J Dent Anesth Pain Med.
2020 Feb;20(1):49-53. 10.17245/jdapm.2020.20.1.49.
Difficult intubation caused by an immature upper airway in a patient with cri-du-chat syndrome: a case report
- Affiliations
-
- 1Department of Anesthesiology, School of Dentistry, Dankook University, Cheonan, Korea. ksomd@naver.com
- KMID: 2471174
- DOI: http://doi.org/10.17245/jdapm.2020.20.1.49
Abstract
- Cri-du-chat syndrome (CdCS) is caused by the deletion of the short arm of chromosome 5. Most patients with CdCS develop intellectual disabilities. Therefore, they have poor oral hygiene and a high caries index. However, treating such patients is not an easy task, because of the difficulty in communication. General anesthesia may be a useful option in adult patients with CdCS and intellectual disability. General anesthesia should be administered very carefully, owing to the presence of comorbid diseases, which may need airway management. Infants with CdCS need general anesthesia if they have a concomitant cardiac anomaly. Intubation is reportedly difficult for such patients was, owing to the structural and functional abnormalities in the larynx and vocal cords. The purpose of this study was to report a case of difficult intubation while inducing general anesthesia in a patient with CdCS during dental treatment, due to a narrow larynx and trachea.
MeSH Terms
Figure
-
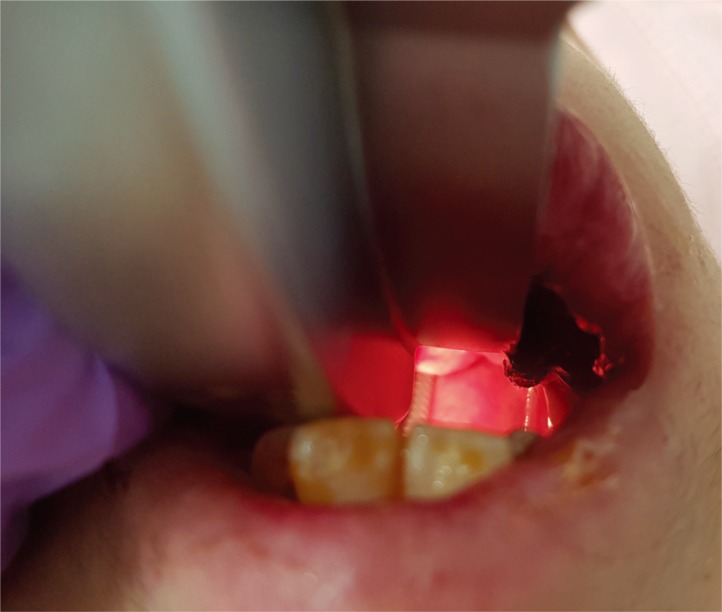
Fig. 1 Laryngoscopic field of view (in the stable condition) after successful intubation using a size 3 Macintosh curved blade. The Cormack-Lehane Grade was 4 before intubation, but intubation could not be delayed to take a photograph.
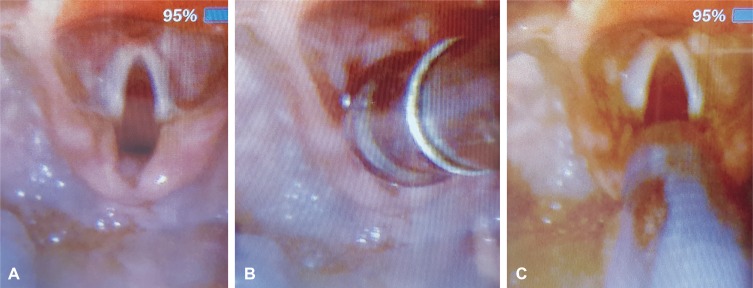
Fig. 2 A: Field of view using video laryngoscopy. A small epiglottis and vocal cord are visible. Vocal cord is fully relaxed. B: The vocal cord is completely covered by Yankauer's suction with an outer diameter of 9.4 mm. C: Intubation with endotracheal tube with an outer diameter of 8.0 mm and an inner diameter of 5.5 mm with a balloon.
Reference
-
1. Niebuhr E. The cri du chat syndrome: Epidemiology, cytogenetics, and clinical features. Hum Genet. 1978; 44:227–275. PMID: 365706.2. Overhauser J, Huang X, Gersh M, Wilson W, McMahon J, Bengtsson U, et al. Molecular and phenotypic mapping of the short arm of chromosome 5: Sublocalization of the critical region for the cri-du-chat syndrome. Hum Mol Genet. 1994; 3:247–252. PMID: 8004090.
Article3. Mainardi PC, Pastore G, Castronovo C, Godi M, Guala A, Tamiazzo S, et al. The natural history of cri du chat syndrome. A report from the italian register. Eur J Med Genet. 2006; 49:363–383. PMID: 16473053.4. Solanki J, Gupta S, Arya A. Dental caries and periodontal status of mentally handicapped institutilized children. J Clin Diagn Res. 2014; 8:ZC25–ZC27.
Article5. Lim MA, Borromeo GL. The use of general anesthesia to facilitate dental treatment in adult patients with special needs. J Dent Anesth Pain Med. 2017; 17:91–103. PMID: 28879336.
Article6. Haywood PT, Karalliedde LD. General anesthesia for disabled patients in dental practice. Anesth Prog. 1998; 45:134–138. PMID: 10483384.7. Lim SW, So E, Yun HJ, Karm MH, Chang J, Lee H, et al. Analysis of the effect of oral midazolam and triazolam premedication before general anesthesia in patients with disabilities with difficulty in cooperation. J Dent Anesth Pain Med. 2018; 18:245–254. PMID: 30186971.
Article8. Park CH, Kim S. Survey of the sevoflurane sedation status in one provincial dental clinic center for the disabled. J Dent Anesth Pain Med. 2016; 16:283–288. PMID: 28879316.
Article9. Bersten AD, Rutten AJ, Vedig AE, Skowronski GA. Additional work of breathing imposed by endotracheal tubes, breathing circuits, and intensive care ventilators. Crit Care Med. 1989; 17:671–677. PMID: 2736929.
Article10. Asai T, Shingu K. Difficulty in advancing a tracheal tube over a fibreoptic bronchoscope: incidence, causes and solutions. Br J Anaesth. 2004; 92:870–881. PMID: 15121723.
Article11. Wang TK, Wu RS, Chen C, Chang TC, Hseih FS, Tan PP. Endotracheal tube size selection guidelines for chinese children: prospective study of 533 cases. J Formos Med Assoc. 1997; 96:325–329. PMID: 9170819.12. Inamoto Y, Saitoh E, Okada S, Kagaya H, Shibata S, Baba M, et al. Anatomy of the larynx and pharynx: effects of age, gender and height revealed by multidetector computed tomography. J Oral Rehabil. 2015; 42:670–677. PMID: 25892610.
Article
