney donors. Endocr Res. 2016; 41:98–102. PMID: 26541634.
Article12. Reimondo G, Castellano E, Grosso M, Priotto R, Puglisi S, Pia A, et al. Adrenal incidentalomas are tied to increased risk of diabetes: findings from a prospective study. J Clin Endocrinol Metab. 2020; 1. 04. [Epub]. DOI: 10.1210/clinem/dgz284.
Article13. Reincke M. Subclinical Cushing's syndrome. Endocrinol Metab Clin North Am. 2000; 29:43–56. PMID: 10732263.
Article14. Terzolo M, Bovio S, Reimondo G, Pia A, Osella G, Borretta G, et al. Subclinical Cushing's syndrome in adrenal incidentalomas. Endocrinol Metab Clin North Am. 2005; 34:423–439. PMID: 15850851.
Article15. Terzolo M, Bovio S, Pia A, Osella G, Borretta G, Angeli A, et al. Subclinical Cushing's syndrome. Arq Bras Endocrinol Metabol. 2007; 51:1272–1279. PMID: 18209865.
Article16. Barzon L, Scaroni C, Sonino N, Fallo F, Paoletta A, Boscaro M. Risk factors and long-term follow-up of adrenal incidentalomas. J Clin Endocrinol Metab. 1999; 84:520–526. PMID: 10022410.
Article17. Morelli V, Reimondo G, Giordano R, Della Casa S, Policola C, Palmieri S, et al. Long-term follow-up in adrenal incidentalomas: an Italian multicenter study. J Clin Endocrinol Metab. 2014; 99:827–834. PMID: 24423350.
Article18. Zeiger MA, Thompson GB, Duh QY, Hamrahian AH, Angelos P, Elaraj D, et al. The American Association of Clinical Endocrinologists and American Association of Endocrine Surgeons medical guidelines for the management of adrenal incidentalomas. Endocr Pract. 2009; 15 Suppl 1:1–20.19. NIH state-of-the-science statement on management of the clinically inapparent adrenal mass (“incidentaloma”). NIH Consens State Sci Statements. 2002; 19:1–25.20. Tabarin A, Bardet S, Bertherat J, Dupas B, Chabre O, Hamoir E, et al. Exploration and management of adrenal incidentalomas. French Society of Endocrinology Consensus. Ann Endocrinol (Paris). 2008; 69:487–500. PMID: 19022420.21. Kapoor A, Morris T, Rebello R. Guidelines for the management of the incidentally discovered adrenal mass. Can Urol Assoc J. 2011; 5:241–247. PMID: 21801680.
Article22. Bednarczuk T, Bolanowski M, Sworczak K, Gornicka B, Cieszanowski A, Otto M, et al. Adrenal incidentaloma in adults: management recommendations by the Polish Society of Endocrinology. Endokrynol Pol. 2016; 67:234–258. PMID: 27082051.23. Lee JM, Kim MK, Ko SH, Koh JM, Kim BY, Kim SW, et al. Clinical guidelines for the management of adrenal incidentaloma. Endocrinol Metab (Seoul). 2017; 32:200–218. PMID: 28685511.
Article24. Hong AR, Kim JH, Park KS, Kim KY, Lee JH, Kong SH, et al. Optimal follow-up strategies for adrenal incidentalomas: reappraisal of the 2016 ESE-ENSAT guidelines in real clinical practice. Eur J Endocrinol. 2017; 177:475–483. PMID: 28870984.
Article25. Elhassan YS, Alahdab F, Prete A, Delivanis DA, Khanna A, Prokop L, et al. Natural history of adrenal incidentalomas with and without mild autonomous cortisol excess: a systematic review and meta-analysis. Ann Intern Med. 2019; 171:107–116. PMID: 31234202.26. Terzolo M, Reimondo G. Insights on the natural history of adrenal incidentalomas. Ann Intern Med. 2019; 171:135–136. PMID: 31234201.
Article27. Tasaki M, Kasahara T, Takizawa I, Saito K, Nishiyama T, Tomita Y. Limited significance of repeated long-term radiological and hormonal examination in nonfunctioning adrenal incidentalomas. Int Braz J Urol. 2019; 45:503–513. PMID: 30785700.
Article28. Debono M, Bradburn M, Bull M, Harrison B, Ross RJ, Newell-Price J. Cortisol as a marker for increased mortality in patients with incidental adrenocortical adenomas. J Clin Endocrinol Metab. 2014; 99:4462–4470. PMID: 25238207.
Article29. Di Dalmazi G, Vicennati V, Garelli S, Casadio E, Rinaldi E, Giampalma E, et al. Cardiovascular events and mortality in patients with adrenal incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing's syndrome: a 15-year retrospective study. Lancet Diabetes Endocrinol. 2014; 2:396–405. PMID: 24795253.
Article30. Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence and natural history of adrenal incidentalomas. Eur J Endocrinol. 2003; 149:273–285. PMID: 14514341.
Article31. Bernini GP, Moretti A, Oriandini C, Bardini M, Taurino C, Salvetti A. Long-term morphological and hormonal follow-up in a single unit on 115 patients with adrenal incidentalomas. Br J Cancer. 2005; 92:1104–1109. PMID: 15770213.
Article32. Fagour C, Bardet S, Rohmer V, Arimone Y, Lecomte P, Valli N, et al. Usefulness of adrenal scintigraphy in the follow-up of adrenocortical incidentalomas: a prospective multicenter study. Eur J Endocrinol. 2009; 160:257–264. PMID: 18974229.
Article33. Libe R, Dall'Asta C, Barbetta L, Baccarelli A, Beck-Peccoz P, Ambrosi B. Long-term follow-up study of patients with adrenal incidentalomas. Eur J Endocrinol. 2002; 147:489–494. PMID: 12370111.
Article34. Nieman LK. Update on subclinical Cushing's syndrome. Curr Opin Endocrinol Diabetes Obes. 2015; 22:180–184. PMID: 25887388.
Article35. Dekkers OM, Horvath-Puho E, Jorgensen JO, Cannegieter SC, Ehrenstein V, Vandenbroucke JP, et al. Multisystem morbidity and mortality in Cushing's syndrome: a cohort study. J Clin Endocrinol Metab. 2013; 98:2277–2284. PMID: 23533241.
Article36. Lacroix A, Feelders RA, Stratakis CA, Nieman LK. Cushing's syndrome. Lancet. 2015; 386:913–927. PMID: 26004339.
Article37. Neychev V, Steinberg SM, Yang L, Mehta A, Nilubol N, Keil MF, et al. Long-term outcome of bilateral laparoscopic adrenalectomy measured by disease-specific questionnaire in a unique group of patients with Cushing's syndrome. Ann Surg Oncol. 2015; 22 Suppl 3:S699–S706. PMID: 25968622.
Article38. Nieman LK. Cushing's syndrome: update on signs, symptoms and biochemical screening. Eur J Endocrinol. 2015; 173:M33–M38. PMID: 26156970.
Article39. Nieman LK, Biller BM, Findling JW, Murad MH, Newell-Price J, Savage MO, et al. Treatment of Cushing's syndrome: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2015; 100:2807–2831. PMID: 26222757.
Article40. Reimondo G, Puglisi S, Pia A, Terzolo M. Autonomous hypercortisolism: definition and clinical implications. Minerva Endocrinol. 2019; 44:33–42. PMID: 29963828.
Article41. Sydney GI, Ioakim KJ, Paschou SA. Insulin resistance and adrenal incidentalomas: a bidirectional relationship. Maturitas. 2019; 121:1–6. PMID: 30704559.
Article42. Belmihoub I, Silvera S, Sibony M, Dousset B, Legmann P, Bertagna X, et al. From benign adrenal incidentaloma to adrenocortical carcinoma: an exceptional random event. Eur J Endocrinol. 2017; 176:K15–K19. PMID: 28348073.
Article43. Bernard MH, Sidhu S, Berger N, Peix JL, Marsh DJ, Robinson BG, et al. A case report in favor of a multistep adrenocortical tumorigenesis. J Clin Endocrinol Metab. 2003; 88:998–1001. PMID: 12629075.
Article44. Ozsari L, Kutahyalioglu M, Elsayes KM, Vicens RA, Sircar K, Jazaerly T, et al. Preexisting adrenal masses in patients with adrenocortical carcinoma: clinical and radiological factors contributing to delayed diagnosis. Endocrine. 2016; 51:351–359. PMID: 26206754.
Article45. Nogueira TM, Lirov R, Caoili EM, Lerario AM, Miller BS, Fragoso MC, et al. Radiographic characteristics of adrenal masses preceding the diagnosis of adrenocortical cancer. Horm Cancer. 2015; 6:176–181. PMID: 26021762.
Article46. Luft FC. Inherited colon cancer as an example of a multistep process model. J Mol Med (Berl). 1996; 74:487–488. PMID: 8892052.
Article47. Al-Sohaily S, Biankin A, Leong R, Kohonen-Corish M, Warusavitarne J. Molecular pathways in colorectal cancer. J Gastroenterol Hepatol. 2012; 27:1423–1431. PMID: 22694276.
Article48. Tissier F, Cavard C, Groussin L, Perlemoine K, Fumey G, Hagnere AM, et al. Mutations of beta-catenin in adrenocortical tumors: activation of the Wnt signaling pathway is a frequent event in both benign and malignant adrenocortical tumors. Cancer Res. 2005; 65:7622–7627. PMID: 16140927.49. Bonnet-Serrano F, Bertherat J. Genetics of tumors of the adrenal cortex. Endocr Relat Cancer. 2018; 25:R131–R152. PMID: 29233839.
Article50. Heaton JH, Wood MA, Kim AC, Lima LO, Barlaskar FM, Almeida MQ, et al. Progression to adrenocortical tumorigenesis in mice and humans through insulin-like growth factor 2 and β-catenin. Am J Pathol. 2012; 181:1017–1033. PMID: 22800756.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Adrenal Incidentaloma: Imaging Approach and Differential Diagnosis
- Recent Updates on the Management of Adrenal Incidentalomas
- A 5-Year Prospective Follow-Up Study of Lipid-Rich Adrenal Incidentalomas: No Tumor Growth or Development of Hormonal Hypersecretion
- Differential Diagnosis of Adrenal Mass Using Imaging Modality: Special Emphasis on F-18 Fluoro-2-Deoxy-D-Glucose Positron Emission Tomography/Computed Tomography
- Clinical Characteristics and Metabolic Features of Patients with Adrenal Incidentalomas with or without Subclinical Cushing's Syndrome
