Performance of F-18 Fluorocholine PET/CT for Detection of Hyperfunctioning Parathyroid Tissue in Patients with Elevated Parathyroid Hormone Levels and Negative or Discrepant Results in conventional Imaging
- Uslu-BeÅŸli L

- Sonmezoglu K
- Teksoz S
- Akgun E
- Karayel E
- Pehlivanoglu H
- Khosroshahi BR
- Ocak M
- Kabasakal
- Sager S
- Bukey Y
- Affiliations
-
- 1Department of Nuclear Medicine, Istanbul University-Cerrahpasa, Cerrahpasa Medical Faculty, Istanbul, Turkey. drkerim@istanbul.edu.tr
- 2Department of General Surgery, Istanbul University-Cerrahpasa, Cerrahpasa Medical Faculty, Istanbul, Turkey.
- 3Department of Nuclear Medicine, Division of Radiopharmacy, Istanbul University-Cerrahpasa, Cerrahpasa Medical Faculty, Istanbul, Turkey.
- 4Department of Pharmaceutical Technology, Istanbul University, Pharmacy Faculty, Istanbul, Turkey.
- KMID: 2471641
- DOI: http://doi.org/10.3348/kjr.2019.0268
Abstract
OBJECTIVE
Our aim was to assess the diagnostic performance of F-18 fluorocholine (FCH) positron emission tomography/computed tomography (PET/CT) in detecting hyperfunctioning parathyroid tissue (HPT) in patients with elevated parathyroid hormone levels with negative or inconclusive conventional imaging results and to compare the findings with those obtained using technetium-99m sestamibi (MIBI) scintigraphy and neck ultrasonography (US).
MATERIALS AND METHODS
Images of 105 patients with hyperparathyroidism who underwent FCH PET/CT, dual-phase MIBI parathyroid scintigraphy (median interval: 42 days), and neck US were retrospectively analyzed. The gold standard was histopathological findings for 81 patients who underwent parathyroidectomy and clinical follow-up findings in the remaining 24 patients. Sensitivities, positive predictive values (PPVs), and accuracies were calculated for all imaging modalities.
RESULTS
Among the 81 patients who underwent parathyroidectomy, either parathyroid adenoma (n = 64), hyperplasia (n = 9), neoplasia (n = 4), or both parathyroid adenoma and hyperplasia (n = 1) were detected, except 3 patients who did not show HPT. Of the 24 (23%) patients who were followed-up without operation, 22 (92%) showed persistent hyperparathyroidism. FCH PET/CT showed significantly higher sensitivity than MIBI scintigraphy and US in detection of HPT (p < 0.01). Sensitivity, PPV, and accuracy of FCH PET/CT were 94.1% (95/101), 97.9% (95/97), and 92.4% (97/105), respectively. The corresponding values for MIBI scintigraphy and US were 45.1% (46/102), 97.9% (46/47), and 45.7% (48/105) and 44.1% (45/102), 93.8% (45/48), and 42.9% (45/105), respectively. Among the 35 patients showing negative MIBI scintigraphy and neck US findings, 30 (86%) showed positive results on FCH PET/CT. FCH PET/CT could demonstrate ectopic locations of HPT in 11 patients whereas MIBI and US showed positive findings in only 6 and 3 patients, respectively.
CONCLUSION
FCH PET/CT is an effective imaging modality for detection of HPT with the highest sensitivity among the available imaging techniques. Therefore, FCH PET/CT can be recommended especially for patients who show negative or inconclusive results on conventional imaging.
Keyword
MeSH Terms
Figure
-
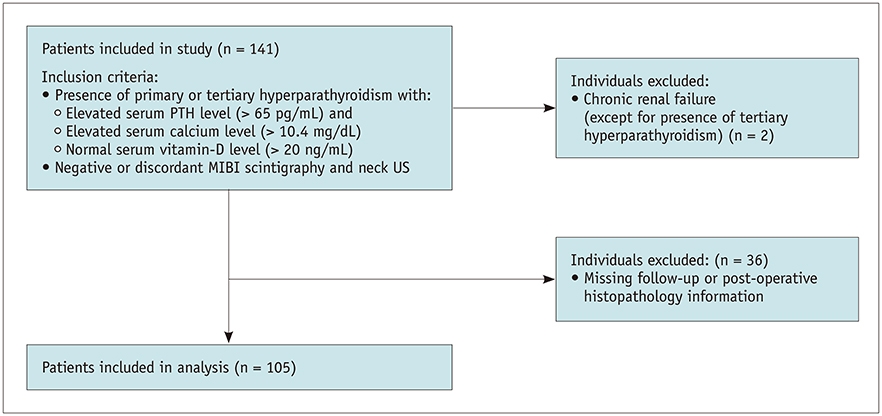
Fig. 1 Flow chart showing patient selection process. MIBI = technetium-99m sestamibi, n = number of patients, PTH = parathyroid hormone, US = ultrasonography
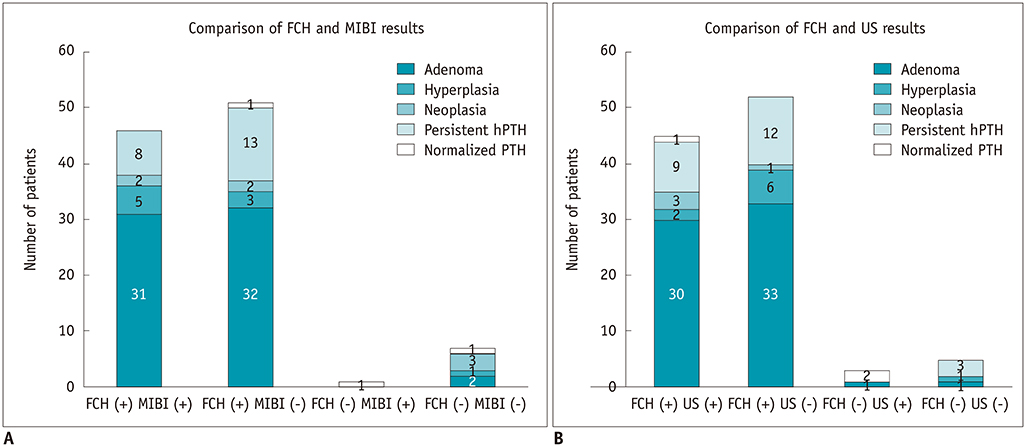
Fig. 2 Distribution of concordant and discordant cases between FCH PET/CT and MIBI scintigraphy (A) and neck ultrasonography (B) according to patients' final status based on findings from postoperative histopathological assessments or clinical follow-up examinations. FCH = fluorine-18 fluorocholine, hPTH = persistent raised PTH, PET/CT = positron emission tomography/computed tomography
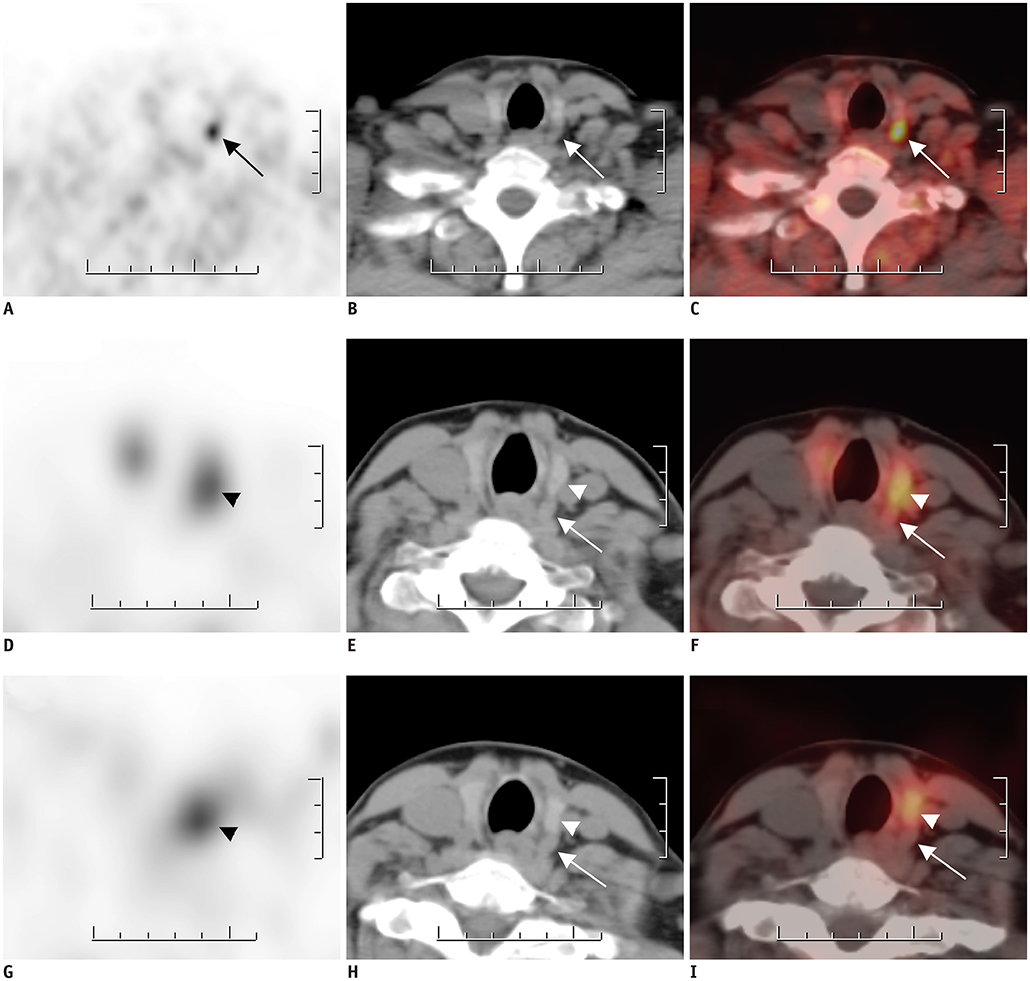
Fig. 3 FCH PET/CT (A–C) and MIBI SPECT/CT (D–I) findings for 48-year-old female with hyperparathyroidism (PTH level: 191 pg/mL). FCH PET (A), CT (B), and fused PET/CT (C) images in FCH PET/CT reveal nodular lesion with intense FCH uptake (arrows) posterior to left thyroid lobe, which was confirmed to be parathyroid adenoma. Patient also showed papillary thyroid microcarcinoma in left thyroid lobe with no FCH uptake. In early MIBI SPECT (D), CT (E), and fused SPECT/CT (F) images, MIBI uptake was noted on left thyroid lobe. Moreover, MIBI uptake persisted in late SPECT (G), CT (H), and fused SPECT/CT (I) images (arrowheads). However, parathyroid lesion posterior to left thyroid lobe did not exhibit any MIBI uptake in early and late SPECT/CT scans (arrows). SPECT = single-photon emission computed tomography
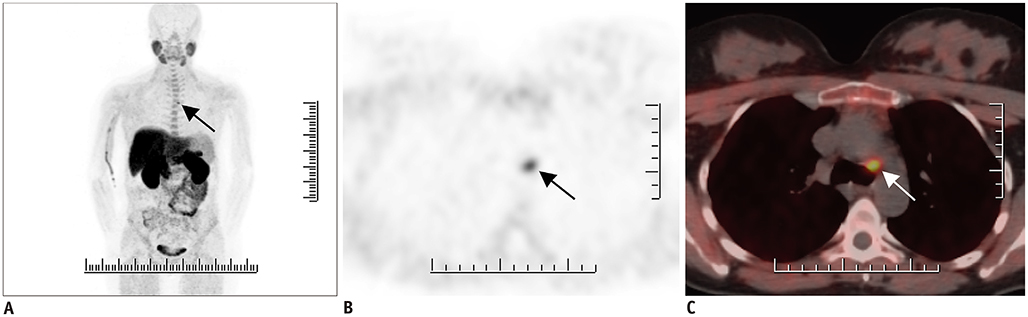
Fig. 4 39-year-old female patient with hyperparathyroidism (PTH level: 203.0 pg/mL) showing negative MIBI and ultrasonography results (not shown). FCH PET/CT MIP image (A) shows focus of FCH uptake on upper mediastinum (arrow). Axial PET (B) and fused PET/CT (C) images reveal 1-cm nodular lesion with intense FCH uptake in aortopulmonary window (arrows). Postoperative histopathology revealed presence of ectopic mediastinal parathyroid adenoma. MIP = maximum intensity projection
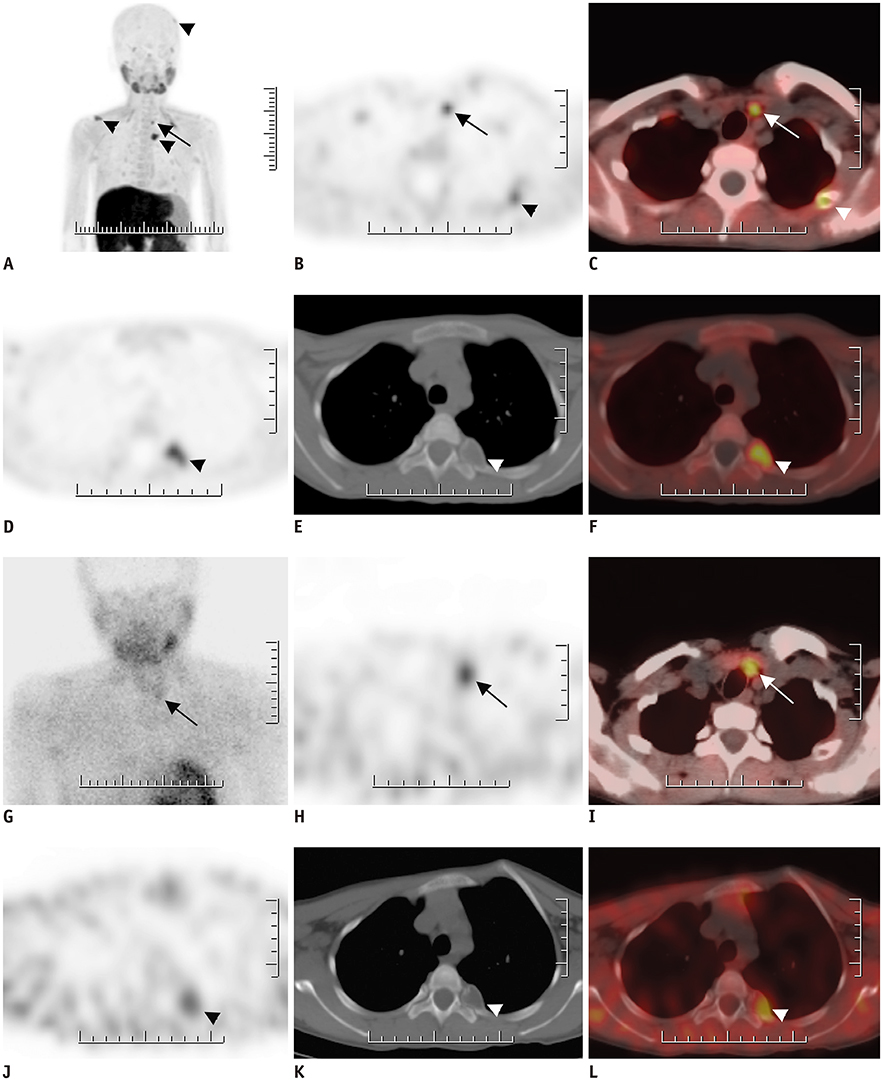
Fig. 5 16-year-old female patient with chronic renal failure. A–F. FCH PET/CT MIP image (A) reveals multiple foci of increased FCH uptake. Axial PET (B) and fused PET/CT (C) images on lower neck region reveal intense FCH uptake on left side that was found to be in accordance with parathyroid adenoma in surgical specimen (arrows). Brown tumors also demonstrate increased FCH uptake (arrowheads). G–L. MIBI SPECT/CT images of same patient. MIBI uptake at late planar (G), SPECT (H), and fused SPECT/CT (I) images reveal MIBI uptake on parathyroid adenoma (arrows). Brown tumors also demonstrate increased MIBI uptake (arrow heads).
Reference
-
1. Wilhelm SM, Wang TS, Ruan DT, Lee JA, Asa SL, Duh QY, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. 2016; 151:959–968.
Article2. Ciappuccini R, Morera J, Pascal P, Rame JP, Heutte N, Aide N, et al. Dual-phase 99mTc sestamibi scintigraphy with neck and thorax SPECT/CT in primary hyperparathyroidism: a single-institution experience. Clin Nucl Med. 2012; 37:223–228.3. Hunter GJ, Schellingerhout D, Vu TH, Perrier ND, Hamberg LM. Accuracy of four-dimensional CT for the localization of abnormal parathyroid glands in patients with primary hyperparathyroidism. Radiology. 2012; 264:789–795.
Article4. Nael K, Hur J, Bauer A, Khan R, Sepahdari A, Inampudi R, et al. Dynamic 4D MRI for characterization of parathyroid adenomas: multiparametric analysis. AJNR Am J Neuroradiol. 2015; 36:2147–2152.
Article5. Mahajan A, Starker LF, Ghita M, Udelsman R, Brink JA, Carling T. Parathyroid four-dimensional computed tomography: evaluation of radiation dose exposure during preoperative localization of parathyroid tumors in primary hyperparathyroidism. World J Surg. 2012; 36:1335–1339.
Article6. Quak E, Lheureux S, Reznik Y, Bardet S, Aide N. F18-choline, a novel PET tracer for parathyroid adenoma? J Clin Endocrinol Metab. 2013; 98:3111–3112.
Article7. Lezaic L, Rep S, Sever MJ, Kocjan T, Hocevar M, Fettich J. 18F-Fluorocholine PET/CT for localization of hyperfunctioning parathyroid tissue in primary hyperparathyroidism: a pilot study. Eur J Nucl Med Mol Imaging. 2014; 41:2083–2089.8. Kluijfhout WP, Vorselaars WM, Vriens MR, Borel Rinkes IH, Valk GD, de Keizer B. Enabling minimal invasive parathyroidectomy for patients with primary hyperparathyroidism using Tc-99m-sestamibi SPECT-CT, ultrasound and first results of (18) F-fluorocholine PET-CT. Eur J Radiol. 2015; 84:1745–1751.9. Michaud L, Balogova S, Burgess A, Ohnona J, Huchet V, Kerrou K, et al. A pilot comparison of 18F-fluorocholine PET/CT, ultrasonography and 123I/99mTc-sestaMIBI dual-phase dual-isotope scintigraphy in the preoperative localization of hyperfunctioning parathyroid glands in primary or secondary hyperparathyroidism: influence of thyroid anomalies. Medicine (Baltimore). 2015; 94:e1701.10. Kluijfhout WP, Vorselaars WM, van den Berk SA, Vriens MR, Borel Rinkes IH, Valk GD, et al. Fluorine-18 fluorocholine PET-CT localizes hyperparathyroidism in patients with inconclusive conventional imaging: a multicenter study from the Netherlands. Nucl Med Commun. 2016; 37:1246–1252.11. Thanseer N, Bhadada SK, Sood A, Mittal BR, Behera A, Gorla AKR, et al. Comparative effectiveness of ultrasonography, 99mTc-sestamibi, and 18F-fluorocholine PET/CT in detecting parathyroid adenomas in patients with primary hyperparathyroidism. Clin Nucl Med. 2017; 42:e491–e497.
Article12. Michaud L, Burgess A, Huchet V, Lefèvre M, Tassart M, Ohnona J, et al. Is 18F-fluorocholine-positron emission tomography/computerized tomography a new imaging tool for detecting hyperfunctioning parathyroid glands in primary or secondary hyperparathyroidism? J Clin Endocrinol Metab. 2014; 99:4531–4536.
Article13. Kryza D, Tadino V, Filannino MA, Villeret G, Lemoucheux L. Fully automated [18F]fluorocholine synthesis in the TracerLab MX FDG coincidence synthesizer. Nucl Med Biol. 2008; 35:255–260.14. Rep S, Lezaic L, Kocjan T, Pfeifer M, Sever MJ, Simoncic U, et al. Optimal scan time for evaluation of parathyroid adenoma with [(18)F]-fluorocholine PET/CT. Radiol Oncol. 2015; 49:327–333.
Article15. Hocevar M, Lezaic L, Rep S, Zaletel K, Kocjan T, Sever MJ, et al. Focused parathyroidectomy without intraoperative parathormone testing is safe after pre-operative localization with 18F-fluorocholine PET/CT. Eur J Surg Oncol. 2017; 43:133–137.
Article16. Huber GF, Hüllner M, Schmid C, Brunner A, Sah B, Vetter D, et al. Benefit of 18F-fluorocholine PET imaging in parathyroid surgery. Eur Radiol. 2018; 28:2700–2707.
Article17. Quak E, Blanchard D, Houdu B, Le Roux Y, Ciappuccini R, Lireux B, et al. F18-choline PET/CT guided surgery in primary hyperparathyroidism when ultrasound and MIBI SPECT/CT are negative or inconclusive: the APACH1 study. Eur J Nucl Med Mol Imaging. 2018; 45:658–666.
Article18. Kim SJ, Lee SW, Jeong SY, Pak K, Kim K. Diagnostic performance of F-18 fluorocholine PET/CT for parathyroid localization in hyperparathyroidism: a systematic review and meta-analysis. Horm Cancer. 2018; 9:440–447.
Article19. Treglia G, Piccardo A, Imperiale A, Strobel K, Kaufmann PA, Prior JO, et al. Diagnostic performance of choline PET for detection of hyperfunctioning parathyroid glands in hyperparathyroidism: a systematic review and meta-analysis. Eur J Nucl Med Mol Imaging. 2019; 46:751–765.
Article20. Kluijfhout WP, Pasternak JD, Gosnell JE, Shen WT, Duh QY, Vriens MR, et al. 18F fluorocholine PET/MR imaging in patients with primary hyperparathyroidism and inconclusive conventional imaging: a prospective pilot study. Radiology. 2017; 284:460–467.
Article21. Lavely WC, Goetze S, Friedman KP, Leal JP, Zhang Z, Garret-Mayer E, et al. Comparison of SPECT/CT, SPECT, and planar imaging with single- and dual-phase (99m)Tc-sestamibi parathyroid scintigraphy. J Nucl Med. 2007; 48:1084–1089.
Article22. Cheung K, Wang TS, Farrokhyar F, Roman SA, Sosa JA. A meta-analysis of preoperative localization techniques for patients with primary hyperparathyroidism. Ann Surg Oncol. 2012; 19:577–583.
Article23. Smith RB, Evasovich M, Girod DA, Jorgensen JB, Lydiatt WM, Pagedar NA, et al. Ultrasound for localization in primary hyperparathyroidism. Otolaryngol Head Neck Surg. 2013; 149:366–371.
Article24. Uslu L, Calis¸kan A, Sağer S, Teksöz S, Halaç M. Preoperative and postoperative 18FDG PET/CT and bone scintigraphy images in a patient with parathyroid adenoma. Clin Nucl Med. 2013; 38:456–458.
Article25. van Baardwijk A, de Jong J, Arens A, Thimister P, Verseput G, Kremer B, et al. False-positive FDG-PET scan due to brown tumours. Eur J Nucl Med Mol Imaging. 2006; 33:393–394.
Article26. Vaishya R, Agarwal AK, Singh H, Vijay V. Multiple ‘brown tumors’ masquerading as metastatic bone disease. Cureus. 2015; 7:e431.
Article27. Taywade SK, Damle NA, Behera A, Devasenathipathy K, Bal C, Tripathi M, et al. Comparison of 18F-fluorocholine positron emission tomography/computed tomography and four-dimensional computed tomography in the preoperative localization of parathyroid adenomas-initial results. Indian J Endocrinol Metab. 2017; 21:399–403.28. O'Doherty MJ, Kettle AG, Wells P, Collins RE, Coakley AJ. Parathyroid imaging with technetium-99m-sestamibi: preoperative localization and tissue uptake studies. J Nucl Med. 1992; 33:313–318.29. Piwnica-Worms D, Chiu ML, Budding M, Kronauge JF, Kramer RA, Croop JM. Functional imaging of multidrug-resistant P-glycoprotein with an organotechnetium complex. Cancer Res. 1993; 53:977–984.30. Ratnam S, Kent C. Early increase in choline kinase activity upon induction of the H-ras oncogene in mouse fibroblast cell lines. Arch Biochem Biophys. 1995; 323:313–322.31. Glunde K, Bhujwalla ZM, Ronen SM. Choline metabolism in malignant transformation. Nat Rev Cancer. 2011; 11:835–848.
Article32. Ishizuka T, Kajita K, Kamikubo K, Komaki T, Miura K, Nagao S, et al. Phospholipid/Ca2+-dependent protein kinase activity in human parathyroid adenoma. Endocrinol Jpn. 1987; 34:965–968.
Article33. van der Hiel B, Stokkel MPM, Buikhuisen WA, Janssen H, van Velthuysen MLF, Rhodius RJ, et al. 18F-choline PET/CT as a new tool for functional imaging of non-proliferating secreting neuroendocrine tumors. J Endocrinol Metab. 2015; 5:267–271.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hyperfunctioning Intrathyroidal Parathyroid: a Misleading Preoperative Diagnosis
- Dual Pathologies of Parathyroid Adenoma and Papillary Thyroid Cancer on Fluorocholine and Fluorodeoxyglucose PET/CT
- Sensitive Detection of a Small Parathyroid Adenoma Using Fluorocholine PET/CT: A Case Report
- The Parathyroid Gland: An Overall Review of the Hidden Organ for Radiologists
- Intraoperative Parathyroid Hormone Monitoring in the Surgical Management of Sporadic Primary Hyperparathyroidism
