Kinematically Aligned Total Knee Arthroplasty with Patient-Specific Instrument
- Affiliations
-
- 1Department of Orthopaedic Surgery, Konyang University College of Medicine, Daejeon, Korea.
- 2Department of Biomedical Engineering, University of California at Davis, Davis, CA, USA.
- 3Department of Orthopedic Surgery, Ajou University College of Medicine, Suwon, Korea. yeyeonwon@gmail.com
- KMID: 2470916
- DOI: http://doi.org/10.3349/ymj.2020.61.3.201
Abstract
- Kinematically aligned total knee arthroplasty (TKA) is a new alignment technique. Kinematic alignment corrects arthritic deformity to the patient's constitutional alignment in order to position the femoral and tibial components, as well as to restore the knee's natural tibial-femoral articular surface, alignment, and natural laxity. Kinematic knee motion moves around a single flexion-extension axis of the distal femur, passing through the center of cylindrically shaped posterior femoral condyles. Since it can be difficult to locate cylindrical axis with conventional instrument, patient-specific instrument (PSI) is used to align the kinematic axes. PSI was recently introduced as a new technology with the goal of improving the accuracy of operative technique, avoiding practical issues related to the complexity of navigation and robotic system, such as the costs and higher number of personnel required. There are several limitations to implement the kinematically aligned TKA with the implant for mechanical alignment. Therefore, it is important to design an implant with the optimal shape for restoring natural knee kinematics that might improve patient-reported satisfaction and function.
Keyword
Figure
-
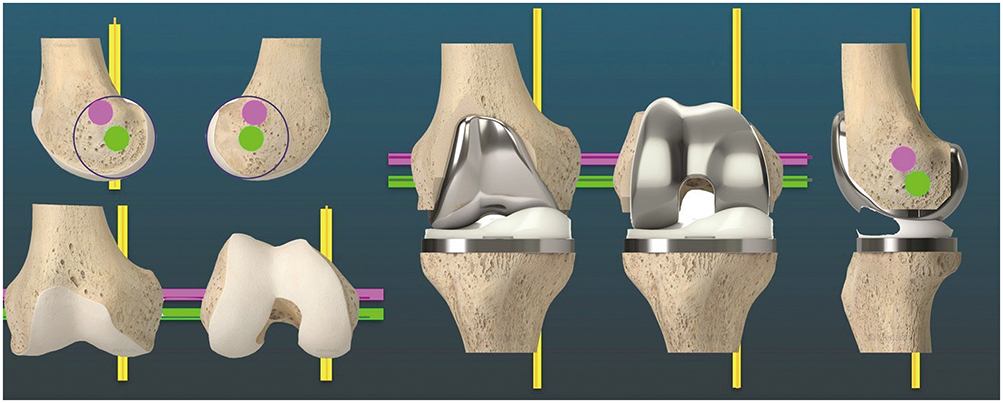
Fig. 1 The knee has three kinematic axes. Yellow line shows the longitudinal axis in the tibia that the tibia on the femur rotates about. In the femur, the green line shows transverse axes about which the tibia flexes and extends. Magenta line indicates the transverse axis of the femur that the patella flexes and extends about.
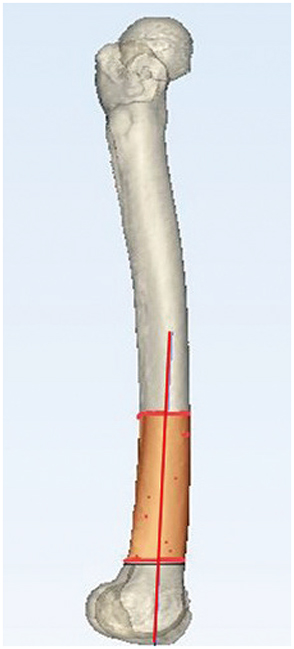
Fig. 2 From the upper margin, distal one-third to metaphyseal flare of the femur was registered with points by pen, which made a truncated cone. The distal femoral flexion axis was obtained as a line passing through the center of the truncated cone to the best fit.

Fig. 3 Preoperative determination of primary femoral axis. (A) Surfaces of each distal femoral condyle were marked from the distal portion in order to recess to posterior end of posterior condyles. (B) The best-fit sphere from each condyle was made from registered points, and putative positioning of sphere's center was equidistant from pre-arthritic articular surface. (C) Cylindrical axis was made by connecting the centers of two spheres.

Fig. 4 Preoperative determination of tibial alignment. (A) The registration process involved a surface centroid excluding regional bone defect and tibial spines. (B) Tibial resection was planned by the plane of best fit to both plateaus (overall arthritic plateau).

Fig. 5 Preoperative determination of guide pin location. (A) Patient-specific instrument (PSI) was manufactured by considering the distance between pin hole and saw slot of the cutting block. (B) PSI was applied to the three-dimensional (3D) model of the patient's tibia which was manufactured by 3D printer.
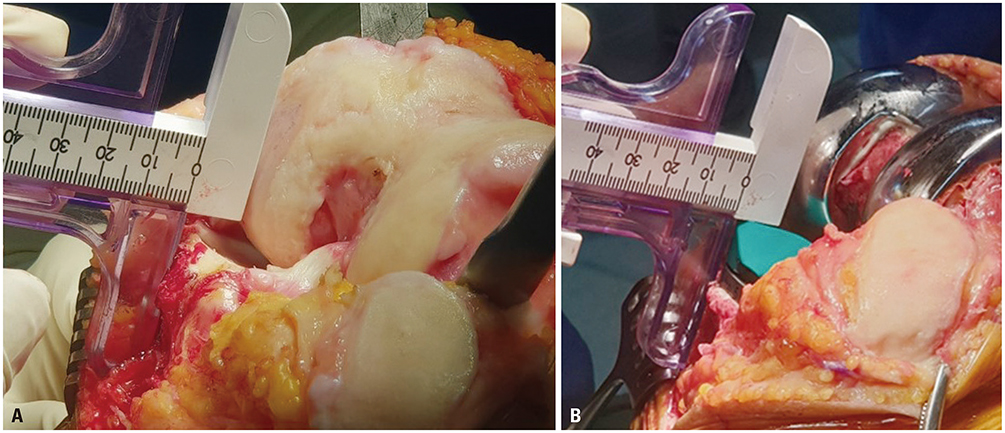
Fig. 6 Intra-operative measurement of anterior offset of the tibia from the femur. (A) Intra-operative images of a left knee with varus deformity in 90° of flexion demonstrate the measurement of anterior offset of the tibia from the worn distal medial articular surface of the femur. (B) In order to restore the slope of the native proximal tibial joint line, the anterior-posterior slope and thickness of the tibial component are adjusted until the anterior tibia offset from the distal medial femoral condyle matches that of the knee at the time of exposure.
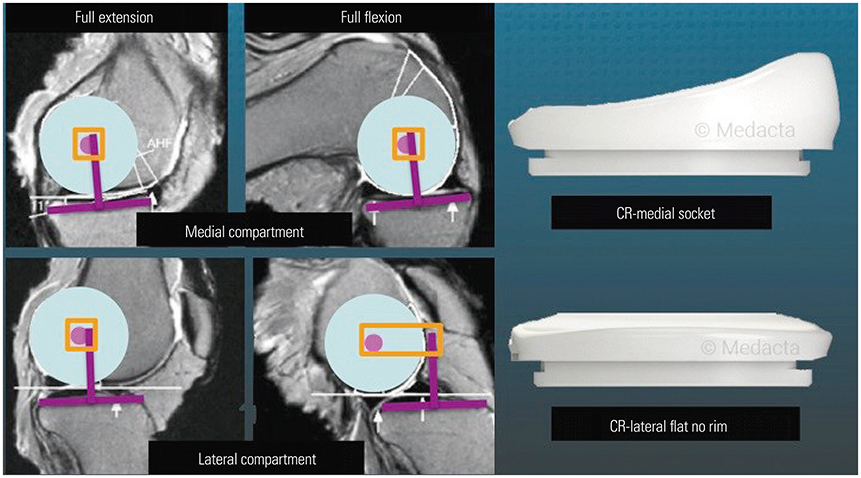
Fig. 7 This composite shows the tibiofemoral relationship of medial and lateral compartments of the native knee in full extension and full extension, in which medial femoral condyle hardly moves (orange square) and lateral femoral condyle rolls posterior in full flexion (orange rectangle). The design of cruciate retaining (CR) insert, consisting of a medial ball-and-socket and a lateral flat surface without a posterior rim, is a promising strategy for promoting A-P stability and reducing the risk of late tibial component failure from posterior rim wear of the insert.
Reference
-
1. Cherian JJ, Kapadia BH, Banerjee S, Jauregui JJ, Issa K, Mont MA. Mechanical, anatomical, and kinematic axis in TKA: concepts and practical applications. Curr Rev Musculoskelet Med. 2014; 7:89–95.
Article2. D'Lima DD, Hermida JC, Chen PC, Colwell CW Jr. Polyethylene wear and variations in knee kinematics. Clin Orthop Relat Res. 2001; (392):124–130.3. Sikorski JM. Alignment in total knee replacement. J Bone Joint Surg Br. 2008; 90:1121–1127.
Article4. Morgan SS, Bonshahi A, Pradhan N, Gregory A, Gambhir A, Porter ML. The influence of postoperative coronal alignment on revision surgery in total knee arthroplasty. Int Orthop. 2008; 32:639–642.
Article5. Baker PN, van der Meulen JH, Lewsey J, Gregg PJ. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J Bone Joint Surg Br. 2007; 89:893–900.6. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010; 468:57–63.
Article7. Niki Y, Nagai K, Sassa T, Harato K, Suda Y. Comparison between cylindrical axis-reference and articular surface-reference femoral bone cut for total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2017; 25:3741–3746.
Article8. Bonner TJ, Eardley WG, Patterson P, Gregg PJ. The effect of postoperative mechanical axis alignment on the survival of primary total knee replacements after a follow-up of 15 years. J Bone Joint Surg Br. 2011; 93-B:1217–1222.
Article9. Luyckx T, Vanhoorebeeck F, Bellemans J. Should we aim at undercorrection when doing a total knee arthroplasty? Knee Surg Sports Traumatol Arthrosc. 2015; 23:1706–1712.
Article10. Parratte S, Pagnano MW, Trousdale RT, Berry DJ. Effect of postoperative mechanical axis alignment on the fifteen-year survival of modern, cemented total knee replacements. J Bone Joint Surg Am. 2010; 92:2143–2149.
Article11. Vanlommel L, Vanlommel J, Claes S, Bellemans J. Slight undercorrection following total knee arthroplasty results in superior clinical outcomes in varus knees. Knee Surg Sports Traumatol Arthrosc. 2013; 21:2325–2330.
Article12. Lee SS, Lee H, Lee DH, Moon YW. Slight under-correction following total knee arthroplasty for a valgus knee results in similar clinical outcomes. Arch Orthop Trauma Surg. 2018; 138:1011–1019.
Article13. Magnussen RA, Weppe F, Demey G, Servien E, Lustig S. Residual varus alignment does not compromise results of TKAs in patients with preoperative varus. Clin Orthop Relat Res. 2011; 469:3443–3450.
Article14. Shelton TJ, Nedopil AJ, Howell SM, Hull ML. Do varus or valgus outliers have higher forces in the medial or lateral compartments than those which are in-range after a kinematically aligned total knee arthroplasty? Limb and joint line alignment after kinematically aligned total knee arthroplasty. Bone Joint J. 2017; 99-B:1319–1328.15. Miller EJ, Pagnano MW, Kaufman KR. Tibiofemoral alignment in posterior stabilized total knee arthroplasty: static alignment does not predict dynamic tibial plateau loading. J Orthop Res. 2014; 32:1068–1074.
Article16. Calliess T, Bauer K, Stukenborg-Colsman C, Windhagen H, Budde S, Ettinger M. PSI kinematic versus non-PSI mechanical alignment in total knee arthroplasty: a prospective, randomized study. Knee Surg Sports Traumatol Arthrosc. 2017; 25:1743–1748.
Article17. Waterson HB, Clement ND, Eyres KS, Mandalia VI, Toms AD. The early outcome of kinematic versus mechanical alignment in total knee arthroplasty: a prospective randomized control trial. Bone Joint J. 2016; 98-B:1360–1368.18. Dossett HG, Estrada NA, Swartz GJ, LeFevre GW, Kwasman BG. A randomised controlled trial of kinematically and mechanically aligned total knee replacements: two-year clinical results. Bone Joint J. 2014; 96-B:907–913.19. Nam D, Nunley RM, Barrack RL. Patient dissatisfaction following total knee replacement: a growing concern? Bone Joint J. 2014; 96-B:11 Supple A. 96–100.20. Young SW, Walker ML, Bayan A, Briant-Evans T, Pavlou P, Farrington B. The Chitranjan S. Ranawat Award: No difference in 2-year functional outcomes using kinematic versus mechanical alignment in TKA: a randomized controlled clinical trial. Clin Orthop Relat Res. 2017; 475:9–20.21. Howell SM, Howell SJ, Kuznik KT, Cohen J, Hull ML. Does a kinematically aligned total knee arthroplasty restore function without failure regardless of alignment category? Clin Orthop Relat Res. 2013; 471:1000–1007.
Article22. Howell SM, Papadopoulos S, Kuznik K, Ghaly LR, Hull ML. Does varus alignment adversely affect implant survival and function six years after kinematically aligned total knee arthroplasty? Int Orthop. 2015; 39:2117–2124.
Article23. Howell SM, Shelton TJ, Hull ML. Implant survival and function ten years after kinematically aligned total knee arthroplasty. J Arthroplasty. 2018; 33:3678–3684.
Article24. Howell SM, Kuznik K, Hull ML, Siston RA. Results of an initial experience with custom-fit positioning total knee arthroplasty in a series of 48 patients. Orthopedics. 2008; 31:857–863.
Article25. Klatt BA, Goyal N, Austin MS, Hozack WJ. Custom-fit total knee arthroplasty (OtisKnee) results in malalignment. J Arthroplasty. 2008; 23:26–29.
Article26. Weber W, Weber E. Section 4: On the knee. P Maquet R Furlong . Mechanics of the human walking apparatus. Berlin: Springer Verlag;1992. p. 75.27. Eckhoff DG, Bach JM, Spitzer VM, Reinig KD, Bagur MM, Baldini TH, et al. Three-dimensional mechanics, kinematics, and morphology of the knee viewed in virtual reality. J Bone Joint Surg Am. 2005; 87 Suppl 2:71–80.
Article28. Eckhoff D, Hogan C, DiMatteo L, Robinson M, Bach J. Difference between the epicondylar and cylindrical axis of the knee. Clin Orthop Relat Res. 2007; 461:238–244.29. Hollister AM, Jatana S, Singh AK, Sullivan WW, Lupichuk AG. The axes of rotation of the knee. Clin Orthop Relat Res. 1993; (290):259–268.
Article30. Iranpour F, Merican AM, Baena FR, Cobb JP, Amis AA. Patellofemoral joint kinematics: the circular path of the patella around the trochlear axis. J Orthop Res. 2010; 28:589–594.
Article31. Griffin FM, Math K, Scuderi GR, Insall JN, Poilvache PL. Anatomy of the epicondyles of the distal femur: MRI analysis of normal knees. J Arthroplasty. 2000; 15:354–359.32. Chan WP, Lang P, Stevens MP, Sack K, Majumdar S, Stoller DW, et al. Osteoarthritis of the knee: comparison of radiography, CT, and MR imaging to assess extent and severity. AJR Am J Roentgenol. 1991; 157:799–806.
Article33. Pfitzner T, Röhner E, Preininger B, Perka C, Matziolis G. Femur positioning in navigated total knee arthroplasty. Orthopedics. 2012; 35:10 Suppl. 45–49.
Article34. Ensini A, Timoncini A, Cenni F, Belvedere C, Fusai F, Leardini A, et al. Intra- and post-operative accuracy assessments of two different patient-specific instrumentation systems for total knee replacement. Knee Surg Sports Traumatol Arthrosc. 2014; 22:621–629.
Article35. Nedopil AJ, Howell SM, Hull ML. What clinical characteristics and radiographic parameters are associated with patellofemoral instability after kinematically aligned total knee arthroplasty? Int Orthop. 2017; 41:283–291.
Article36. Kim K, Kim J, Lee D, Lim S, Eom J. The accuracy of alignment determined by patient-specific instrumentation system in total knee arthroplasty. Knee Surg Relat Res. 2019; 31:19–24.
Article37. Howell SM, Howell SJ, Hull ML. Assessment of the radii of the medial and lateral femoral condyles in varus and valgus knees with osteoarthritis. J Bone Joint Surg Am. 2010; 92:98–104.
Article38. Johnson JM, Mahfouz MR, Midilliogğlu MR, Nedopil AJ, Howell SM. Three-dimensional analysis of the tibial resection plane relative to the arthritic tibial plateau in total knee arthroplasty. J Exp Orthop. 2017; 4:27.
Article39. Nedopil AJ, Howell SM, Hull ML. What mechanisms are associated with tibial component failure after kinematically-aligned total knee arthroplasty? Int Orthop. 2017; 41:1561–1569.
Article40. Ikeuchi M, Yamanaka N, Okanoue Y, Ueta E, Tani T. Determining the rotational alignment of the tibial component at total knee replacement: a comparison of two techniques. J Bone Joint Surg Br. 2007; 89:45–49.41. Coughlin KM, Incavo SJ, Churchill DL, Beynnon BD. Tibial axis and patellar position relative to the femoral epicondylar axis during squatting. J Arthroplasty. 2003; 18:1048–1055.
Article42. Akagi M, Matsusue Y, Mata T, Asada Y, Horiguchi M, Iida H, et al. Effect of rotational alignment on patellar tracking in total knee arthroplasty. Clin Orthop Relat Res. 1999; (366):155–163.
Article43. Rhoads DD, Noble PC, Reuben JD, Mahoney OM, Tullos HS. The effect of femoral component position on patellar tracking after total knee arthroplasty. Clin Orthop Relat Res. 1990; (260):43–51.
Article44. Steinbrück A, Schröder C, Woiczinski M, Fottner A, Müller PE, Jansson V. The effect of trochlea tilting on patellofemoral contact patterns after total knee arthroplasty: an in vitro study. Arch Orthop Trauma Surg. 2014; 134:867–872.
Article45. Rivière C, Iranpour F, Harris S, Auvinet E, Aframian A, Parratte S, et al. Differences in trochlear parameters between native and prosthetic kinematically or mechanically aligned knees. Orthop Traumatol Surg Res. 2018; 104:165–170.
Article46. Ishikawa M, Kuriyama S, Ito H, Furu M, Nakamura S, Matsuda S. Kinematic alignment produces near-normal knee motion but increases contact stress after total knee arthroplasty: a case study on a single implant design. Knee. 2015; 22:206–212.
Article47. Anouchi YS, Whiteside LA, Kaiser AD, Milliano MT. The effects of axial rotational alignment of the femoral component on knee stability and patellar tracking in total knee arthroplasty demonstrated on autopsy specimens. Clin Orthop Relat Res. 1993; (287):170–177.
Article48. Incavo SJ, Schmid S, Sreenivas K, Ismaily S, Noble PC. Total knee arthroplasty using anatomic alignment can produce mid-flexion laxity. Clin Biomech (Bristol, Avon). 2013; 28:429–435.
Article49. Freeman MA, Pinskerova V. The movement of the normal tibiofemoral joint. J Biomech. 2005; 38:197–208.
Article50. French SR, Munir S, Brighton R. A single surgeon series comparing the outcomes of a cruciate retaining and medially stabilized total knee arthroplasty using kinematic alignment principles. J Arthroplasty. 2020; 35:422–428.
Article51. Schütz P, Taylor WR, Postolka B, Fucentese SF, Koch PP, Freeman MA, et al. Kinematic evaluation of the GMK sphere implant during gait activities: a dynamic video fluoroscopy study. J Orthop Res. 2019; 37:2337–2347.
Article52. Nicolet-Petersen S, Saiz A, Shelton T, Howell SM, Hull ML. Small differences in tibial contact locations following kinematically aligned TKA from the native contralateral knee. Knee Surg Sports Traumatol Arthrosc. 2019; 08. 13. DOI: 10.1007/s00167-019-05658-1. [Epub]. Available at: .
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kinematically Aligned Oxford Unicompartmental Knee Arthroplasty Using the Microplasty Instrumentation System
- Accuracy of Patient-Specific Instrument for Cylindrical Axis Implementation in Kinematically Aligned Total Knee Arthroplasty
- The Accuracy of Alignment Determined by Patient-Specific Instrumentation System in Total Knee Arthroplasty
- Isolated Posterior Malleolar Fracture of Ankle Occurring with Total Knee Arthroplasty in Severe Osteoporotic Patient
- Staged Reimplantation Using Cement Spacer Containing Antibiotics in Infected Total Knee Arthroplasty
