Fibrin Clot Mistook as a Worm in the Intravenous Line
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. jy925@paik.ac.kr
- KMID: 2470925
- DOI: http://doi.org/10.3349/ymj.2020.61.3.267
Abstract
- There have been several reports of foreign bodies being discovered in the intravenous set. In this case, the patient complained that he found a worm in his intravenous line. It was later confirmed as a long, white fibrin deposit by pathologic examination. This happened even though there was a non-return valve in the intravenous line. Also, since there were few red blood cells in the deposit, it did not look like a blood clot. In cases like this, we suggest that physicians keep this possibility in mind to reassure their patients.
Figure
-
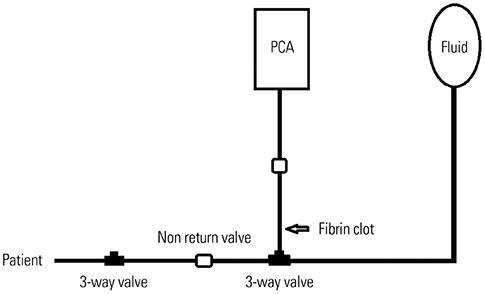
Fig. 1 The IV line pattern that was connected to the patient's body. White arrow indicates the location of fibrin clot. PCA, patient-controlled analgesia.

Fig. 2 White arrow indicates the fibrin clot found in the patient-controlled analgesia line.
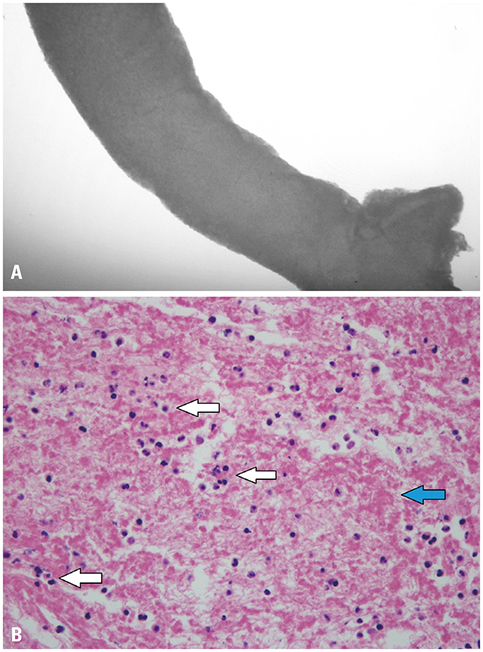
Fig. 3 (A) Microscopic finding of specimen before staining, ×40. (B) Hematoxylin and eosin (H&E) staining of a fibrin clot, ×400. Blue arrow shows dark pink amorphous material of fibrin. White arrows are indicating white blood cells such as leukocytes and lymphocytes. There are no red blood cells found in this view.
Cited by 1 articles
-
Ensuring patient safety: the importance of prompt pathological examination for foreign bodies in intravenous lines
Min Hee Heo, Sang Il Lee, Kyung Woo Kim, Jun Hyun Kim
Anesth Pain Med. 2023;18(4):445-446. doi: 10.17085/apm.23069.
Reference
-
1. Madsen H, Winding O. Release of foreign bodies (particles) by clinical use of intravenous infusion sets. Biomaterials. 1996; 17:663–666.
Article2. Yorioka K, Oie S, Oomaki M, Imamura A, Kamiya A. Particulate and microbial contamination in in-use admixed intravenous infusions. Biol Pharm Bull. 2006; 29:2321–2323.
Article3. Pathak K, Yadav D. Percutaneous removal of intracardiac and intravascular foreign bodies. Med J Armed Forces India. 2011; 67:367–369.
Article4. Gschwind CR. The intravenous foreign body: a report of 2 cases. J Hand Surg Am. 2002; 27:350–354.
Article5. Song M, Wei M, Song Z, Li L, Fan J, Liu M. A foreign body in the cephalic vein: a case report. Medicine (Baltimore). 2018; 97:e11144.6. Ellger B, Kiski D, Diem E, van den Heuvel I, Freise H, Van Aken H, et al. Non-return valves do not prevent backflow and bacterial contamination of intravenous infusions. J Hosp Infect. 2011; 78:31–35.
Article7. Rutherford J, Patri M. Failure of antireflux valve in a Vygon PCA set. Anaesthesia. 2004; 59:511.
Article8. Crosby E. Intravenous infusions and one-way valves. Can J Anaesth. 1991; 38:799–800.
Article9. Ambesh P, Ambesh SP. A simple technique to prevent reverse flow of blood from intravenous line in ipsilateral arm with noninvasive blood pressure cuff. J Clin Diagn Res. 2015; 9:UL01.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fibrin Clot Delivery System for Meniscal Repair
- The effect of autogenous fibrin clot on meniscal repair
- Meniscus Repair with Fibrin Clot in Complete Radial Tear of Lateral Meniscus
- A Case of a Large Fibrin Clot Formed in a Plama Unit Collected by Donor Plasmapheresis
- Arthroscopic Meniscal Repair using Fibrin Clot for Horizontal Tear in Young Adults: A Case Report
