Ann Surg Treat Res.
2020 Mar;98(3):111-115. 10.4174/astr.2020.98.3.111.
Separate thyrothymic thyroid remnant; clinically crucial anatomic variation
- Affiliations
-
- 1Department of Surgery, Duzce University Medical Faculty, Duzce, Turkey. egurleyik@yahoo.com
- 2Department of Surgery, Haydarpasa Numune Teaching Hospital, Health Sciences University, Istanbul, Turkey.
- KMID: 2471175
- DOI: http://doi.org/10.4174/astr.2020.98.3.111
Abstract
- PURPOSE
The anatomical variations of the thyroid gland including separate thyroidal remnant at the thyrothymic area are of significance during thyroid surgery for "total" thyroidectomy, and for recurrent goitre. In the present study, we aimed to detect the separate rests of thyroidal tissue in the thyrothymic region.
METHODS
The thyrothymic region was explored for identification, dissection, and excision of separate thyroidal remnants in 134 patients who underwent primary thyroid surgery. In this series, we studied the incidence and anatomical features of the thyrothymic remnant and its relation with other embryologic remnants.
RESULTS
Overall, 222 sides of the thyroid were explored in this study. An entirely separate thyrothymic remnant of the thyroid was identified and excised in 8 of 134 patients (6%). Mean size of removed remnants was 36.4 mm (range, 29-45 mm) in diameter. The incidences of pyramidal lobe (PL) and Zuckerkandl's tubercle (ZT) were 71.6% and 59.7%, respectively. The thyrothymic remnant coexisted with PLs in 4 patients. Four patients had all 3 embryologic remnants: thyrothymic remnant, PLs, and ZTs.
CONCLUSION
An entirely separate thyroidal remnant at the thyrothymic area is not a rare variation. The considerably large size of a remnant may threaten the completeness of thyroidectomy and may result in recurrence if it is left behind after thyroid surgery. Awareness, identification, and excision of the separate remnant at the thyrothymic area and the other embryologic remnants are critical for ensuring completeness of thyroidectomy and preventing recurrences.
Figure
-
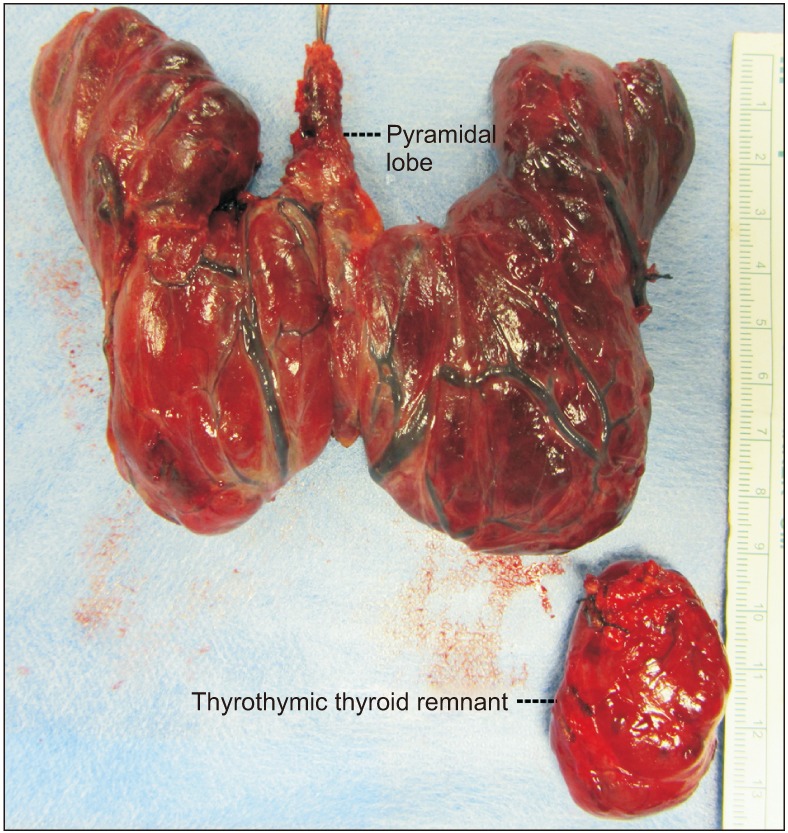
Fig. 1 Total thyroidectomy specimen with 2 embryologic remnants; the thyroid gland with pyramidal lobe and thyrothymic thyroidal remnant adjacent to lower pole of the left lobe. Largest separate thyroidal remnant at left thyrothymic tract.
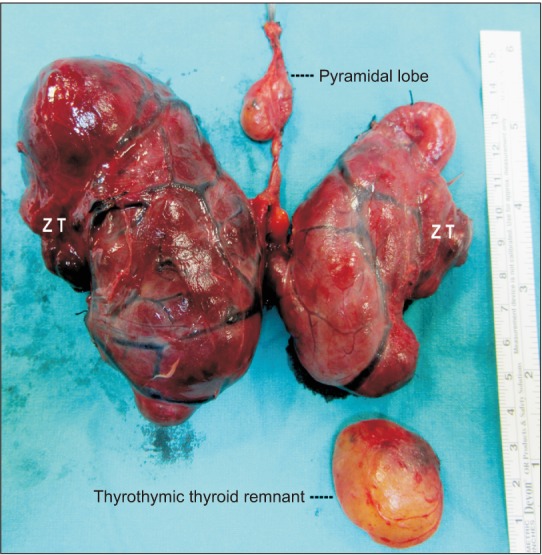
Fig. 2 Total thyroidectomy specimen with all 3 embryologic remnants; the thyroid gland with pyramidal lobe and bilateral Zuckerkandl's tubercles (ZT), and separate thyroidal remnant at left thyrothymic tract.
Reference
-
1. Fernando R, Rajapaksha A, Ramasinghe N, Gunawardana D. Embryologic remnants of the thyroid gland and their significance in thyroidectomy. World J Endocr Surg. 2014; 6:110–112.2. Sackett WR, Reeve TS, Barraclough B, Delbridge L. Thyrothymic thyroid rests: incidence and relationship to the thyroid gland. J Am Coll Surg. 2002; 195:635–640. PMID: 12437250.
Article3. Sheahan P, O'Duffy F. Thyroid thyrothymic extension: an anatomic study in a surgical series. Head Neck. 2016; 38:732–735. PMID: 25524573.
Article4. Cilento BW, Futran N. Retroesophageal thyrothymic thyroid rest. Ann Otol Rhinol Laryngol. 2005; 114:416–418. PMID: 15966532.
Article5. Delbridge L. Total thyroidectomy: the evolution of surgical technique. ANZ J Surg. 2003; 73:761–768. PMID: 12956795.
Article6. Gurleyik E, Gurleyik G, Dogan S, Cobek U, Cetin F, Onsal U. Pyramidal lobe of the thyroid gland: surgical anatomy in patients undergoing total thyroidectomy. Anat Res Int. 2015; 2015:384148. PMID: 26236507.
Article7. Benmoussa JA, Shawa H. Pyramidal lobe remnant. Endocr Pract. 2018; 24:396. PMID: 29144821.
Article8. Wang M, Zou X, Li Z, Zhu J. Recurrence of papillary thyroid carcinoma from the residual pyramidal lobe: a case report and literature review. Medicine (Baltimore). 2019; 98:e15210. PMID: 30985719.
Article9. Gurleyik E, Gurleyik G. Incidence and surgical importance of Zuckerkandl's tubercle of the thyroid and its relations with recurrent laryngeal nerve. ISRN Surg. 2012; 2012:450589. PMID: 22957274.
Article10. Snook KL, Stalberg PL, Sidhu SB, Sywak MS, Edhouse P, Delbridge L. Recurrence after total thyroidectomy for benign multinodular goiter. World J Surg. 2007; 31:593–598. PMID: 17308855.
Article11. Vasica G, O'Neill CJ, Sidhu SB, Sywak MS, Reeve TS, Delbridge LW. Reoperative surgery for bilateral multinodular goitre in the era of total thyroidectomy. Br J Surg. 2012; 99:688–692. PMID: 22287186.
Article12. Cunha FM, Rodrigues E, Oliveira J, Saavedra A, Vinhas LS, Carvalho D. Graves' disease in a mediastinal mass presenting after total thyroidectomy for nontoxic multinodular goiter: a case report. J Med Case Rep. 2016; 10:70. PMID: 27029843.
Article13. Sadacharan D, Mahadevan S, Muthukumar S, Dinesh S. Non-elevation of TSH after total thyroidectomy: a surgical surprise. BMJ Case Rep. 2015; 5. 15. 2015:bcr2015209809. DOI: 10.1136/bcr-2015-209809.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Variation in repeated measurements of transepidermal water loss, skin hydration, and sebum level in normal beagle dogs
- Anatomic Variation of the Common Palmar Digital Nerves and Arteries
- Ablation of Remnant Thyroid Tissue with I-131 in Well Differentiated Thyroid Cancer After Surgery
- Anatomic Variants Mimicking Pathology on Echocardiography: Differential Diagnosis
- Papillary Cancer Arising in Remnant Thyroglossal Duct
