Role of Carotid Artery Stenting in Prevention of Stroke for Asymptomatic Carotid Stenosis: Bayesian Cross-Design and Network Meta-Analyses
- Affiliations
-
- 1Department of Cardiology in Internal Medicine, School of Medicine, Chungnam National University, Chungnam National University Hospital, Daejeon, Korea. myheart@cnu.ac.kr
- 2Department of Cardiology, Daegu Fatima Hospital, Daegu, Korea.
- 3Department of Statistics, Kyungpook National University, Daegu, Korea.
- 4Division of Cardiology, Department of Internal Medicine, Korea University Medical Center Anam Hospital, Seoul, Korea.
- KMID: 2471283
- DOI: http://doi.org/10.4070/kcj.2019.0125
Abstract
- BACKGROUND AND OBJECTIVES
There is insufficient evidence regarding the optimal treatment for asymptomatic carotid stenosis.
METHODS
Bayesian cross-design and network meta-analyses were performed to compare the safety and efficacy among carotid artery stenting (CAS), carotid endarterectomy (CEA), and medical treatment (MT). We identified 18 studies (4 randomized controlled trials [RCTs] and 14 nonrandomized, comparative studies [NRCSs]) comparing CAS with CEA, and 4 RCTs comparing CEA with MT from MEDLINE, Cochrane Library, and Embase databases.
RESULTS
The risk for periprocedural stroke tended to increase in CAS, compared to CEA (odds ratio [OR], 1.86; 95% credible interval [CrI], 0.62-4.54). However, estimates for periprocedural myocardial infarction (MI) were quite heterogeneous in RCTs and NRCSs. Despite a trend of decreased risk with CAS in RCTs (OR, 0.70; 95% CrI, 0.27-1.24), the risk was similar in NRCSs (OR, 1.02; 95% CrI, 0.87-1.18). In indirect comparisons of MT and CAS, MT showed a tendency to have a higher risk for the composite of periprocedural death, stroke, MI, or nonperiprocedural ipsilateral stroke (OR, 1.30; 95% CrI, 0.74-2.73). Analyses of study characteristics showed that CEA-versus-MT studies took place about 10-year earlier than CEA-versus-CAS studies.
CONCLUSIONS
A similar risk for periprocedural MI between CEA and CAS in NRCSs suggested that concerns about periprocedural MI accompanied by CEA might not matter in real-world practice when preoperative evaluation and management are working. Maybe the benefits of CAS over MT have been overestimated considering advances in medical therapy within10-year gap between CEA-versus-MT and CEA-versus-CAS studies.
MeSH Terms
Figure
-
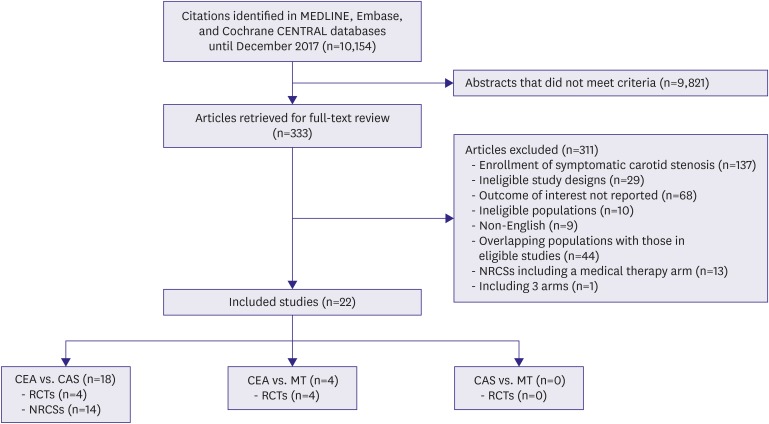
Figure 1 Summary of evidence search and selection.CAS = carotid artery stenting; CEA = carotid endarterectomy; CENTRAL = Central Register of Controlled Trials; MT = medical treatment; NRCS = nonrandomized comparative study; RCT = randomized controlled trial.
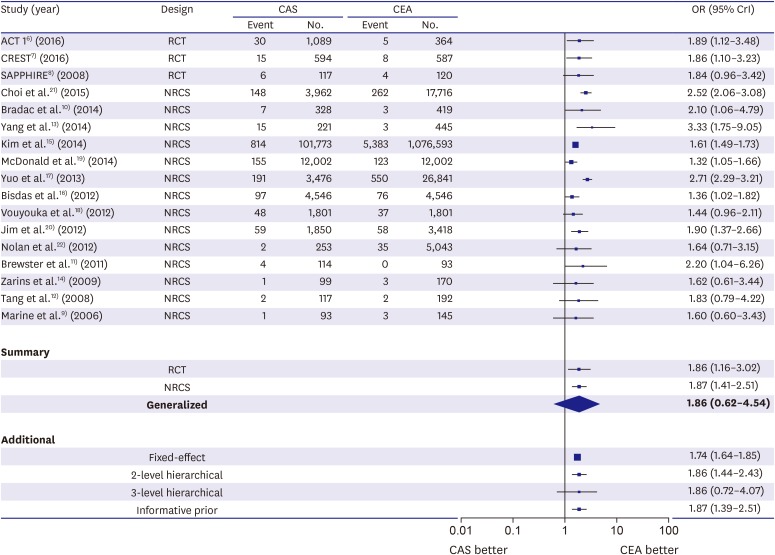
Figure 2 The risk of any periprocedural stroke with stenting versus endarterectomy. Data are expressed on a logarithmic scale. The size of central markers reflects the weight of each study.ACT 1 = Asymptomatic Carotid Trial; CAS = carotid artery stenting; CEA = carotid endarterectomy; CREST = Carotid Revascularization Endarterectomy versus Stenting Trial; CrI = credible interval; NRCS = nonrandomized comparative study; OR = odds ratio; RCT = randomized controlled trial; SAPPHIRE = Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy.
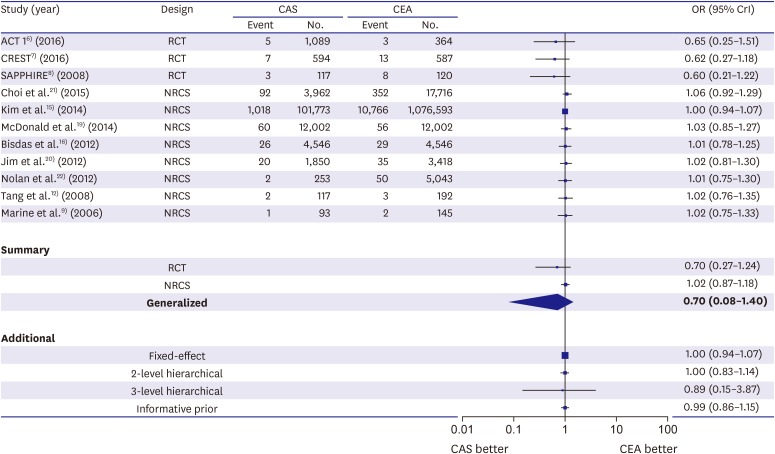
Figure 3 The risk of periprocedural myocardial infarction with stenting versus endarterectomy. Data are expressed on a logarithmic scale. The size of central markers reflects the weight of each study.ACT 1 = Asymptomatic Carotid Trial; CAS = carotid artery stenting; CEA = carotid endarterectomy; CREST = Carotid Revascularization Endarterectomy versus Stenting Trial; CrI = credible interval; NRCS = nonrandomized comparative study; OR = odds ratio; RCT = randomized controlled trial; SAPPHIRE = Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy.
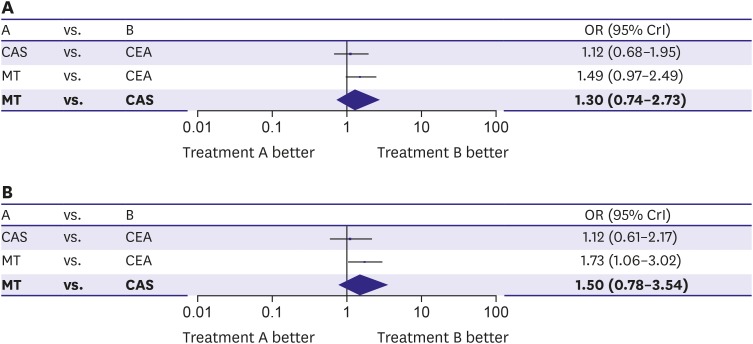
Figure 4 Stenting versus medical treatment for asymptomatic carotid stenosis. Data are expressed on a logarithmic scale. (A) The composite of death, stroke, or myocardial infarction during periprocedural period and ipsilateral stroke during long-term follow-up. (B) The risk for any periprocedural stroke plus nonperiprocedural ipsilateral stroke. The size of central markers reflects the weight of each study.CAS = carotid artery stenting; CEA = carotid endarterectomy; CrI = credible interval; MT = medical treatment; OR = odds ratio.
Cited by 1 articles
-
Reassembling Evidence for Treatment in Asymptomatic Carotid Artery Stenosis
Hyung Oh Kim, Weon Kim
Korean Circ J. 2020;50(4):343-345. doi: 10.4070/kcj.2020.0023.
Reference
-
1. Kartchner MM, McRae LP. Noninvasive evaluation and management of the “asymptomatic” carotid bruit. Surgery. 1977; 82:840–847. PMID: 929374.2. Aboyans V, Ricco JB, Bartelink ME, et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries endorsed by: the European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur Heart J. 2018; 39:763–816. PMID: 28886620.3. Prevost TC, Abrams KR, Jones DR. Hierarchical models in generalized synthesis of evidence: an example based on studies of breast cancer screening. Stat Med. 2000; 19:3359–3376. PMID: 11122501.4. Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med. 2004; 23:3105–3124. PMID: 15449338.5. Kougias P, Collins R, Pastorek N, et al. Comparison of domain-specific cognitive function after carotid endarterectomy and stenting. J Vasc Surg. 2015; 62:355–361. PMID: 26211378.6. Rosenfield K, Matsumura JS, Chaturvedi S, et al. Randomized Trial of Stent versus Surgery for Asymptomatic Carotid Stenosis. N Engl J Med. 2016; 374:1011–1020. PMID: 26886419.7. Brott TG, Howard G, Roubin GS, et al. Long-term results of stenting versus endarterectomy for carotid-artery stenosis. N Engl J Med. 2016; 374:1021–1031. PMID: 26890472.8. Gurm HS, Yadav JS, Fayad P, et al. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med. 2008; 358:1572–1579. PMID: 18403765.9. Marine LA, Rubin BG, Reddy R, Sanchez LA, Parodi JC, Sicard GA. Treatment of asymptomatic carotid artery disease: similar early outcomes after carotid stenting for high-risk patients and endarterectomy for standard-risk patients. J Vasc Surg. 2006; 43:953–958. PMID: 16678689.10. Bradac O, Mohapl M, Kramar F, et al. Carotid endarterectomy and carotid artery stenting: changing paradigm during 10 years in a high-volume centre. Acta Neurochir (Wien). 2014; 156:1705–1712. PMID: 25011733.11. Brewster LP, Beaulieu R, Corriere MA, et al. Carotid revascularization outcomes comparing distal filters, flow reversal, and endarterectomy. J Vasc Surg. 2011; 54:1000–1004. PMID: 21871772.12. Tang GL, Matsumura JS, Morasch MD, et al. Carotid angioplasty and stenting vs carotid endarterectomy for treatment of asymptomatic disease: single-center experience. Arch Surg. 2008; 143:653–658. PMID: 18645107.13. Yang SS, Kim YW, Kim DI, et al. Impact of contralateral carotid or vertebral artery occlusion in patients undergoing carotid endarterectomy or carotid artery stenting. J Vasc Surg. 2014; 59:749–755. PMID: 24360588.14. Zarins CK, White RA, Diethrich EB, et al. Carotid revascularization using endarterectomy or stenting systems (CaRESS): 4-year outcomes. J Endovasc Ther. 2009; 16:397–409. PMID: 19702339.15. Kim LK, Yang DC, Swaminathan RV, et al. Comparison of trends and outcomes of carotid artery stenting and endarterectomy in the United States, 2001 to 2010. Circ Cardiovasc Interv. 2014; 7:692–700. PMID: 25116802.16. Bisdas T, Egorova N, Moskowitz AJ, et al. The impact of gender on in-hospital outcomes after carotid endarterectomy or stenting. Eur J Vasc Endovasc Surg. 2012; 44:244–250. PMID: 22819738.17. Yuo TH, Degenholtz HS, Chaer RA, Kraemer KL, Makaroun MS. Effect of hospital-level variation in the use of carotid artery stenting versus carotid endarterectomy on perioperative stroke and death in asymptomatic patients. J Vasc Surg. 2013; 57:627–634. PMID: 23312937.18. Vouyouka AG, Egorova NN, Sosunov EA, et al. Analysis of Florida and New York state hospital discharges suggests that carotid stenting in symptomatic women is associated with significant increase in mortality and perioperative morbidity compared with carotid endarterectomy. J Vasc Surg. 2012; 56:334–342. PMID: 22583852.19. McDonald RJ, McDonald JS, Therneau TM, Lanzino G, Kallmes DF, Cloft HJ. Comparative effectiveness of carotid revascularization therapies: evidence from a National Hospital Discharge Database. Stroke. 2014; 45:3311–3319. PMID: 25300973.20. Jim J, Rubin BG, Ricotta JJ 2nd, et al. Society for Vascular Surgery (SVS) Vascular Registry evaluation of comparative effectiveness of carotid revascularization procedures stratified by Medicare age. J Vasc Surg. 2012; 55:1313–1320. PMID: 22459755.21. Choi JC, Johnston SC, Kim AS. Early outcomes after carotid artery stenting compared with endarterectomy for asymptomatic carotid stenosis. Stroke. 2015; 46:120–125. PMID: 25424479.22. Nolan BW, De Martino RR, Goodney PP, et al. Comparison of carotid endarterectomy and stenting in real world practice using a regional quality improvement registry. J Vasc Surg. 2012; 56:990–996. PMID: 22579135.23. Walker MD, Marler JR, Goldstein M, et al. Endarterectomy for asymptomatic carotid artery stenosis. JAMA. 1995; 273:1421–1428. PMID: 7723155.24. Hobson RW 2nd, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. N Engl J Med. 1993; 328:221–227. PMID: 8418401.25. Halliday A, Harrison M, Hayter E, et al. 10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): a multicentre randomised trial. Lancet. 2010; 376:1074–1084. PMID: 20870099.26. Kolos I, Troitskiy A, Balakhonova T, et al. Modern medical treatment with or without carotid endarterectomy for severe asymptomatic carotid atherosclerosis. J Vasc Surg. 2015; 62:914–922. PMID: 26410046.27. Raman G, Moorthy D, Hadar N, et al. Management strategies for asymptomatic carotid stenosis: a systematic review and meta-analysis. Ann Intern Med. 2013; 158:676–685. PMID: 23648949.28. Sardar P, Chatterjee S, Aronow HD, et al. Carotid artery stenting versus endarterectomy for stroke prevention: a meta-analysis of clinical trials. J Am Coll Cardiol. 2017; 69:2266–2275. PMID: 28473130.29. Song F, Xiong T, Parekh-Bhurke S, et al. Inconsistency between direct and indirect comparisons of competing interventions: meta-epidemiological study. BMJ. 2011; 343:d4909. PMID: 21846695.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carotid Artery Stenting for Asymptomatic Carotid Stenosis: What We Need to Know for Treatment Decision
- Carotid Artery Stenting
- A Case of Transseptal Approach to Carotid Artery Stenting in Right Internal Carotid Stenosis
- Current Indications of Surgery and Endovascular Treatment in Ischemic Stroke
- Percutaneous Transluminal Angioplasty with Palmaz-Schatz Stent in the Carotid Artery Stenosis
